
Case Report | DOI: https://doi.org/10.31579/2641-0419/121
1Division of Cardiovascular Diseases, Creighton University School of Medicine, Omaha, NE, USA
2Division of Internal Medicine, Creighton University School of Medicine, Omaha, NE, USA
*Corresponding Author: Abhishek Thandra, Division of Cardiovascular Diseases Creighton University School of Medicine, 7500 Mercy Rd Suite 301, Omaha, NE, 68124
Citation: Abhishek Thandra., Raahat Bansal., Tarun Tandon., Ann Narmi., (2021) Taking over the Territory: A Case of Superdominant Right Coronary Artery. J. Clinical Cardiology and Cardiovascular Interventions, 4(4); Doi:10.31579/2641-0419/121
Copyright: © 2021 Abhishek Thandra, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 December 2020 | Accepted: 02 March 2021 | Published: 11 March 2021
Keywords: left circumflex artery; super-dominant; right coronary artery
Coronary artery anomalies are a diverse group of congenital disorders, with a reported incidence of 0.6 – 1.3%. Congenital absence of the LCX is an extremely rare anomaly, with a frequency of only 0.003% in all patients who undergo coronary angiography. Here, we present a case of 76-year-old female who had an episode of chest pain while she was hospitalized for management of small bowel obstruction with elevated troponin and coronary angiogram showed super-dominant right coronary artery without any obstructive disease.
Running Title: Congenital absence of left circumflex artery
LCX=left circumflex artery
RCA=right coronary artery
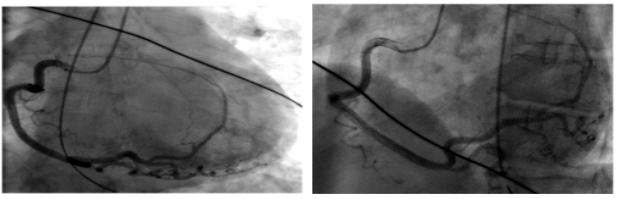
A 76-year-old femalse with history of hypertension, diabetes mellitus type 2, and hyperlipidemia was admitted with a diagnosis of small bowel obstruction and managed conservatively. During her hospitalization, she complained of chest pressure. Initial evaluation included a physical examination and electrocardiogram, which were unremarkable. Troponin I peaked at 3.94 ng/ml (≤0.04 ng/ml). Her Echocardiogram demonstrated apical segment akinesis with an ejection fraction of 30%. Coronary angiogram showed no angiographic evidence of coronary artery disease. However, the left circumflex artery (LCX) artery did not originate from the left main coronary artery. Rather, the super-dominant right coronary artery (RCA) had a large postero-lateral branch, which occupied the atrio-ventricular groove and supplied the lateral wall of the myocardium (Figure 1, Figure 2a, 2b and 2c).

Coronary artery anomalies are a diverse group of congenital disorders, with a reported incidence of 0.6 – 1.3%. [1] Congenital absence of the LCX is an extremely rare anomaly, with a frequency of only 0.003% in all patients who undergo coronary angiography [1]. With absence of LCX, the lateral wall of the left ventricle is mostly supplied by a super-dominant RCA (90% of the time) or occasionally by a multiple diagonal branch of LAD [2,3]. On literature review, super-dominant RCA is always associated with an absent LCX. Considered to be a benign anomaly, a few cases have reported its association with systolic click syndrome, ischemic changes in the zone of hypoperfusion, heart failure, and syncope [3,4]. Coronary angiogram or coronary CTA are used for definitive diagnosis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
