Video Presentation | DOI: https://doi.org/10.31579/2641-0419/224
1 Cardiothoracic Centre, All India Institute of Medical Sciences, New Delhi
2 Department of Cardiothoracic and Vascular Surgery, All India Institute of Medical Sciences, Bilaspur, Himachal Pradesh
*Corresponding Author: Ujjwal Kumar Chowdhury, Professor Department of Cardiothoracic and Vascular Surgery AIIMS, New Delhi 110029, INDIA
Citation: Ujjwal Kumar Chowdhury, Niwin George , Lakshmi Kumari Sankhyan , Shikha Goja , Sumanth Raghuprakash., et all (2021). Technical Details of Redo Aortic Valve Replacement using St. Jude Medical Mechanical Prosthesis in a Patient with Thrombosed Aortic Mechanical Prosthesis: A Video Presentation. J. Clinical Cardiology and Cardiovascular Interventions, 4(18); DOI:10.31579/2641-0419/224
Copyright: © 2021 Ujjwal Kumar Chowdhury, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 September 2021 | Accepted: 19 November 2021 | Published: 29 November 2021
Keywords: redo aortic valve; femoral arterio-venous cannulation prior; echocardiographically
Current consensus guidelines of the AHA and ESC, uniformly recommend either type of prosthetic valve for patients aged 60 to 70 years and mechanical prosthesis for patients aged less than 60 years
Current consensus guidelines of the AHA and ESC, uniformly recommend either type of prosthetic valve for patients aged 60 to 70 years and mechanical prosthesis for patients aged less than 60 years. [1-4] These recommendations are based on the results of 4 randomized controlled trials that demonstrated no significant difference in late survival. [2-6] Two of these trials compared mechanical and bioprosthetic valve models implanted in 1970s and 1980s. [5-7] The other 2 trials included patients undergoing aortic valve replacement. Contemporary data are limited to small single center studies. [1,2,8-10]
Valve replacement in young adults entails a choice between a mechanical prosthesis with risks of anticoagulation-related bleeding/thrombosis versus bioprosthesis necessitating eventual reoperation.
Despite usage of carbon pyrolite and central flow design of St. Jude Medical mechanical prosthetic valve, thromboembolism and anticoagulant induced haemorrhage after surgery continue to account for 75% of all valve-related complications. [11,12]
Thrombolysis of thrombosed St. Jude mechanical valves is safe and is the preferred first choice of treatment in the absence of other contraindications for anticoagulation. [11-15] Cinefluoroscopy is the preferred method for diagnosis and follow-up of St. Jude thrombosis in our institution. [11] Doppler echocardiography and cinefluoroscopy have complimentary role in assessing prosthetic valve function during thrombolytic therapy. [5-8,16-19]
Patients who do not respond within 48-72 hours should be referred for surgery because these patients may have tissue ingrowth obstructing the prosthetic valve (Panus formation) and usually do not respond to continued thrombolytic treatment. Explantation of the prosthetic valves during redo surgical procedures present formidable surgical challenges in many instances.
We present here-in a 48 year-old male patient diagnosed to have a chronic thrombosed St. Jude Medical aortic valve prosthesis, with failed thrombolysis, who underwent explantation of the thrombosed aortic prosthesis and re-replacement of the mitral valve using another 21mm St. Jude Medical mechanical prosthesis. The technical details of explantation and re-replacement procedure without causing injury to the cardiac chambers, and great vessels have been discussed in detail. Postoperative recovery was uneventful.
Following systemic heparinisation, elective right femoral arteriovenous cannulation is done using long femoral arterial and venous cannulae (Edwards Lifesciences LLC, One Edwards Way, Irvine, CA, USA).
Under cardiopulmonary bypass, secondary median sternotomy is performed with the heart decompressed on bypass. The pericardium overlying the aorta, right ventricular outflow tract and superior vena cava is dissected.
An 18-Fr sump suction vent is placed over the main pulmonary artery for further decompression of the heart to facilitate dissection. The superior caval vein is being dissected and cannulated directly using an angled metal tipped venous cannula and drained directly into the oxygenator. The intrapericardial inferior caval vein is dissected and looped for later occlusion.
After aortic cross-clamping, an oblique horse-shoe shaped aortotomy was performed in between stay sutures 1.5 cm above the sinus of the right coronary artery stopping about 1 cm above the midpoint of the non-coronary sinus. Myocardial protection was achieved by integrated myocardial protection using direct ostial St. Thomas (II) based cold blood cardioplegia (4:1) and topical cardiac cooling using ice cold saline. Successive doses of cardioplegia were repeated every 30 minutes.
Two stay sutures of 2-0 Ethibond (Johnson and Johnson Ltd., Ethicon, LLC, San Lorenzo, USA) are placed over the prosthetic mitral annulus to facilitate later explantation of the aortic prosthesis.
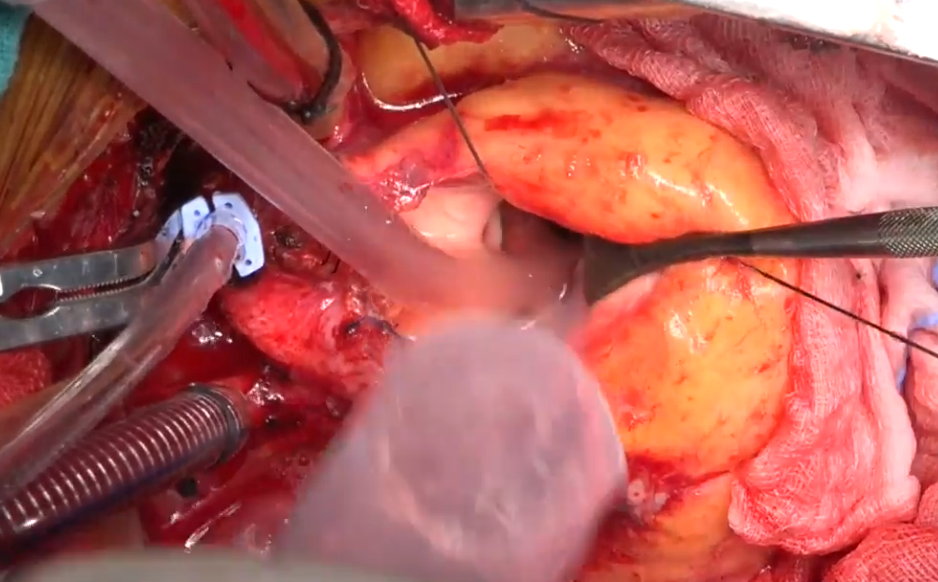
An incision is made on the aortic prosthetic ring using a No.11 scalpel blade. The prosthetic valve is detached from the aortic annulus by a combined sharp and blunt dissection.
A small right angle forceps is insinuated within the opening to facilitate explantation of the aortic prosthesis. The prosthetic valve is explanted by incising the prosthetic fibrous capsule on both aortic and ventricular surface. Extreme precautions are taken not to cause aorto ventricular discontinuity. Precautions are also taken not to dislodge the thrombus contained within the prosthetic mitral valve.
Re-replacement of the mitral valve is done using a 21 mm St. Jude mechanical aortic prosthesis (St. Jude Medical; St Jude Medical; St. Paul, MN, USA) and interrupted 2-0 Ethibond mattress suture. The aortotomy is closed in two layers using 4-0 polypropylene sutures (Johnson and Johnson Ltd., Ethicon, LLC, San Lorenzo, USA).
The patient was weaned off cardiopulmonary bypass on dopamine 5µg/kg/min and nitriglycerine 0.5 µg/kg/min. He was extubated after 6 hours. At 12 months follow-up, he is in New York Heart Association functional class I with left ventricular ejection fraction of 0.60, in normal sinus rhythm. Echocardiographically, the mean systolic left ventricle-to-aortic pressure gradient was 8 mmHg, no aortic regurgitation and there was no paravalvular / cuff leakage.
Elective institution of cardiopulmonary bypass through femoro-femoral arterio-venous cannulation prior to sternotomy prevents accidental injury to the cardiac chambers and great vessels during sternal entry. Pulmonary artery venting and cannulation of the superior vena cava further facilitates dissection of the cardiac chambers without causing injury. Placement of two stay sutures on the prosthetic annulus and intracapsular dissection greatly facilitates explantation without causing aorto ventricular discontinuity.
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of the article.
The authors received no financial support for the research, authorship and/or publication of this article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,