
Case Report | DOI: https://doi.org/10.31579/2641-0419/404
1Department of Cardiology, Sikasso Hospital, Mali.
2UFR of Medicine, University of Western Brittany, France.
3Department of Otorhinolaryngologie, Sikasso Hospital, Mali.
4Department of Pediatrics, Sikasso Hospital, Mali.
5Department of Radiology, Sikasso Hospital, Mali.
6Biology laboratory (BioSik), Sikasso, Mali.
*Corresponding Author: Cénac Arnaud, UFR of Medicine, University of Western Brittany, Brest, France.
Citation: Traore K. Abdoulaye, Cénac Arnaud, Dembele Ahmadou, Cissouma Assetou, Haidara Ousmane, et al, (2024), Tamponade revealing purulent pericarditis caused by Klebsiella pneumoniæ and Escherichia coli. Clinical cure by drainage and antibiotic therapy. Sikasso (Mali), Journal of Clinical Cardiology and Cardiovascular Interventions, 7(10); DOI:10.31579/2641-0419/404
Copyright: © 2024, Cénac Arnaud. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 August 2024 | Accepted: 23 September 2024 | Published: 30 September 2024
Keywords: tamponade; purulent pericarditis; klebsiella pneumoniæ; escherichia coli
The authors report the observation of a 52-year-old Malian patient living in Sikasso (Mali), hospitalized urgently for febrile condition with arterial hypotension. The diagnosis of tamponade is made by echocardiography. Drainage of the pericardial effusion quickly improves the hemodynamic status and reveals purulent fluid. Microbiological analysis of the liquid identifies 2 different, associated pathogenic bacteria: Escherichia coli and Klebsiella pneumoniæ. Treatment with Imipenem (2 g/day by venous infusion) for 21 days leads to healing. Thirty-six months later the patient is in a stable state of clinical recovery. The authors did not find in the literature any purulent pericarditis with the 2 bacteria identified here, associated.
Purulent pericarditis, apart from tuberculosis, is rare [1]. The observation reported is a purulent pericarditis where 2 associated pathogenic bacteria were isolated, an association not previously described.
Clinical history. A 52-year-old black Malian man living in Sikasso was hospitalized in January 2021 for febrile chest pain with dry cough and edema of the lower limbs. The clinical examination data are:
Height = 1.86 m Weight = 65 kg
Respiratory rate =22 cycles/min
Chest distensionBilateral crackling rattles
Unperceived peak shock
Low blood pressure: right arm = 90/50 mmHg
left arm = 80/50 mmHg
Hepatomegaly with jugular turgor
Hepatojugular reflux
Peripheral pulses weakly felt
ECG: sinus rhythm at 98/min, diffuse repolarization disorders such as “Holzmann stage 1 pericarditis”.
Frontal chest x-ray: very enlarged cardiac shadow (cardiothoracic ratio = 0.8), basal opacity of the left lung field, barely visible recess of pleura (pleural effusion?) (Figure 1).
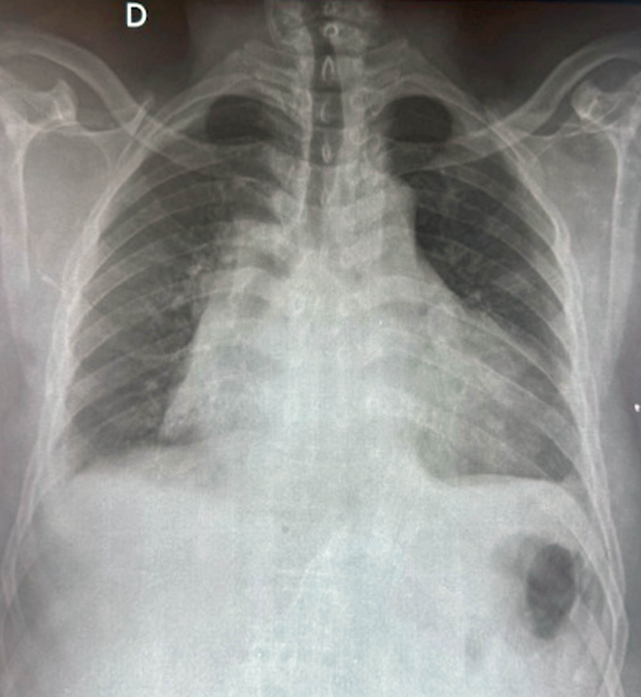
Figure 1 : Frontal chest radiograph. Cardiothoracic ratio = 0.8.
Echocardiography: demonstration of a large pericardial effusion with a “swinging heart” appearance. Left and right systolic functions are preserved but the diastole of the right ventricle is of low amplitude, a sign of tamponade (figure 2).
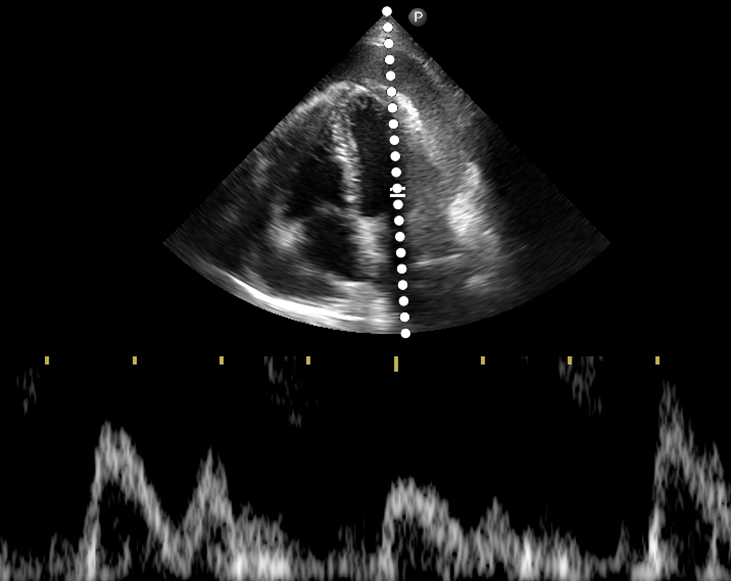
Figure 2 : Ultrasound before puncture (apical section of the 4 cavities): large pericardial effusion and significant variations in flow, signs of poor tolerance (tamponade).
Biological results: anemia with hemoglobin at 10 g/dL and hematocrit at 35.5%, red blood cells = 4.42 million/mm3, leukocytosis at 26,400/mm3 with 82% neutrophils, platelets = 245,000/mm3C reactive protein = 50 mg/L Fasting blood sugar = 1 g/L Creatinine = 18 mg/LThe pericardial puncture brings back a brown, cloudy fluid with a purulent appearance. On direct examination under the microscope, the number of leukocytes per field is greater than 500, with 90% neutrophils and 10% lymphocytes. The culture makes it possible to isolate 2 pathogenic bacteria, Escherichia coli and Klebsiella pneumoniae and to establish an antibiogram. Both bacteria are sensitive to several antibiotics: Imipeneme, Kanamycin, Amikacin, etc.Treatment and evolution. The diagnosis of purulent pericarditis complicated by tamponade was made. High-flow oxygen therapy is installed and an ultrasound-guided pericardial puncture is performed. An hour later, a new ultrasound examination reveals the virtual disappearance of the effusion (figure 3) and signs of tamponade. Antibiotic treatment with Imipeneme is undertaken at a dose of 2 g/day, intravenously, for 21 days, under monitoring of renal function. At the end of this treatment, the clinical, biological and ultrasound assessments confirm healing. After several months (up to 36 months), the patient's condition is stable, without relapse.
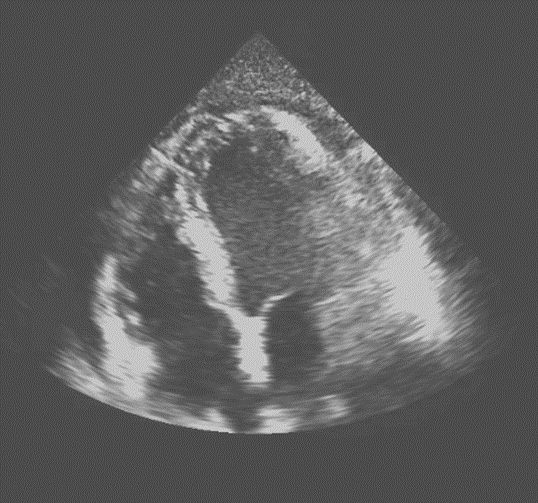
Figure 3: Ultrasound after puncture (apical section of the 4 cavities): small pericardial effusion coinciding with a spectacular clinical improvement
Purulent pericarditis is a serious, life-threatening infection [1]. Having become rare in Europe (< 1 href="%">percentage of causes of pericarditis) [2]. When the diagnosis is considered during a tamponade, it is a vital emergency [3]. The contribution of echocardiography to making the diagnosis of pericardial effusion with tamponade is then decisive [3]. As for the pathogens responsible, several have been reported but are rare apart from the tuberculosis bacillus [2]. Thus Klebsiella pneumoniæ is found responsible for purulent pericarditis in a patient undergoing hemodialysis [4], in a Nigerian child [5], in a 44-year-old Chinese woman infected with a lethal hyper-virulent form [6], in a Colombian [7]. The responsibility of Escherichia coli seems exceptional; we found only one observation in the medical literature [8]. As for the question of a Klebsiella pneumoniæ-Escherichia coli double infection, no case is reported in the literature accessible on the databases.
This clinical case demonstrates for the first time the possibility of a bacterial association in a purulent pericarditis.
No conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
