
Review Article | DOI: https://doi.org/10.31579/2690-4861/128
*Corresponding Author: Akshay Mehta, Department of Paediatric Cardiology Southampton General Hospital, Southampton, United Kingdom.
Citation: A Mehta, B Malik, Z Smith. (2021) Synopsis on Non-invasive Ventilation in Neonatology. International Journal of Clinical Case Reports and Reviews. 7(4); DOI: 10.31579/2690-4861/128
Copyright: © 2021 Akshay Mehta, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 March 2021 | Accepted: 28 June 2021 | Published: 02 July 2021
Keywords: heated humidified high flow nasal cannula; nasal continuous positive airway pressure; nasal intermittent positive pressure ventilation; noninvasive ventilation; preterm infants
Non-invasive ventilation (NIV) is a mode of respiratory support commonly used on the neonatal unit. Since the advent of NIV, it has evolved from being used as a mode of respiratory support to wean infants from mechanical ventilation (MV) to a primary mode of respiratory support. NIV improve the functional residual capacity in the newborn (at term or preterm) avoiding invasive actions such as tracheal intubation. Newer methods of NIV support such as nasal bilevel positive airway pressure (BiPAP) and humidified high flow nasal cannula oxygen therapy (HHFNC) have emerged in attempts to reduce intubation rates and subsequent MV in preterm infants. With this synopsis, we aim to discuss various available NIV modes of ventilation in Neonatology, including indications, physiological principle, practical aspects and effects on important short and long-term morbidities associated with the use of NIV.
Invasive Mechanical Ventilation (IMV) has been the primary treatment in Respiratory distress Syndrome (RDS) for Very low birth weight babies (VLBW). Although lifesaving, IMV is an important risk factor in developing Broncho pulmonary dysplasia (BPD) and its related complications [1].
Affected infants require comprehensive medical followup and treatment after hospital discharge with frequent hospital readmissions, home based oxygen therapy, treatment for pulmonary hypertension, these factors thus significantly affect quality of life of affected infants [2].
Despite advances in neonatal medicine, such as improved antenatal care, antenatal corticosteroids and surfactant administration; there hasn’t been significant fall in incidence of BPD in last decade [3].
IMV causes volutrauma, barotrauma, inflammatory mediated alveolar and vascular destruction resulting in progressive impaired gas exchange. To alleviate the harmful effects of IMV on the premature lungs, nasal CPAP was introduced as a non-invasive ventilation strategy. CPAP was first used clinically in 1971, CPAP significantly reduced the need for IMV, but failure rates of almost 50% have prompted for seeking more effective NIV modalities [4, 5].
There are various non-invasive ways in which respiratory support can be provided to neonates with parenchymal lung disease or apnoea viz heated humidified high flow nasal cannula (HHHFNC), Continuous Positive Airway Pressure (CPAP), Nasal Intermittent Positive Pressure Ventilation (NIPPV).
Heated Humidified High Flow Nasal Cannula (HHHFNC)
HHHFNC is commonly used in most NICUs throughout the world. It is a flow based non-invasive respiratory support which delivers heated and humidi- fied gas.
Oxygen delivered by “low flow” nasal cannula (LFNC) typically refers to the use of flow rates of less than or equal to 1-2 L/minute. Usually the gas used is unblended (i.e.100% oxygen), unheated and non-humidified. LFNC is used commonly in growing convalescent preterm infants (often with chron- ic lung disease). In contrast, “high flow” nasal cannula (HFNC) has been used to refer to the administration of oxygen or blended oxygen/air to new born infants via nasal cannula at higher flow rates than LFNC. The use of devices providing use of humidified high flow by nasal cannula (HFNC) to these babies has increased dramatically over last few years due to relative simplicity of its use and user friendly nature [6]. Most commonly it is used for babies recovering from RDS on low pressure nCPAP and FiO2 and who would traditionally undergo a period of cycling nCPAP regimen before discontinuing respiratory support. Anecdotally, HFNC allows infant to be handled less, makes easier to receive kangaroo care and breast feeding than nCPAP. The clinical role of HFNC is still evolving and further controlled clinical trials are needed to identify which infants benefit most from HFNC. Despite its popularity, the use of HFNC should not be extended as a routine replacement for nCPAP until further large randomised controlled trials comparing efficacy and safety are published and the unit gains enough ex- perience using it on stable babies [7].
Physiological Principles of HFNC (8)
1. Washout of Naso-pharangeal dead space
2. Reduces respiratory resistance and hence decreases work of breathing
3. Provides continuous distending pressure; pharyngeal pressure provided is directly related to flow but inversely related to infant size.
4. Respiratory gas conditioning; improves lung and airway mechanics by eliminating the effect of drying/cooling.
Differences from nCPAP
HFNC should not be regarded as a form of nCPAP. Rather, it is a distinct respiratory support modality that should be assessed on its own merits in the same way as for other modalities of ventilation.
nCPAP has been shown to reduce extubation failure, treat apnoea and respiratory distress syndrome, and may reduce chronic lung disease by minimising duration of mechanical ventilation. Oxygen administered by nCPAP is usually blended, humidified and heated. Contrary to HFNC, the pressure delivered by the circuit for nCPAP is measured and regulated directly. The use of binasal prongs to deliver nCPAP can be associated with trauma to the nasal septum and distortion of the nares. Difficulties with successful application of nCPAP are principally related to the bulky interface with the patient leading to problems maintaining proper position and effectiveness. It also is less patient friendly making handling and feeding more difficult while on nCPAP [9].
In contrast, HFNC provides blended, heated, humidified oxygen at flow rates higher than the patient’s inspiratory flow rate thereby reducing work of breathing and ensuring that intended oxygen concentration is delivered. If prongs are selected properly, HFNC is an open system potentially reduc- ing the risk of baro/volutrauma and reducing nasal mucosal damage. It cre- ates a flow related variable distending pressure delivered to the neonates upper airway and lungs that unlike CPAP is unmeasurable in clinical practice. Adult studies suggest it provides low PEEP, improves mucosal perfusion and stimulates respiratory drive. The interface is less bulky, allowing easy access for parents and nurses for handling and feeding purposes. [10, 11]
Possible Risks
Concerns that have been expressed include increased risk of infection (Vapotherm only), excessive airway pressure generation (avoid a tight fit nasal prong) and local trauma (avoid a tight fit nasal prong)
Indications for use
No formal recommendations are available for specific clinical indications published. Collectively published studies suggest a wide potential role for HFNC in respiratory care of the neonate.
Consider HFNC on:
• Stable babies recovering from RDS or with chronic lung disease
• FiO2 ≤ 30%
• Ready to be cycled off on nCPAP at a pressure of 5cm H20 or lower.
• No significant apnoea, desaturations or bradycardia requiring frequent stimulation. These set of babies are likely to benefit from HFNC as weaning will be more physiological, and user friendly.
Relative Contraindications:
• Should not be used on babies where a suitable loose fit nasal cannula is not available (extremely small nares). Avoid tight fit nasal cannula at all cost
• Use judgment for babies with significant CLD. This may take some experience
• Not to be considered for babies who can be taken off nCPAP to air directly i.e. stable term/ near term babies.

Nasal CPAP- Nasal Continuous Positive Airway Pressure
CPAP aims to prevent alveolar collapse at end expiration. It is used for infants with moderate respiratory distress and for recurrent apnoeas. It is also used for weaning from mechanical ventilation. Use of early CPAP has significantly reduced the need for invasive ventilation and surfactant administration in preterms [12, 13].
Physiological principle:
1. Provides continuous distending pressure to maintain functional residual capacity (FRC) –reduction of airway collapse by decreased airway resistance and reduces work of breathing
2. Splints the pharyngeal airway to avoid obstruction
3. Keeps the surfactant on alveolar surface and thus promotes reduction of alveolar edema
4. Improves the ventilation-perfusion ratio and decreases intrapulmonary shunting
Indications for CPAP include (14):
• Babies weighing less than 1000 grams with respiratory distress and a good respiratory drive.
• Clinically increasing respiratory distress in any gestation (check to rule out pneumothorax)
• Post-extubation in VLBW babies.
Use CPAP with caution in:
• Meconium aspiration syndrome, for the risk of pneumothorax in a vigorous baby
• Gastrointestinal malformations for e.g. Tracheo-oesophageal fistula; for the risk of abdominal distension causing splinting of the chest leading to a further compromise of ventilation. In this situation insert an NG tube and aspirate the stomach periodically.
Practical considerations:
• The most appropriate size of hat and nasal prongs / mask should be selected.
• The fit of these should be “snug” but never tight. The fixing ties should never be over tightened in order to maintain a seal as this may cause damage to the face.
• Humidity must be used when delivering CPAP; humidified oxygen
must be delivered at a temperature of 37 C at the baby’s nose.
• Babies with respiratory distress and who weigh less than 1000grams, requiring non-invasive respiratory support should be nursed on nC- PAP.
• Normal CPAP pressures are 5 to 6 cm of water. The use of higher levels of CPAP for individual babies must be agreed by the multi -disciplinary team (MDT) and this decision documented in the notes. As the condition of the baby improves the pressures can be carefully weaned to 4cm water.
• Some babies become agitated on CPAP. Appropriate “nesting” and removal of noxious stimuli such as light and noise can alleviate this. Occasionally sedation such as Chloral Hydrate may need to be considered if these strategies are not working.
For babies extubated onto CPAP not being able to maintain an adequate respiratory effort, reintubation will be required. Signs that aid in the assessment for the need to be reintubated are:
• Significantly increased frequency and severity of apnoeas and brady-cardias
• Increasing oxygen requirements over 60% in term babies and over 40% in preterm babies
• Increased work of breathing
• Poor gases
Complications of CPAP (15):
• Gaseous distension of the stomach +/- feeding difficulties
• Nasal trauma from the pressure of the prongs / mask
• Pneumothorax
Weaning from CPAP:
• Once respiratory distress is settling, weaning from CPAP may be commenced.
• Gradually try to wean the oxygen to air and the PEEP to 5 cm water.
• When the PEEP is 5 cm water and the oxygen requirement is ≤30% consider switching over to High flow nasal cannula Oxygen (HFNC) and monitor work of breathing. See HFNC guideline.
• Babies weighing less than 1000 grams, who are being nursed on nC- PAP, should not be weaned from CPAP until the MDT decide that the baby has a consistently strong respiratory drive.
• If the baby has to work excessively to maintain respiratory status then CPAP should be reinstated. Signs of increase in work of breathing include:
Tachypnoea consistently >60 /min
Tachycardia - >160beats / min
Increasing sub and intercostal recessions
Increase in oxygen by more than 10-20%
Increase in the number of desaturations/bradycardias
Removal from CPAP without Weaning:
Term/Near term babies may require CPAP for only a short time and may not need to wean incrementally from CPAP but may cope well in ambient oxygen or air.
Use of Blood Gases in babies on long term CPAP
Any baby who is placed on CPAP for worsening respiratory distress should have gases taken as frequently as clinical condition dictates. As a guide –
1. For Term / near term babies
• Take gases 4 hrs after CPAP discontinued if clinical condition remains stable in between. Earlier gases are recommended if clinical condition seems unstable to assess need for escalating support.
• If subsequent saturations are > 98% in air, gases do not need to be taken again.
• If in oxygen, take at least one gas daily
2. Preterm/LBW Babies 1 to 14 day old
• Gases should be taken at least daily for babies who are on CPAP in oxygen or on HFNC in oxygen
• Gases should be taken at least 2 times a week for babies on CPAP in air.
• Preterm/LBW Babies 14 days to 28 days
• Gases should be taken at least 2 times a week for babies who are stable on CPAP in oxygen.
• Gases should be taken once a day for babies who are on HFNC in oxygen and on alternate days in those who are on HFNC in air.

Non-invasive Positive pressure Ventilation
Non-invasive intermittent positive pressure ventilation has emerged as an alternative strategy to n-CPAP. It delivers time-cycled positive pressure ven- tilation above a PEEP level in the absence of ET tube [16].
NIPPV can be delivered as:
1. CMV NIPPV
2. BiPAP (Bilevel - NIPPV)
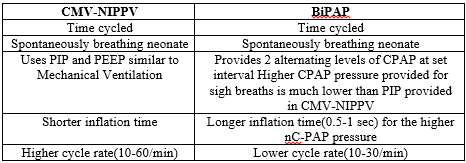
CMV-NIPPV: CMV-NIPPV uses a ventilator to provide intermittent breaths at PIP and rates similar to those used for Mechanical Ventilation.
Physiological Principle:
1. Stablises the alveoli by providing positive airway pressure(PEEP)
2. Promotes better ventilation by delivering positive pressure breaths to the lower airway
3. Triggers an augmented inspiratory reflex (head’s paradoxical reflex) in preterm infants.
4. Less inflammation than Invasive Mechanical Ventilation BiPAP:
It is a form of non-invasive ventilation that provides two alternating levels of CPAP at set intervals using nasal prongs or face mask while the baby is breathing spontaneously. Difference between high and low nCPAP pres- sure is < 4cm>
1. Delta P produced by the ventilator creates a switch from FRC level to another one
2. Derived changes in FRC improves alveolar ventilation
3. Vt depends on both Delta P and lung compliance.
CMV-NIPPV and BiPAP are respiratory support modality with different mechanism to support breathing and their use should be assessed on mer- its and clinical judgement in the same way as for other modalities of ventila- tion.
CMV-NIPPV and BiPAP can be delivered either synchronised or non-syn- chronised. There are various ways of synchronising breaths while the new- born is on CMV-NIPPV/BiPAP however, it is difficult to obtain synchronisa- tion due to open ventilation and very low pressure in preterm infants. NAVA presently offers better possibility of synchronisation. Oesophageal feeding tube is used for NAVA. It signals the onset of diaphragmatic contractions. However, in preterm the combination of diaphragmatic contractions/glottis opening is out of phase in 60‰ cases because glottis opening doesnot fol- low immediately diaphragm contraction. Therefore, ventilation flow could find the glottis closed although diaphragm starts to move downward.There- fore, synchronisation of breaths is difficult with CMV-NIPPV or BiPAP and hence both are generally used in a non-synchronised mode.
When compared with nCPAP; CNV-NIPPV/BiPAP improves thoraco-abdom- inal synchrony, increases tidal volume and minute ventilation and thus de- creases work of breathing and improves CO2 clearance. These effects are better pronounced with synchronised than non-synchronised ventilation.
Indications for NIPPV [17]:
1. Post-extubation failure: In comparison with n-CPAP, NIPPV decreases the frequency of post extubation failure; based on clinical judgement can be considered in neonates with CPAP failure.
2. Apnea of prematurity: In preterm with recurrent apneas while on CPAP, NIPPV has shown to reduce frequency of apnea or need for intubation.
There are 3 kind of interfaces applicable for NIPPV between device and newborn.
1. Short binasal prongs
2. Hypopharangeal tube
3. Nasal mask
Short binasal prongs represent the better interface for both the comfort of the neonate (they adapt correctly and with minimal injury) and the success of the technique (lower flow resistance).

1. Abdominal distension: Less likely to be clinically significant if regular OG tube aspiration is done.
2. Nasal septum erosion/nasal trauma similar to that observed with nCPAP
3. Air leak Syndrome
NIPPV Failure
Consider invasive ventilation in neonates on NIPPV with:
1. Worsening respiratory acidosis
2. Cardiorespiratory compromise
3. FiO2 requirement > 60%.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
