
Case Report | DOI: https://doi.org/10.31579/2690-4861/025
*Corresponding Author: Deepanjan Bhattacharya, Senior Resident, Department of Paediatrics, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
Citation: Deepanjan B,Mounam C. (2020) Systemic Thromboembolisation as an Uncommon Manifestation of Dilated Cardiomyopathy in Sinus Rhythm. International Journal of Clinical Case Reports and Reviews. 2(4); DOI: 10.31579/2690-4861/025
Copyright: © 2020 Deepanjan Bhattacharya, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 May 2020 | Accepted: 18 June 2020 | Published: 24 June 2020
Keywords: sinus rhythm; exertional dyspnea; alcohol or tobacco; left ventricular hypertrophy
Systemic thromboembolism in cases with dilated cardiomyopathy in sinus rhythm has been rarely described. We report a middle-aged man, who had splenic as well as cerebral thromboembolism, with a background of dilated cardiomyopathy in sinus rhythm.
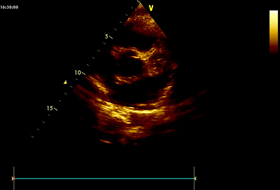
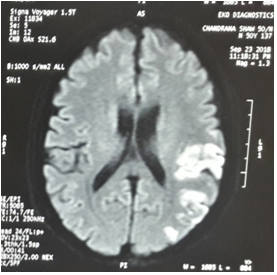
A 40 year old man presented with severe pain localized to the left upper abdomen for the past 7 days, which was dull aching, and not associated with vomiting, dysphagia or heartburn. At the time of admission, he developed sudden onset right sided complete hemiparesis. He had a history of progressive exertional dyspnea for the last 6 months, which was partially controlled by oral medications. There was no history of similar episode in the past, seizure, loss of consciousness, jaundice or previous abdominal surgery. There was no family history of similar illness, and he denied consumption of alcohol or tobacco. On examination, he was alert and co-operative, with stable vitals (pulse rate – 90 per minute, regular, blood pressure – 100/70 mm Hg, respiratory rate – 14 per minute, regular). Systemic examination revealed diffuse tenderness over the left hypochondrium, apex beat shifted downwards and outwards, and normally heard heart sounds. Neurological examination was suggestive of left sided facial nerve weakness (upper motor neuron type), left hemiplegia with extensor plantar response, without any evidence of raised intracranial pressure. Complete blood count, renal and liver function tests were within normal limits. 12 lead electrocardiogram was suggestive of left axis deviation, left ventricular hypertrophy and non-specific ST segment changes in left precordial leads. Chest X ray showed cardiomegaly with blunting of bilateral costophrenic angles.Transthoracic echocardiography showed dilated cardiac chambers (left ventricular end diastolic dimension – 58 mm), global hypokinesia with ejection fraction of 22%. No clots or vegetations could be identified (Figure 1A and B).

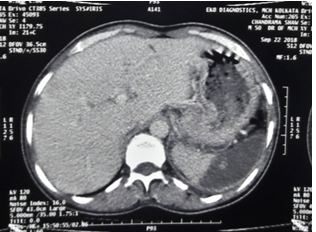
Ultrasound of the abdomen showed mild hepatomegaly, dilated inferior vena cava with loss of respiratory variation, bilateral mild pleural effusion, and peripheral wedge shaped hypoechoic lesion in the spleen, which was confirmed to be an infarct of computed tomography (Figure 2A).
Coagulation profile was normal. Prothrombotic workup was also normal, with negative anti-phospholipid workup.Warfarin was initiated for thromboembolism, with a target International Normalized Ratio (INR) of 2.5. He was continued on diuretics and ramipril for cardiomyopathy, and started on comprehensive neuro-rehabilitation. At followup after 3 months, he has minimal residual neurological weakness and controlled heart failure with functional class II.
DISCUSSION
Although there are several reports of thromboembolism in patients with dilated cardiomyopathy, [1] [2] those with the patient in sinus rhythm is extremely rare. Simultaneous demonstration of evidence of two distant sites of systemic embolization (here brain and spleen) has been hardly reported in scientific articles. Intramural thrombi are rarely demonstrable on echocardiography after embolization, hence it should not preclude initiation of anticoagulation. [3]. There is no consensus regarding the use of anticoagulation in those with reduced LV function in sinus rhythm, but the risk of thromboembolism is incontrovertible. Since the risk further increases with initiation of diuretics, one must be careful and prefer early initiation of anticoagulation [4].
DECLARATION
Conflicts of interest: none
Funding: None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
