
Case Report | DOI: https://doi.org/10.31579/2641-0419/349
1 Intensive Care Unit, Geneva University Hospitals, Geneva, Switzerland.
2 Faculty of Medicine, University of Geneva, Switzerland.
3 Geneva Hemodynamic Research Group.
4 Department of Cardiovascular Surgery, Geneva University Hospitals, Geneva, Switzerland.
5 Division of Anesthesiology, Geneva University Hospitals, Geneva, Switzerland.
*Corresponding Author: Raphaël Giraud, MD, PhD, Intensive Care Unit Geneva University Hospitals Rue Gabrielle Perret-Gentil 4 CH-1211 Geneva, Switzerland.
Citation: Benjamin Assouline, Damiano Mugnai, Andres Hagerman, Lydia Wuarin, Léonore Schopfer, et al, (2024), Switching from VA-ECMO to a Percutaneous right Ventricular assist device as a Bridge to Recovery in a Case of right Ventricular Myocardial Infarction, J. Clinical Cardiology and Cardiovascular Interventions, 7(2); DOI:10.31579/2641-0419/349
Copyright: © 2024, Raphaël Giraud. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 February 2024 | Accepted: 13 February 2024 | Published: 13 March 2024
Keywords: va-ecmo; short-term mechanical assist device; right ventricular assist device; protekduo; cardiogenic shock; right ventricular myocardial infarction
Acute right heart failure (RHF) is associated with high morbidity and mortality. Temporary mechanical circulatory support (MCS) is now part of the advanced management strategy for refractory cardiogenic shock (CS). Among such support systems, veno-arterial Extracorporeal Membrane Oxygenation (VA-ECMO) remains the fastest MCS system to set up. The ProtekDuo cannula can be used as a temporary and percutaneous right ventricular assist device (RVAD) in relay with VA-ECMO in the context of prolonged weaning.
This case report describes the clinical course of a 69-year-old patient who underwent elective aortic valve replacement surgery complicated by acute RHF due to iatrogenic ligation of the right coronary artery. VA-ECMO was initiated in the context of refractory cardiogenic shock. Faced with prolonged MCS weaning, due to lack of recovery of the right ventricle associated with the absence of any other therapeutic option, a percutaneous RVAD via a ProtekDuo cannula was implanted as a bridge to recovery. The ProtekDuo was gradually weaned while the patient began rehabilitation. The patient was transferred to the medical ward after 5 weeks in the ICU, stayed 5 months in an acute medical setting, went to a rehabilitation center afterward and returned home 6 months after the initial surgery without any neurological sequalae or organ failures. In total, she remained on MCS for 39 days (21 on VA-ECMO and 18 on ProtekDuo).
In cases of refractory RHF, after stabilization and organ perfusion restoration under VA-ECMO, it is feasible to switch to a percutaneous RVAD, allowing early mobilization of patients during prolonged MCS weaning until the right ventricle adapts to new loading conditions.
Acute myocardial infarction (MI) involving only the right ventricle (RV) is a rare event, with an estimated incidence of less than 3% and is frequently associated with a iatrogenic cause (cardiac surgery and interventional cardiology) [1-3]. More commonly, right ventricular myocardial infarction (RVMI) is associated with inferior acute myocardial infarction (AMI), occurring in 30 to 50% of the cases [4]. However, compared to patients without RV infarction, hemodynamically significant right ventricular AMI have a worse prognosis in the acute phase and are more prone to develop refractory cardiogenic shock [5].
Temporary mechanical circulatory support (MCS) is now part of the advanced management strategy for refractory cardiogenic shock (CS) [6]. Herein, we describe the clinical course of a 69-year-old patient who underwent elective aortic valve replacement surgery complicated by acute right ventricular failure (RVF) due to iatrogenic ligation of the right coronary artery with refractory cardiogenic shock (CS), requiring the initiation of veno-arterial Extracorporeal Membrane Oxygenation (VA-ECMO). Faced with prolonged weaning due to lack of recovery of the right ventricle, a percutaneous right ventricular assist device (RVAD) via a ProtekDuo cannula was implanted as a bridge to recovery. The aim of this article is to review and discuss the place of temporary MCS in the management of refractory isolated right ventricular failure in the context of AMI.
A 69-year-old patient without any relevant past medical history underwent aortic valve replacement in the context of a bicuspid valve and severe aortic stenosis. The surgery was uneventful, and the patient was weaned from cardiopulmonary bypass successfully with a minimal amount of vasopressor support and under transesophageal echocardiography (TOE) guidance. However, while surgical hemostasis was performed, the patient became progressively unstable and required increased doses of vasopressors and inotropes (norepinephrine up to 1 µg/kg/min and dobutamine up to 10 µg/kg/min). After sternal closure, another TOE examination was urgently performed and showed severe dilation and global akinesia of the right ventricle. The surgical and anesthesiology team decided to proceed to a percutaneous coronary intervention (PCI). Angiography showed complete occlusion of the right coronary artery (Figure 1); however, the artery was not technically amenable to percutaneous treatment. The patient was transferred to our tertiary ECMO center in critical condition. Indeed, on arrival, the patient presented with profound CS refractory to optimal medical management (SCAI E). VA-ECMO was immediately initiated, complicated by a brief cardiac arrest during cannulation (bilateral femoral cannulation: arterial cannula was inserted on the left and venous cannula on the right side). Due to an ischemic time of more than 8 hours, the small caliber of the right coronary artery and left coronary dominance (Figure 1), it was decided by a multidisciplinary team (cardiac critical care, cardiology and cardiac surgery consultants) to not proceed with emergent coronary artery bypass graft surgery in a patient presenting with multiple organ failure (MOF). Anticoagulation was withheld during the initial 48-hour period. This decision was made because the patient presented rapidly after admission a tamponade along with a hemorrhagic shock resulting from bleeding at the aortotomy site. Subsequently, a conventional anticoagulation regimen with unfractionated heparin was initiated and gradually increased towards therapeutic anticoagulation levels (Anti-Xa 0.3-0.5 IU/ml). The patient's anticoagulation status was closely monitored through Anti-Xa assay measurement.
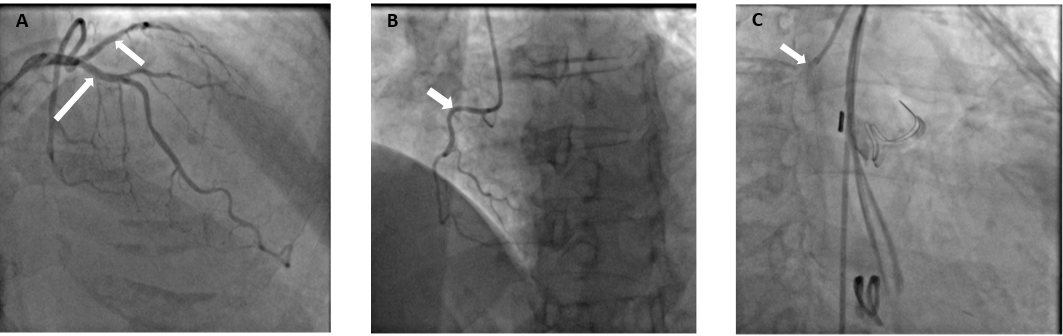
LCA: Left coronary artery, RCA: right coronary artery
Figure 1: Preoperative coronary angiography reported a Left dominance Panel A, white arrows & B, white arrow). Postoperative coronary angiography confirmed an ostial right coronary artery occlusion (Panel C, white arrow).
When the patient stabilized and organ function was restored, sedation was stopped, allowing neurological evaluation. Awakening occurred on postoperative Day 4, without any neurological sequelae, and the patient was extubated. Levosimendan was initiated on Day 10, and fluid depletion was achieved through diuretic administration. Nonetheless, the patient could not be weaned off VA-ECMO due to an akinetic and nonrecruitable right ventricle, despite inotropic support. It was decided to wait further on MCS. The patient was conscious, calm, and cooperative but remained bedridden because of the femoro-femoral VA-ECMO. After two weeks, the patient still could not be weaned off from VA-ECMO. Indeed, below two liters per minute of blood flow, the patient showed both macrocirculatory and microcirculatory signs of RVF. The mean arterial pressure dropped, the central venous pressure (CVP) increased up to 25 mmHg, the central venous
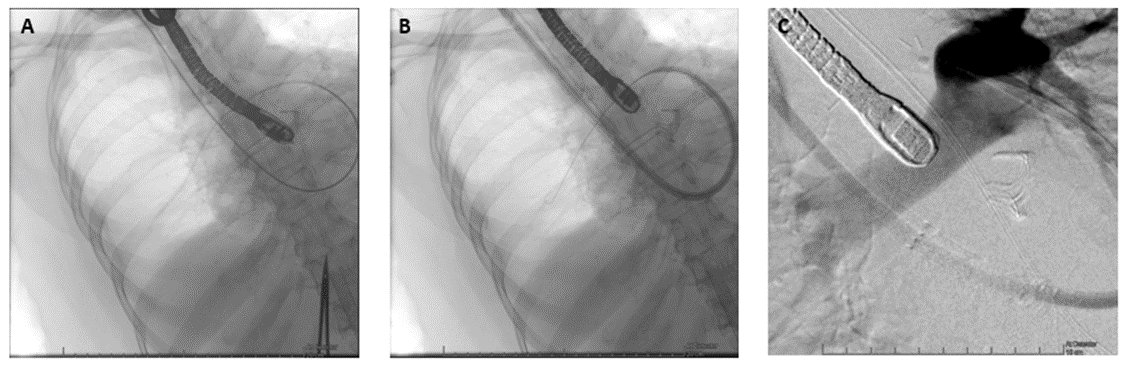
oxygen saturation (SvO2) dropped from 60 to 30%, the lactate level increased up to 4 mmol/l, and the patient became oliguric. The TOE exam showed a severely dilated and akinetic right ventricle (Tricuspid Annular Plane Systolic Excursion (TAPSE) 4mm, lateral tricuspid annulus peak systolic velocity (S’) 2.3 cm/s, RV Fractional area change (FAC) 10%), a small left ventricular (LV) size with a preserved function and a left ventricular outflow tract velocity time integral (LVOT VTI) 10 cm/s. Due to her age and an INTERMACS 1 profile, the patient was not eligible, in our country, for a heart transplant or a definitive RVAD implantation (Heartmate III, modified insertion for the right ventricle). Faced with the prospect of prolonged weaning and no other therapeutic alternatives, VA-ECMO was switched to a temporary percutaneous RVAD by implanting a ProtekDuo cannula through the right internal jugular route (Figure 2).
TOE: Transesophageal echocardiography.
Figure 2: Insertion of the ProtekDuo cannula under fluoroscopy and TOE. A: Pulmonary artery catheter already positioned in the right pulmonary artery. B: Insertion of the ProtekDuo cannula on the guidewire. C: Confirmation of positioning by injection of contrast via the distal port of the ProtekDuo cannula with its tip located in the main trunk of the pulmonary artery.
A centrifugal pump without an oxygenator was connected to the cannula with an initial flow rate of 4 liters per minute. After a few minutes, the VA-ECMO components could be removed without any vasopressor support. After the
initiation of the RVAD, intraoperative TOE showed a reconfiguration of the ventricles. The right ventricle was suitable unloaded by the RVAD, while the left ventricle resumed a circular shape with complete regression of the D-shaped sign (Figure 3).
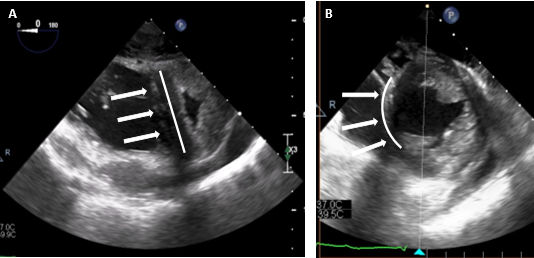
Figure 3: Intraoperative TOE images before VA-ECMO decannulation (Panel A) showing D‐shaped left ventricle (white line and arrows) and under Protek Duo support only (Panel B) showing thatthe right ventricle was suitable unloaded by the RVAD, while the left ventricle resumed a circular shape with complete regression of the D-shaped sign (white line and arrows).
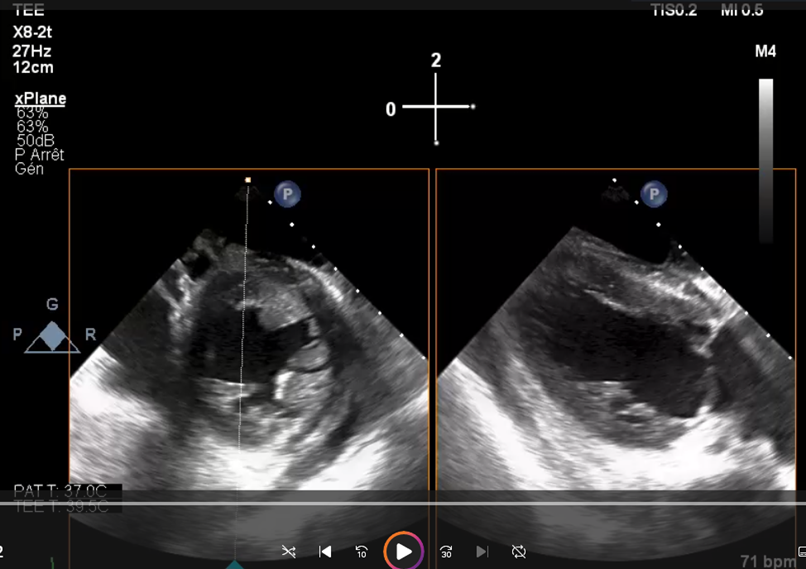
Video 1: Transesophageal echocardiography on VA-ECMO showing a severe dilation of the RV compressing the left ventricle (D-shape).

Video 2: Transesophageal echocardiography on ProtekDuo/RVAD after VA-ECMO decannulation showing a complete regression of the D-shape.
The hemodynamic tolerance of the RVAD was very good (lactate levels < 2> 60%, normal renal and hepatic function). The day after the implantation, the patient was out of bed, placed in a chair, and began rehabilitation. Slow and gradual weaning was instituted. In fact, during the following three weeks, a gradual reduction in the flow rate of the RVAD was carried out at a rate of approximately one liter per week. Interestingly, the serial transthoracic echocardiogram (TTE) exam did not show a significant improvement in RV contractile function, but as the pulmonary pressure, pulmonary resistance and LV-end-diastolic pressure (LVEDP) remained low, the patient’s hemodynamics adapted and showed physiological similarities with a Fontan circulation. During gradual weaning, the renal and hepatic function was monitored daily (creatinine, blood urea nitrogen, aspartate aminotransférase, alanine aminotransférase, bilirubin and factor V levels) and we did not observe any biological signs of congestion or organ dysfunction. Finally, the patient could undergo explantation after 3 weeks of RVAD support. Closed monitoring for 5 additional days was carried out in the ICU. Right ventricular systolic function remained poor (three-dimensional RV ejection fraction (RVEF) = 26%, RV FAC = 21%, severely reduced longitudinal function with global akinesia except for the apical segments of the anterior and lateral wall) but was well tolerated. CVP remained below 15 mmHg, SvO2 was above 60% with normal lactate levels, and renal and hepatic functions remained stable. Anticoagulation therapy was empirically initiated to prevent thromboembolic events, as the patient would likely not survive any abrupt increase in RV afterload. Diuretics and antihypertensive treatments were continued to maintain a low LVEDP. To be noted, during mechanical circulatory support, the patient did develop only minor ECMO-related complications. Minor bleeding at the canula site were noted after canulation and stopped rapidly after optimization of the coagulation profile. Femoral venous thrombosis (at the site of the cannula) was diagnosed after explantation and treated accordingly. We did not observe any Protekduo-related complications.
The patient was transferred to the medical ward after 5 weeks in the ICU, stayed 5 months in an acute medical setting, went to a rehabilitation center afterward and returned home 6 months after the initial surgery. In total, she remained on MCS for 39 days (21 on VA-ECMO and 18 on ProtekDuo).
The present case report highlights that during an isolated RV infarction leading to refractory CS, switching from VA-ECMO to an isolated RVAD via a Protek Duo cannula is a feasible strategy in the context of prolonged weaning from MCS. This approach allowed awakening, extubation and mobilization of the patient while enabling the right ventricle to progressively adapt to new loading conditions.
RVF due to acute myocardial infarction (MI) is rare but is associated with high morbidity and mortality [6]. This condition can occur in a perioperative context of cardiac surgery [7]. In post-MI RVF, RV contractile function becomes severely impaired, resulting in a decrease in RV systolic pressure, an increase in end-diastolic volume, and an increase in end-diastolic pressure. Due to the pericardial constraint, the pressure and volume overload lead to a shift of the interventricular septum to the left, decreasing the LV compliance and LV filling and therefore leading to a low end-diastolic volume. With the reduction in diastolic function and dilation, the volume overload of the right ventricle causes an increase in right atrial pressure and a decrease in venous return and systemic venous congestion, which can lead to acute kidney injury (AKI), ischemic hepatitis, or mesenteric ischemia [2,4,6,8]. Altogether, these combined effects can lead to decreased left heart
filling, reduced systemic cardiac output and ultimately to CS with multiple organ failure [6].
Management strategies for CS in post-MI RVF include early hemodynamic and ultrasound recognition, recommendation for PCI within 90 minutes (class 1), careful fluid management, administration of vasoactive/inotropic drugs to maintain end-organ perfusion and optimization of RV afterload 9. In this patient, PCI was not technically feasible, and surgical revascularization was not performed because of the long ischemic time, the presence of a dominant left coronary network and a right coronary artery too small to be bypassed, all in the context of a patient with multiorgan failure.
In cases of CS refractory to optimal medical management, early initiation of short-term MCS should be considered [9]. Current options for percutaneous MCS for isolated RVF include the Impella RP, TandemHeart RV assist device, ProtekDuo dual lumen cannula, and VA-ECMO [10].
VA-ECMO involves a rapidly implantable percutaneous device that not only unloads the right ventricle and reduces venous congestion but also supports end-organ perfusion. This is the most widely used and easily accessible short-term MCS in refractory CS [11]. Nonetheless, when organ functions are restored and only RVF persists, VA-ECMO can be considered a limitation, particularly regarding mobilization and rehabilitation.
A more RV-specific MCS system exists and could therefore be considered. The Impella RP (right peripheral; Abiomed Inc., Danvers, MA) is a percutaneously implantable microaxial 22 French pump. Blood is aspirated from the right atrium and ejects into the pulmonary artery (PA), bypassing the right ventricle [12]. A reduced RA pressure, increased PA pressure, and increased LV preload characterize the hemodynamic effects of the Impella RP [13]. The main disadvantage of this device, at least in Europe at present, is that it can only be placed through femoral access, which limits patient mobility and therefore rehabilitation. Compared to other MCS systems, it does not provide any respiratory support due to the absence of an oxygenator [14]. In addition, rotating at 33,000 RPM for a maximum flow of 4 L/min, the pump could generate clinically significant hemolysis and therefore increase morbidity [15]. In a recent study reporting the outcomes of patients with acute RVF and cardiogenic shock treated with Impella RP, Botti et al. mentioned that the morbidity burden with Impella RP remains high with significant rates of hemolysis and severe bleeding [12]. In two observational studies [16,17], which used different types of Impella, and in a systematic review about temporary RVAD [14], Impella RP exhibited a higher rate of hemolysis compared to Impella CP/5.0/5.5 or other RVAD. Successful use of the Impella RP has been reported in post-MI RVF, in massive pulmonary embolism [18], in postcardiotomy syndrome [13], after LVAD implantation [19], and in primary graft dysfunction after orthotopic heart transplantation [20]. However, even if these studies have shown encouraging results, they only included small and heterogeneous patient cohorts, with a small proportion presenting post-MI RVF. Furthermore, some results have been the subject of postapproval study assessment by the US Food and Drug Administration (FDA) [21]. Therefore, the Impella RP may be used in RVF refractory to medical therapy as a bridge to recovery but requires further analysis regarding long-term benefits.
The TandemHeart RVAD is a dual-access extracorporeal centrifugal pump that can deliver blood flow at a rate of up to 4 L/min. Classically, it uses two 21 F cannulas implanted via the femoral veins: one is placed in the right atrium (inflow), and the other is placed in the PA (outflow) [22]. The TandemHeart RVAD can be used with a circuit-coupled oxygenator and can be used to manage concomitant hypoxic respiratory failure [23]. The hemodynamic profile of the TandemHeart RVAD is similar to that of the Impella RP, with a reduced RA pressure, increased PA pressure and increased LV preload [13]. Due to the required femoral access, it shares the same disadvantages as the VA-ECMO and IMPELLA RP devices regarding patient mobilization and rehabilitation.
The ProtekDuo cannula is a 29 Fr or 31 Fr double-lumen cannula that is inserted percutaneously via the right internal jugular vein [24]. The inflow is positioned in the right atrium and the outflow in the PA. These two ports are connected to a centrifugal pump, with or without an oxygenator, which can generate, depending on the size of the cannula, up to 4 to 5 liters of blood flow. The major advantage of the ProtekDuo cannula is the elimination of femoral access, thus allowing patient mobilization [25]. Furthermore, as shown in this case report, temporary RVAD, unlike VA-ECMO, allows the loading and evaluation of the left ventricle, a prerequisite for the implementation of a long-term RVAD. The use of the ProtekDuo® cannula coupled with a centrifugal pump for isolated acute RV failure has been the subject of several case series. In a serie of 13 patients with acute RV failure treated with the ProtekDuo®, including four who had acute RV myocardial infarction, Nicolais et al. reported a median duration of support of 6 days and a survival rate of 54% to device explantation [26]. In another retrospective study of 10 patients with acute myocardial infarction complicated by acute RV failure who underwent ProtekDuo® implantation for RVAD support, Kremer et al. reported a mean duration of RVAD support of 10 ± 7.4 days and a 30-day and 1-year survival rate of 60% [27]. Finally, in a retrospective cohort study of 40 patients with acute RV failure, Badu et al. reported an overall rate of survival to discharge of 68%.
The dual-lumen ProtekDuo cannula as RVAD has limitations. A systematic review including seven studies with 127 patients reported these complications and adverse effects. Device-related complications most often described are cannula migration, thrombosis, moderate to severe tricuspid regurgitation created by the cannula, vascular injury, bleeding from cannula site and superior vena cava syndrome. Non-device related complications described are renal failure requiring hemodialysis, hemorrhagic stroke and sepsis. However, the occurrence of these complications did not seem to be more frequent compared with other currently available temporary RVAD systems [25].
Regarding the present case, three questions may arise. The first question is whether implanting the VA-ECMO before the patient’s transfer to our center would have been preferable to prevent an ECPR situation? Mobilizing a mobile ECMO team is not always feasible in a timely manner and was not possible in this case. Additionally, the referring hospital's critical care team and medical transfer team deemed the patient safe for transport. Transfer to a tertiary center was therefore the only option to provide further care to this patient. Secondly, could the implantation of a temporary RVAD have been carried out from the beginning? The implantation of this type of device, even when done percutaneously, is slower and more complex than a VA-ECMO and requires fluoroscopy and experienced operators. Furthermore, the patient presented with profound cardiogenic shock with multiple organ dysfunction and arrested during canulation. In these circumstances, VA-ECMO is the most suitable short-term MCS to consider. Finally, could the temporary RVAD have been implanted earlier, allowing the patient to be mobilized sooner? Failing RV adapts over time to new loading conditions, especially in the absence of pulmonary arterial hypertension. There is a paucity of data regarding the timing of recovery of the RV after AMI-associated CS. This can vary significantly between patients. We had expected our patient to recover earlier, which might have enabled us to wean VA-ECMO without requiring to a temporary RVAD.
To our knowledge, none of those studies mentioned or proposed strategies to improve rehabilitation, including switching from VA-ECMO to ProtekDuo®/RVAD support. The ProtekDuo® cannula may offer additional benefits, including nonsurgical, single-site access in the upper body, which may allow for earlier extubation and/or mobilization, as in our patient 28. Indeed, once the organ dysfunctions linked to cardiogenic shock are resolved, we suggest switching as soon as possible from VA-ECMO to an alternative RV-MCS approach to avoid VA-ECMO-associated complications that are expected much earlier than in alternate approaches
In cases of cardiogenic shock due to isolated RV failure refractory to optimal medical management, VA-ECMO remains the fastest implantable MCS system, allowing hemodynamic and respiratory stabilization. In the context of prolonged RV support, switching to ProtekDuo®/RVAD support can enable the right ventricle to adapt to its new loading conditions through progressive weaning and permit early mobilization and rehabilitation.
BA, KB and RG wrote the first draft. DM, AH, LW and LS revised it critically for important intellectual content; All authors approved the final version of the manuscript.
Funding:
None
Acknowledgements:
None
Conflict of interest:
The authors have no conflict of interest to declare.
Ethics statement
The patient signed a declaration of consent for the use of health data for research purposes and accepts that her health data and biological samples collected during episodes of care may be used for research purposes.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
