1Department of Plastic and Reconstructive Surgery, MedStar Georgetown University Hospital; Washington, District of Columbia.
2Department of Plastic and Reconstructive Surgery, Georgetown University School of Medicine; Washington, District of Columbia.
3Plastic and Reconstructive Surgery Division, Rutgers Robert Wood Johnson Medical School, New Brunswick, New Jersey.
4Department of Surgery, University of Pittsburgh Medical Center (UPMC) Mercy Hospital, Pittsburgh, Pennsylvania.
5Division of Plastic and Reconstructive Surgery, Department of Surgery, Keck School of Medicine, University of Southern California, Los Angeles, California.
6Department of Plastic and Reconstructive Surgery, MedStar Washington Hospital Center; Washington, District of Columbia.
*Corresponding Author:
Laura K. Tom, MD, Department of Plastic and Reconstructive Surgery MedStar Washington Hospital Center 106 Irving Street NW Washington DC, 20010.
Citation: Daisy L. Spoer, Lauren E. Berger, Parhom N. Towfighi, Karen R. Li, Laura K. Tom, (2024), Surgical Techniques for Lymphovenous Bypass: A Review, International Journal of Clinical Case Reports and Reviews, 17(5); DOI:10.31579/2690-4861/462
Background: Lymphedema is a progressive, debilitating disease that may affect up to 250 million individuals worldwide. Complex decongestive therapy (CDT) remains the first line of treatment for lymphedema, and surgical treatment currently has no formally established role. In recent years, lymphovenous bypass (LVB) has emerged as a potentially efficacious intervention to improve patients' objective and subjective measures of lymphedema. Despite this promise, there are few evidence-based recommendations to inform the adoption of the practice.
Methods: A narrative review of the present literature on LVB was performed through a query of records using various combinations of Medical Subject Heading (MeSH) terms and keywords such as “lymphatic vessels,” “lymphedema,” “breast cancer lymphedema,” “surgical anastomosis,” “lymphovenous bypass,” “lymphovenous anastomosis.” The articles were assessed for 1) bibliometric characteristics, 2) preoperative evaluation, 2) operative techniques, 3) postoperative regimens, and 4) outcome measures.
Results: The sixty-year evolution of LVB has transformed rapidly in response to technological advances in the last two decades. The geographically distributed investigation of these surgical innovations has prompted a fragmentation of LVB practice. As original research outpaces literature review, there needs to be more consistency in terminology, perioperative practices, and evaluation of outcomes of LVB, which challenge systematic analysis. The systematic reviews to date emphasize the ability of LVB to improve objective measures such as limb circumference. Still, the inconsistent use of subjective measures limits our appreciation of the collective improvement in patient-reported outcomes. Moreover, there are a limited number of accepted methods for patient selection, preoperative evaluation, and surgical planning, with many surgical techniques employed.
Conclusion: The unifying principles and scientific evidence must be clarified to guide an overarching consensus before the widespread adoption of LVB. This article aims to synthesize recommendations and current institutional preferences concerning the research and clinical applications of LVB. The collaboration and continued refining of these practices will be necessary to establish the role of LVB in the treatment and prevention of lymphedema.
Introduction
Lymphedema is a progressive, debilitating disease that may affect up to 250 million individuals worldwide [1]. In the industrialized world, secondary lymphedema often develops as a sequela of surgery, radiation, and chemotherapy in cancer treatment [2-6]. Inflammation due to surgery or chemotherapy can induce exudation of lymphatic free fatty acids and promote adipogenesis [4,7-9]. Synergistically, radiotherapy causes direct DNA damage and the release of reactive oxygen species that promote time-dependent degeneration [10-12]. The associated fibrosis and adipogenesis contribute to afterload-mediated lymphatic remodeling and dysfunction like hypertensive cardiomyopathy [4,13-17]. The disease is generally progressive, hastened by obesity, and results in reduced quality of life for up to 10 years [18].
Complex decongestive therapy (CDT) is the standard approach to lymphedema management, but routine manual drainage and compression offer limited efficacy while carrying an immense treatment burden with inconsistent insurance coverage [19-24].
The rising survivorship may predict increases in breast cancer-related lymphedema, and surgical innovations may offer solutions for preventing or mitigating the morbidity of this condition. Lymphovenous bypass is a physiological intervention that ideally prevents lymphedema progression by increasing collateral lymphatic outflow. Today, the advances in imaging and supermicrosurgical LVB confer an average decrease of 4.1 cm in limb volume and improve the quality-of-life measures in 57-100% of patients [25-30].
Despite scientific evidence that LVB can improve subjective and objective outcomes of lymphedema beyond CDT, the marked heterogeneity of practice limits the widespread adoption.6,19,20,27-42 This narrative review aims to provide an overview of current LVB research, perioperative practices, and outcome measures to highlight essential gaps in the distributed investigation of LVB, which warrant further study and consensus.
Methods
Study Design
A literature search through December 2022 was performed across PubMed, the Web of Science, and Grey literature. A list of predetermined Medical Subject Heading (MeSH) search terms and keywords were employed, including but not limited to various combinations of the following: “lymphatic vessels,” “lymphedema,” “breast cancer lymphedema,” “surgical anastomosis,” “lymphovenous bypass,” “lymphovenous anastomosis” and the Boolean operators “AND” and “OR,” disregarding results for non-English language. Following record screening, the remaining studies then underwent full-text review. No restrictions were set on the year of publication, country of origin, or study size. This review's inclusion depended on predefined inclusion and exclusion criteria to select original and review articles on lymphovenous bypass. Studies assessing all physiologic lymphedema surgery were included only if outcomes of interest were stratified by procedure to understand the specific role of LVB better. Articles describing other surgical interventions, such as vascularized lymph node transfer or non-physiologic lymphatic surgery without cases of LVB, were also excluded. Full-text studies were included in this narrative review if they reported on the outcomes of interest. The articles were assessed for 1) bibliometric characteristics, 2) preoperative evaluation, 2) operative techniques, 3) postoperative regimens, and 4) outcome measures. Bibliometric data included information related to the terminology used, research era, and study location. Preoperative evaluation included data related to diagnosis and imaging. Operative techniques included data about instruments, vessel selection, bypass methods, and surgical training. The primary outcomes included clinical and patient-reported outcomes.
Results
LVB Research and Nomenclature
The composite field of lymphedema research expanded within the last two decades (87.7%), of which surgery was the second most researched topic.6 Today, the leaders of lymphedema research span Australia, Belgium, China, Germany, Italy, Japan, the United Kingdom, the United States, and Taiwan.6 A recent bibliometric analysis of lymphedema research between 1900-2023 revealed that Japan had contributed the largest quantity of papers related to “lymphovenous anastomosis” and “microsurgery” (n=73 and 41 publications/year). The second most productive country for “lymphovenous anastomosis” was the United States (n=46 publications/year), which was tied with Italy as the second most productive in “microsurgery” (n=21 publications/year) [6].
A search of terms related to lymphatic surgical “bypass” (n=1093 PubMed results) and “anastomosis” (n=1,614 PubMed results) reveal trending parallel investigations on this surgical concept between 1964 and 2023 (n=2862 total PubMed results). The two fields of work may reflect distinct clusters of surgical study (i.e., microsurgical bypass and supermicrosurgical anastomosis) or inconsistent terminology.25,26,43-46 Coriddi et al. suggest using the term “lymphovenous bypass,” as it more accurately describes the “establishment of a shunt” than does the word “anastomosis,” which refers to a “communication between or coalescence of blood vessels.”47 This paper will discuss LVB as a unified topic.
Microsurgical Era (1960-1996)
The initial experimentation with LVB was facilitated by the advent of microsurgery in the 1960s, which permitted the surgical union of lymphatics to veins greater than 1 mm in diameter.48-52 These early models relied on dilated lymphatics and size-matched cutaneous veins for LVB, often impeded by 21 days postoperatively.50-55 In this era, lymphoscintigraphy was the gold-standard imaging modality for lymphedema, which necessitated ionizing radiation while offering low spatial and temporal resolution.
Supermicrosurgical Era (1997-Current)
In 1997, Koshima et al. demonstrated that surgical union of vessels < 0>1mm).57 These efforts have coincided with reports of improved patency at one week (70%), one month (65%), and one year (56.5%) post-procedure.58-60 The advances in imaging came shortly after that in 2001 with magnetic resonance lymphangiography (MRL) with gadolinium-based contrast, which increased the precision of anatomical staging and treatment planning but was expensive, resource-intensive, and potentially impractical for perioperative use.61 Finally, in 2007, indocyanine green (ICG) lymphography combined with near-infrared imaging (near-infrared fluorescence lymphangiography, [NIRF-L]) surfaced as a practical and more affordable functional imaging modality capable of real-time lymphatic mapping to highlight location, drainage directionality, and collateral circulation.62 The lymphatic uptake of ICG in NIRF-L allowed for visualization that ultimately informed the concept of lymphatic territories (“lymphosomes”) [63 ].
Preoperative Evaluation
Patient Selection
A lymphedema diagnosis can be determined by a change in volume measures, bioimpedance spectroscopy, a physical exam, and clinical history. Still, it may be enhanced by additional measures of lymphoscintigraphy, ultrasound, ICG fluoroscopy, or lymphography and classification systems (e.g., International Society of Lymphology staging criteria (ISL) [20,64-73].
The management of lymphedema differs by lymphedema stage and, in the surgical literature, often follows a stepwise application of CDT, LVB, and vascularized lymph node transfer (VLNT) with and without debulking surgery for less severe, partially obstructed, and severely obstructed lymphatics, respectively.27 There is a rationale to recommend LVB before VLNT as LVB is a less invasive procedure and more effective in early-stage disease [27,36,39,74-76]. A failure of conservative management is not an absolute prerequisite for physiologic surgery, and in patients with breast cancer, those with ≥ 10% volume change should be referred to specialist care [77].
Surgical Planning
Objective parameters of the abnormal lymphatic form (i.e., normal, dilated, or collaterals) or function (i.e., dermal backflow [DBF] or increased lymphatic transit time [TT]) are frequently integrated into the staging of lymphedema and are predictive of LVB outcomes. The current recommendation is to incorporate imaging-based modalities with a clinical assessment to characterize the severity of lymphedema and target surgical intervention more effectively. In cases of a nonfunctioning lymphatic system (NIRF-L +/- MRL) and pitting lymphedema, some recommend 1) intensive rehabilitation therapy followed by 2) reassessing the possibility of a reductive surgical technique [78,79]. A functioning lymphatic system (NIRF-L +/- MRL) with a good axillary status may indicate LVB. In contrast, an axilla with fibrotic tissue or signs of radiodermatitis may indicate VLNT with fibrotic release combined with distal LVB [79]. A VLNT can be combined with free tissue transfer and LVB for individuals pursuing simultaneous breast reconstruction [79,80].
NIRF-L, when combined with staging scales (e.g., the Koshima ICG Classification System, MD Anderson Cancer Center (MDACC) scale, and the Dermal Backflow Scale (DBS)), is considered the “gold standard” imaging modality for the diagnosis, severity staging, and surgical planning of LVB (Figure 2) [31,46,81-86]. The perioperative use of NIRF-L permits precise lymphatic mapping and is more predictive of outcomes than ISL.87,88 Adjunctive ultra-high-frequency ultrasound or “rest/stress intradermal lymphoscintigraphy” may enhance NIRF-L sensitivity [44,89-91].
MRL is more sensitive than NIRF-L and may be suitable for cases warranting a more detailed visualization of the deep lymphatic system (>2 cm deep to the skin surface) and surrounding tissue characteristics.31 The increased sensitivity can paradoxically influence inaccurate surgical planning and is often considered impractical due to the financial costs. New frontiers include high-frequency ultrasound imaging and photoacoustic imaging (PAI), both of which are praised for their sensitivity and, in combination with clinical presentation, have the potential to aid in the expansion of LVB indications [31,92,93].
Figure 1. Overview of lymphatic and venous vasculature frequently used in LVB. The caliber of lymphatics varies in the published literature, although they have been categorized into initial lymphatics (0.01-0.06 mm), pre-collector (0.035–0.150 mm), and collector lymphatics (0.200 mm) [182,183]. Thus, we illustrated a collector lymphatic as the relevant structure for LVB. (A) Collector lymphatics have tight “zipper-like” junctions, specialized muscle cells, and valves that coordinate directional lymph flow via suction-derived diastolic filling [3,15,172]. (B) The cutaneous vessels used in LVB generally include valved subdermal venules (0.3-0.6mm) or large cutaneous veins (>1mm).57 The microcirculatory venules and veins vary according to their ultrastructure and anatomical location, and a venule with sparse smooth muscle cells is illustrated for generalizability [101,184,185].
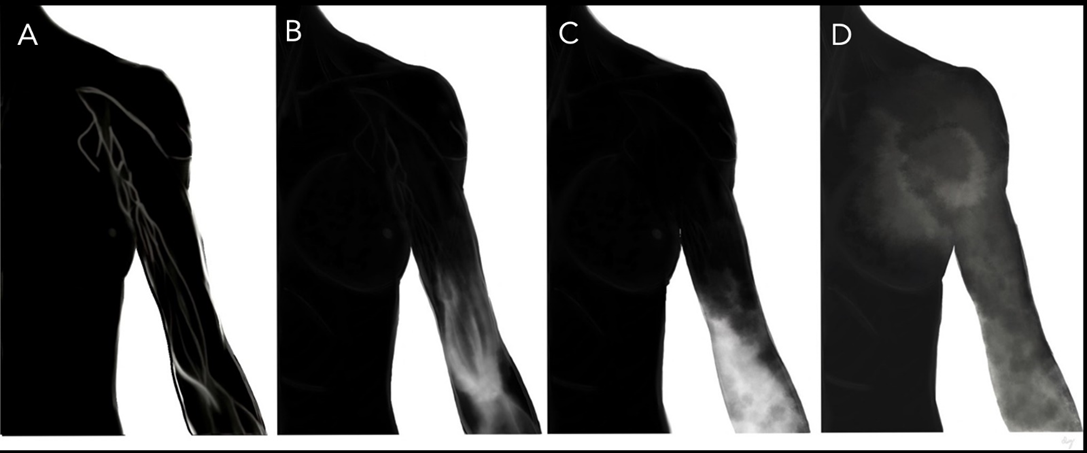
Figure 2. Patient selection and preoperative evaluation. Illustration of Koshima ICG lymphedema classification system [98]. (A) Stage 0: “Normal superficial lymphatic vessels appear as a “linear” pattern with no dermal backflow” (B) Stage 1: “Lymphatic vessels appear dilated and torturous with areas of ICG accumulation as a “splash” pattern” (C) Stage 2: “Contracted lymphatic vessels with loss of intraluminal diameter and thickening of the smooth muscle cell coverage. Lymphatic vessels are disrupted, causing increased areas of ICG accumulation as a “stardust” pattern” (D) Stage 3: “No lymphatic vessels can be seen and there is ICG accumulation as a “diffuse” pattern”[98].
Operative Techniques
Instruments
The preferred instruments for LVB vary and include either supermicrosurgical forceps (0.05 mm tips) or standard microsurgical forceps (0.3 mm). Some consider supermicrosurgical forceps too malleable to avoid damaging the lumen of the lymphatics. Titanium supermicrosurgical instruments and surgical scissors are generally employed.94
Selection of Target Lymphatics
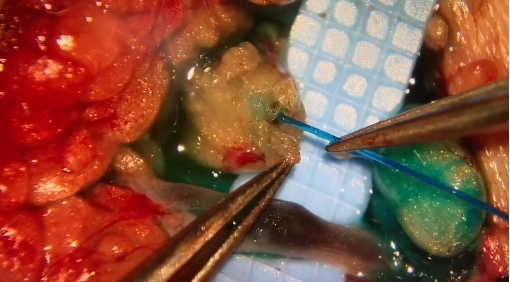
Figure 3 illustrates the step-wise process for selecting target vessels. The lymphatic targets appropriate for bypass must be functional as there is evidence of little to no therapeutic benefit of performing LVB with sclerotic lymphatic vessels. The use of LVB has demonstrated objective and subjective improvement in the lower extremity (objective 46.7-100%, subjective 84-100%) and upper extremity (objective 0-100%, subjective 50-100%) lymphedema.28,29 Functional imaging (i.e., NIRF-L) is recommended for reverse lymphatic mapping. The functional vessels draining the affected distal extremity will appear bright under NIRF-L due to their uptake of ICG (1-2 mg) injected intradermally into the alternating web spaces of the impacted hand or foot.95,96 The fluorescence pattern will demonstrate the disease severity. Incisions are generally guided by dermal backflow (NIRF-L findings) and placed according to the mapped functional lymphatics.36,84,97,98 There is no consensus on the preferred incision length. Still, using the AccuVein system (AccuVein Inc.) in conjunction with NIRF-L, Mihara et al. performed the procedure through a 2-mm incision.45 Isosulfan blue (Lymphazurin; United States Surgical Corp., Norwalk, CT) or methylene blue (American Reagent, Shirley, NY) is helpful intraoperatively, as it allows for gross visualization of lymphatic patency and function (Figure 3). A functional lymphatic is thus frequently defined as both ICG-positive and flow-positive.
Figure A
Figure B
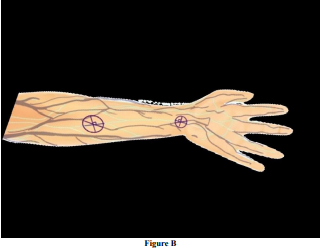
Figure 3: Selection of lymphatic and venous targets. (A) The lymphatic territories (lymphosomes) can be visualized with ICG. Lymphosomes superior to inferior 1) temporal, purple; 2) occipital, blue; 3) mental, tan; 4) supraclavicular, pink; 5) subscapular, not pictured; 6) axillary, dark teal; 7) pectoral, orange; 8) superior inguinal, red; 9) lateral inguinal, salmon; 10) inferior inguinal, magenta; 11) popliteal, not pictured. [illustration of lymphosomes adapted from Suami et al.]186 (B) Pre-incision selection of target vessels will depend on the location of the obstruction and the presence of fluorescent lymphatics and neighboring veins. The incision should be placed over a junction between a lymphatic and vein (X and overlying circle). The incision can be made perpendicular to the lymphatic. Selecting several possible sites for incision is ideal (C) lymphatic and vein in preparation for LVB.
The fibrotic and pressure-overloaded lymphatic in the diseased state will dilate and exhibit ineffective lymphatic pumping.4,7,15 In a recent analysis of 1048 lymphatic vessels, Yang et al. extrapolated that 0.5 mm (lymphatic vessel0.5) represented the threshold for lymphatic function, with calibers ≤ 0.5 mm associated with an adequate function (defined as ICG and flow positive) and postoperative volume reductions [99].
Selection of Recipient Veins/Venules
The pressure gradient, tension, and flow dynamics of the recipient vein (RV) are paramount for a successful bypass.100 An algorithmic approach to venule or venous selection can be based on [1] caliber match, [2] location, and [3] the presence of backflow [100,101]. The original framework considered small RV (≤ 0.4-0.5mm) superior to larger RV in minimizing backflow. This theory potentially contradicts the traditional teaching that, in the supine position, the superior vena cava exhibits the lowest venous pressure as it drains into the right atrium (0-3mmHg) and is precipitously lowered by negative thoracic pressure during inspiration and by gravitational pull when standing [101,102]. Conversely, peripheral venules have higher intraluminal pressures due to an increased net cross-sectional area and relative gravitational influences (hand: +35 mm Hg, foot: +90 mm Hg).103
One study evaluating RV of 1,000 LVBs of similar lymphatic characteristics classified RV according to Visconti flow dynamic classifications, which demonstrated that the smallest RV (≤ 0.4mm) were significantly associated with the least favorable outcomes of backflow and slack compared with medium (0.5-0.9mm) and large (≥ 1mm) RV.100 Matching the caliber of RV and lymphatics while minimizing LVB tension was informative on the final LVB configuration's influence on the outcomes. A physiologic evidence-based algorithm for venous choice is provided in the referenced work [101]
LVB Technique:Configuration
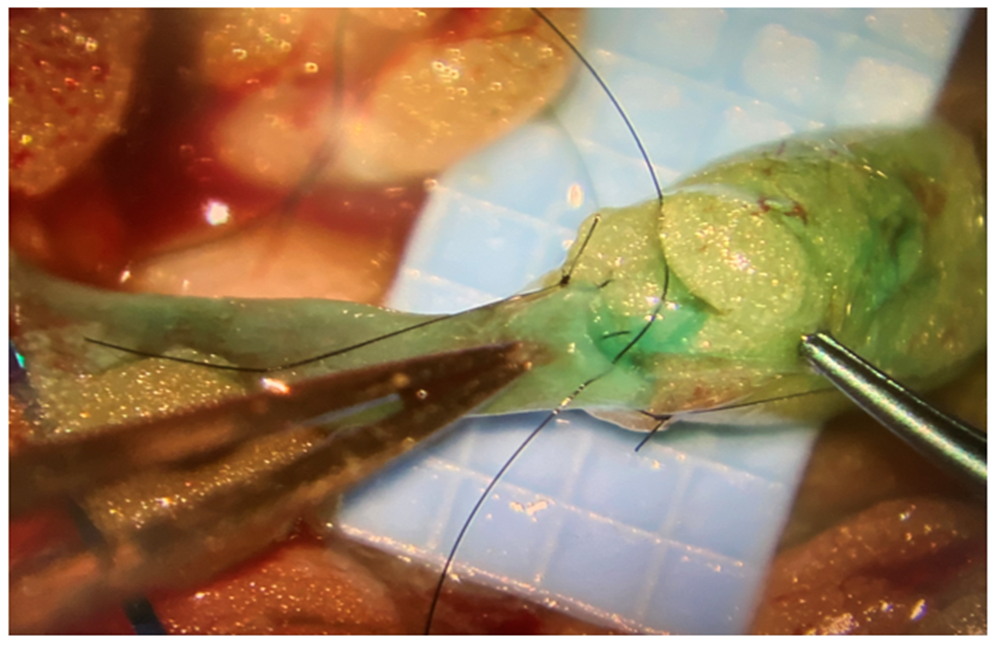
Table 1 depicts the variety of available techniques for LVB from the published literature [43,104-106]. The photographs in Figure 4 demonstrate the practical application of a sequence of methods. The relevance of alternative strategies is primarily addressed in the original papers and institutional care algorithms [94,107-109]. The first described approaches to LVB drew inspiration from microsurgical anastomosis of blood vessels and included end-to-end (E-E) and end-to-side (E-S) configurations [94,110]. However, the postoperative histological evaluation in that era demonstrated that E-E was associated with slight narrowing at the LVB site and that E-S LVB was more often disrupted due to inflammatory changes [51,101]. E-E has remained the most prominent technique across institutions, with authors citing the relative ease of use in caliber matching and improved resistance to venous backflow compared to E-S.
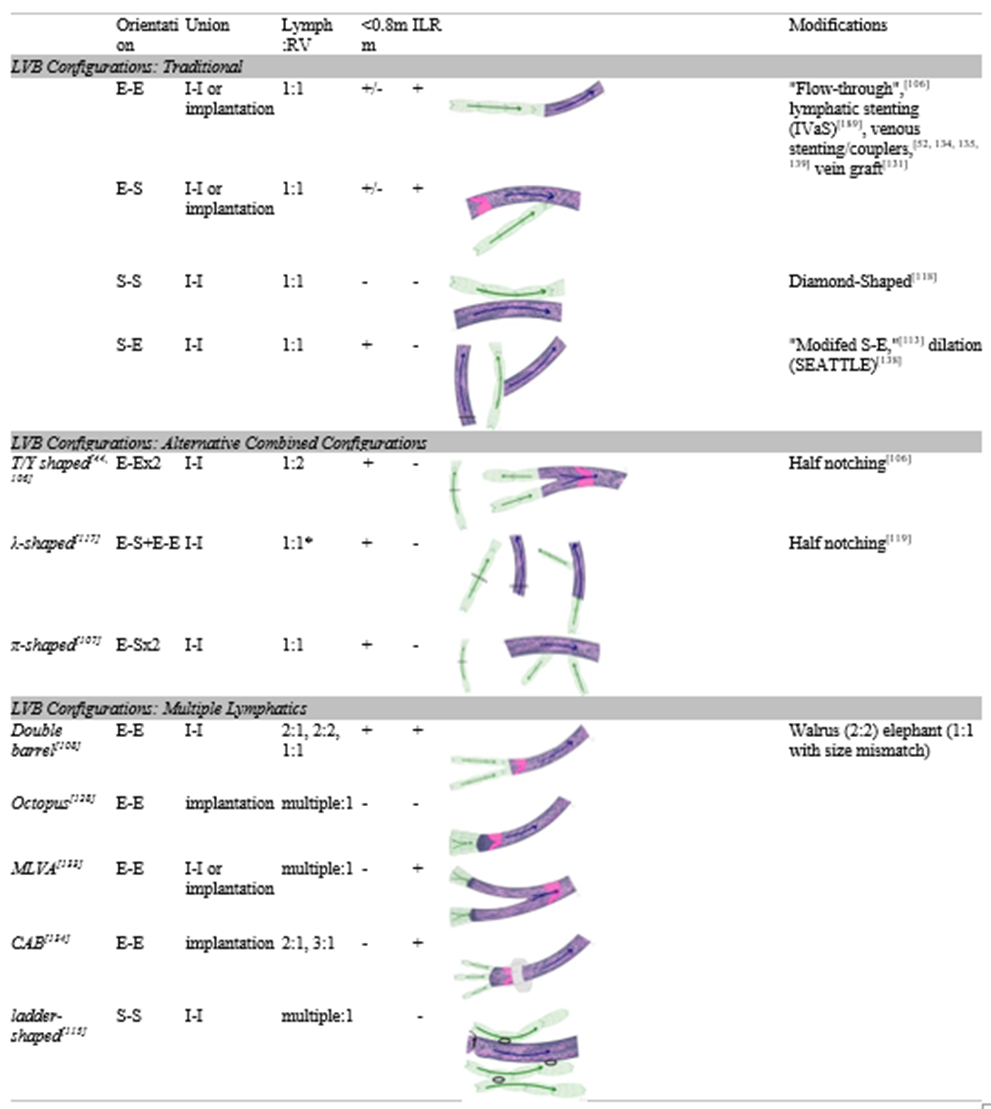
Table 1. Surgical Techniques for Lymphovenous Bypass. Depicts information and illustrations of LVB techniques as described in the published literature. The list is not comprehensive, and more options for LVB exist. Configurations are described by the direction of the union and include end-to-end (E-E), end-to-side (E-S), side-to-end (S-E), and side-to-side (S-S). Ratios of lymphatics: recipient veins (RV) comprise the number of individual, native lymphatics included in the LVB; lymphatics transected and employed using the proximal and distal ends were counted as one lymphatic. Ratios of 2:1 are described as λ-shaped, but the technique is described in the published literature as involving two ends of a transected lymphatic rather than a method of 2:1 LVB. Because procedures involving RV outlets <0>0.8, the procedure was marked with a “+/-.” Procedures that have been applied in the setting of immediate lymphatic reconstruction (ILR) were marked with a “+.” Illustrations are basic representations of the configurations drawn according to the procedural descriptions or images in the referenced articles. Lymphatics, valves, and direction of lymphatic flow (arrows) are depicted in green. RV and direction of flow (arrows) are displayed in dark blue; venous valves are in pink. The directionality of lymphatic flow was based on the orientation described in the technical articles, as lymphatics and RV have directional valves supporting flow in a distal to proximal manner. If the proximal or distal end of the lymphatic or vein was not specified, the directionality was depicted in the anatomical fashion, which would theoretically optimize flow. Modifications to the described approaches are listed with the procedures they are reportedly applied to.
Figure 4A
Figure 4B
Figure 4C
Figure 4D
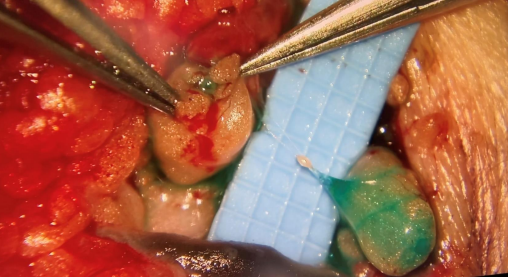
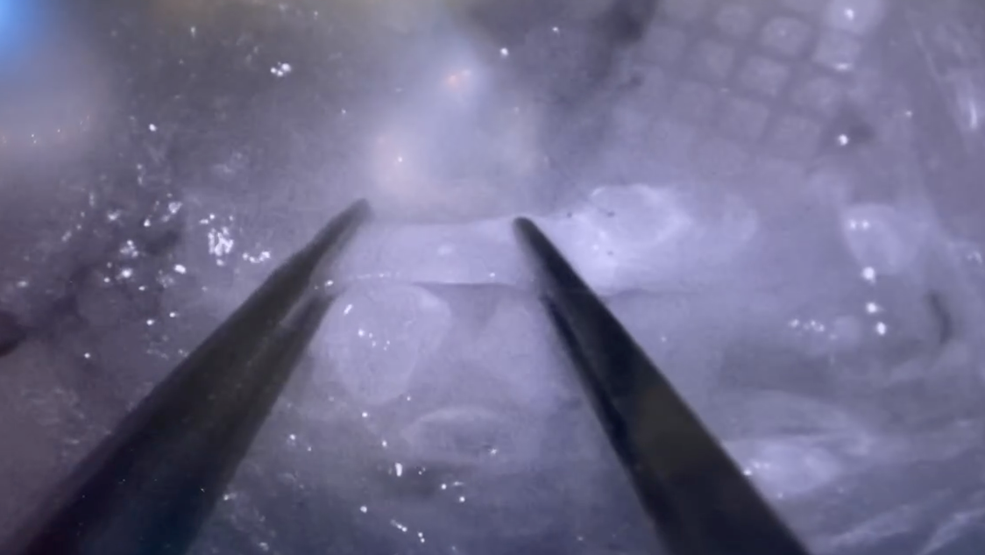
Figure 4. Operative techniques in LVB. (A) Transection of the target lymphatic area should demonstrate lymphatic function. This is facilitated by subcutaneously injecting Isosulfan blue (Lymphazurin; United States Surgical Corp., Norwalk, CT) or methylene blue (American Reagent, Shirley, NY) along the fluorescent lymphatic pathway. (B) Intravascular stenting (IVaS) can be performed with nylon sutures prior to LVB. (D) an implantation technique implants the lymphatic into the venous lumen, using a stitch to connect lymphatic adventitia to venous intima. (E) The success of the bypass can be determined by direct visualization of the unidirectional flow of fluorescence from lymphatic into the recipient vein (distal to proximal) under microscopy.
In 2022, Bianchi et al. further noted that E-E had superior flow characteristics compared to side-to-end (S-E) and side-to-side (S-S). These findings contrast numerous reports corroborating S-E as superior to E-E, particularly in more advanced lymphedema [111,112]. However, Kwon et al.’s results favoring S-E incorporated significantly higher ratios of lymphatics: RV in the S-E group than in the E-E group, possibly confounding their results. Yamamoto et al. reported that S-E and S-S unions outperformed E-S, often resulting in venous-lymphatic reflux and thrombosis [113]. The authors cited that bidirectional drainage is a favorable dynamic, which remains controversial [101,113,114].
A myriad of publications describes combinations and variations of these configurations, including
Postoperative Regimen
The surgical treatment of lymphedema must be combined with lifestyle interventions and postoperative compression. The most common recommendation is to avoid compression in the immediate postoperative period and instead encourage consistently elevating the affected limb though not more than 90 degrees.152,153 The patient can continue compression, lymphatic massage, and lymphedema therapy between 2-4 weeks postoperatively, taking care to avoid massaging incisions, and by one month, they can return to usual activities.152 The outcomes are improved by combining surgery with decongestive therapy, but patients often discontinue CDT postoperatively.154,155 The referrals and planning for post-ILR lymphedema surveillance are usually initiated preoperatively. The regimen after surgery consists of two weeks of decongestive therapy and activity limitations followed by a gradual return to range-of-motion exercises.34,143,146,147 In the first 24 months, patients are screened every three months by specialized physical medicine and rehabilitation physicians for the development of lymphedema via Lymphedema Index (L-Dex; Impedimed, Carlsbad, CA) bioimpedance and arm circumference measurements.156 Beyond two years, patients can be transitioned to bi-annual monitoring. Individuals with abnormal exams should be counseled to wear prescribed compression sleeves (20-30 mm Hg) during daytime hours and be instructed to return after six weeks of wear for retesting.
Outcome Measures
The quality and quantity of lymphedema outcome measures limit the evaluation of LVB efficacy [157]. The objective measures of treatment include limb circumference and volume, which are the most comparable measures of treatment efficacy for lymphedema. Though these metrics are often criticized for being antiquated and unacceptably dynamic, the pooled effects of LVB are considered significantly efficacious in reducing limb circumference or volume [27,158]. Objectively, LVB is associated with a pooled decrease in cutaneous infections.33 Finally, ILR is demonstrated to effectively reduce the risk of lymphedema as measured by a decline in prevalence, incidence, and relative risk [5,32,34,35,38,150,159,160].
The subjective patient-reported outcomes (PROMS) are considered to “improve” after LVB, but metrics are considered too heterogeneous to compare and of universally poor methodological quality [27,30,41]. The Consensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN) analysis suggests that the PROMS with the best methodological quality included the lymphedema life impact scale (LLIS), Lymphoedema Functioning, Disability and Health questionnaire ([Lymph-ICF]; lower-limb specific [Lymph-ICF-LL]), patient benefit index-lymphedema (PBI-L), and upper limb lymphedema 27 (ULL-27) [161-166].
Discussion
Future Directions
Lymphatic Surgical Training
There is yet to be formalized training for supermicrosurgery, which may create additional barriers to entry. To participate in training, expert microsurgeons can engage in a “line production method” for LVB with novice microsurgeons using a microscope and loupes, respectively, as these are demonstrated to increase the quantity and quality of LVB beyond those produced by a traditional single expert, single microscope approach [151]. Papaverine can also prevent lymphatic spasms and reduce lag between novices and experts. Training models are constantly being improved and are demonstrated to support standard microsurgical instruments in anastomosis vessels of up to 0.3mm in an average of approximately 6 minutes [118,167-170].
Physiologic and Biomechanical Research
The lymphatic function and contractile strength may be influenced by manipulation of the luminal size due to fibrosis or surgical technique. Unlike blood vessels, lymphatic vessels propagate fluid synchronously, contracting reminiscent of the cardiac cycle [171]. The current understanding of the lymphatic circulatory system is that it 1) is a low velocity, low-flow system, 2) is composed of individually actively pumping lymphangions bounded by valves, 3) exhibits nonlinear flow or hysteresis, 3) collecting lymphatics exhibit Starling forces with a cyclical contraction (systole), positive transluminal pressure, and ‘suction pressure’ necessary for passive diastolic filling, and 5) is influenced by downstream, upstream, and external pressures [172]. These recently uncovered features indicate the increasing complexity of lymphatics, which may predispose an unpredictable response to surgical interventions. The modern physiologic and biomechanical evaluation of lymphedema surgery in ex-vivo and in-vivo experimentation models lags behind clinical research. Testing these surgical procedures on animal models for lymphedema could enhance the scientific logic behind various practices in LVB [173-180].
Conclusion
The scientific exploration of LVB dates back to the 1960s, during which several imaging methods were developed which permitted further surgical innovation. Over the last twenty years, LVB research has blossomed, driven by novel investigations of surgical techniques.6 The current practices of LVB are evidenced to impact patients’ lives positively, but inconsistent practices challenge the development of evidence-based guidelines and integration in treatment algorithms. Intradisciplinary standardization and high-quality comparative research are needed to inform LVB perioperative decision-making and reach a consensus [30,99,181].
Declarations
Authors’ contributions
Made substantial contributions to the writing of the original draft, review and editing, visualization, and project administration, and gave final approval of the version to be published: Daisy L. Spoer, MS
Made substantial contributions to the writing via review and editing and gave final approval of the version to be published: Lauren E. Berger, BA
Made substantial contributions to the writing via review and editing and gave final approval of the version to be published: Parhom N. Towfighi, MD
Made substantial contributions to the writing via review and editing and gave final approval of the version to be published: Karen R. Li, BS
Made substantial contributions to the conception and design of the study, writing via review and editing, supervision, and gave final approval of the version to be published: Laura K. Tom, MD.
Availability of data and materials
The data supporting this study's findings are available from the corresponding author, [L.K.T.], upon reasonable request.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
This study was performed in line with the principles of the Declaration of Helsinki. This study was conducted with approval granted by the Georgetown-Medstar Institutional Review Board (IRB ID: STUDY00004860, 03/02/2022). All participants provided written informed consent.
Oliver G, Kipnis J, Randolph GJ, Harvey NL. The Lymphatic Vasculature in the 21(st) Century: Novel Functional Roles in Homeostasis and Disease. Cell. Jul 23 2020;182(2):270-296. View
at Publisher |
View
at Google Scholar
Nurlaila I, Roh K, Yeom CH, Kang H, Lee S. Acquired lymphedema: Molecular contributors and future directions for developing intervention strategies. Front Pharmacol. 2022;13:873650. View
at Publisher |
View
at Google Scholar
DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. May 2013;14(6):500-515. View
at Publisher |
View
at Google Scholar
Zhang Y-d, Zhang X, Wang X-y, Han D-m, Du J-s. Visual analysis of global research output of lymphedema based on bibliometrics. Front Oncol. 2022;12:926237. View
at Publisher |
View
at Google Scholar
Ujiie N, Kume T. Mechanical forces in lymphatic vessel development: Focus on transcriptional regulation. Front Physiol. 2022;13:1066460. View
at Publisher |
View
at Google Scholar
Escobedo N, Oliver G. The lymphatic vasculature: its role in adipose metabolism and obesity. Cell metabolism. 2017;26(4):598-609. View
at Publisher |
View
at Google Scholar
Swaroop MN, Ferguson CM, Horick NK, et al. Impact of adjuvant taxane-based chemotherapy on development of breast cancer-related lymphedema: results from a large prospective cohort. Breast Cancer Research and Treatment. 2015;151(2):393-403. View
at Publisher |
View
at Google Scholar
Mortimer PS, Simmonds RH, Rezvani M, Robbins ME, Ryan TJ, Hopewell JW. Time-related changes in lymphatic clearance in pig skin after a single dose of 18 Gy of X rays. Br J Radiol. Dec 1991;64(768):1140-1146. View
at Publisher |
View
at Google Scholar
Boyages J, Vicini FA, Shah C, Koelmeyer LA, Nelms JA, Ridner SH. The risk of subclinical breast cancer-related lymphedema by the extent of axillary surgery and regional node irradiation: a randomized controlled trial. International Journal of Radiation Oncology* Biology* Physics. 2021;109(4):987-997. View
at Publisher |
View
at Google Scholar
Naoum GE, Roberts S, Brunelle CL, et al. Quantifying the impact of axillary surgery and nodal irradiation on breast Cancer–Related lymphedema and local tumor control: long-term results from a prospective screening trial. Journal of Clinical Oncology. 2020;38(29):3430. View
at Publisher |
View
at Google Scholar
Brown S, Dayan JH, Kataru RP, Mehrara BJ. The Vicious Circle of Stasis, Inflammation, and Fibrosis in Lymphedema. Plastic and Reconstructive Surgery.10.1097. View
at Publisher |
View
at Google Scholar
Norrmén C, Tammela T, Petrova TV, Alitalo K. Biological basis of therapeutic lymphangiogenesis. Circulation. 2011;123(12):1335-1351. View
at Publisher |
View
at Google Scholar
O'Melia MJ, Lund AW, Thomas SN. The Biophysics of Lymphatic Transport: Engineering Tools and Immunological Consequences. iScience. Dec 20 2019;22:28-43. View
at Publisher |
View
at Google Scholar
Sweet DT, Jiménez JM, Chang J, et al. Lymph flow regulates collecting lymphatic vessel maturation in vivo. The Journal of clinical investigation. 2015;125(8):2995-3007. View
at Publisher |
View
at Google Scholar
Jørgensen MG, Toyserkani NM, Hansen FG, Bygum A, Sørensen JA. The impact of lymphedema on health-related quality of life up to 10 years after breast cancer treatment. NPJ breast cancer. 2021;7(1):1-8. View
at Publisher |
View
at Google Scholar
Torgbenu E, Luckett T, Buhagiar MA, Phillips JL. Guidelines Relevant to Diagnosis, Assessment, and Management of Lymphedema: A Systematic Review. Advances in Wound Care. 2022. View
at Publisher |
View
at Google Scholar
Torgbenu E, Luckett T, Buhagiar MA, Phillips JL. Guidelines Relevant to Diagnosis, Assessment, and Management of Lymphedema: A Systematic Review. Adv Wound Care (New Rochelle). Jan 2023;12(1):15-27. View
at Publisher |
View
at Google Scholar
Johnstone P, Hawkins K, Hood S. Role of patient adherence in maintenance of results after manipulative therapy for lymphedema. Journal of the Society for integrative Oncology. 2006;4(3):125-129. View
at Publisher |
View
at Google Scholar
King M, Deveaux A, White H, Rayson D. Compression garments versus compression bandaging in decongestive lymphatic therapy for breast cancer-related lymphedema: a randomized controlled trial. Support Care Cancer. May 2012;20(5):1031-1036. View
at Publisher |
View
at Google Scholar
Weiss R. Cost of a lymphedema treatment mandate - 16 years of experience in the Commonwealth of Virginia. Health Econ Rev. Jul 23 2022;12(1):40. View
at Publisher |
View
at Google Scholar
Keskin D, Dalyan M, Unsal-Delialioglu S, Duzlu-Ozturk U. The results of the intensive phase of complete decongestive therapy and the determination of predictive factors for response to treatment in patients with breast cancer related-lymphedema. Cancer Rep (Hoboken). Apr 2020;3(2):e1225. View
at Publisher |
View
at Google Scholar
Campisi C, Eretta C, Pertile D, et al. Microsurgery for treatment of peripheral lymphedema: long-term outcome and future perspectives. Microsurgery. 2007;27(4):333-338. View
at Publisher |
View
at Google Scholar
Campisi C, Bellini C, Campisi C, Accogli S, Bonioli E, Boccardo F. Microsurgery for lymphedema: clinical research and long-term results. Microsurgery. May 2010;30(4):256-260. View
at Publisher |
View
at Google Scholar
Chang DW, Dayan J, Greene AK, et al. Surgical Treatment of Lymphedema: A Systematic Review and Meta-Analysis of Controlled Trials. Results of a Consensus Conference. Plast Reconstr Surg. Apr 1 2021;147(4):975-993. View
at Publisher |
View
at Google Scholar
Gupta N, Verhey EM, Torres-Guzman RA, et al. Outcomes of Lymphovenous Anastomosis for Upper Extremity Lymphedema: A Systematic Review. Plast Reconstr Surg Glob Open. Aug 2021;9(8):e3770. View
at Publisher |
View
at Google Scholar
Verhey EM, Kandi LA, Lee YS, et al. Outcomes of Lymphovenous Anastomosis for Lower Extremity Lymphedema: A Systematic Review. Plast Reconstr Surg Glob Open. Oct 2022;10(10):e4529. View
at Publisher |
View
at Google Scholar
Coriddi M, Dayan J, Sobti N, et al. Systematic Review of Patient-Reported Outcomes following Surgical Treatment of Lymphedema. Cancers. 2020-02-29 2020;12(3):565. View
at Publisher |
View
at Google Scholar
Van Heumen S, Riksen JJM, Bramer WM, Van Soest G, Vasilic D. Imaging of the Lymphatic Vessels for Surgical Planning: A Systematic Review. Annals of Surgical Oncology. 2022-09-28 2022. View
at Publisher |
View
at Google Scholar
Schwarz GS, Grobmyer SR, Djohan RS, et al. Axillary reverse mapping and lymphaticovenous bypass: Lymphedema prevention through enhanced lymphatic visualization and restoration of flow. J Surg Oncol. Aug 2019;120(2):160-167. View
at Publisher |
View
at Google Scholar
Meuli JN, Guiotto M, Elmers J, Mazzolai L, di Summa PG. Outcomes after microsurgical treatment of lymphedema: a systematic review and meta-analysis. International Journal of Surgery. 2023;109(5):1360-1372. View
at Publisher |
View
at Google Scholar
Jorgensen MG, Toyserkani NM, Sorensen JA. The effect of prophylactic lymphovenous anastomosis and shunts for preventing cancer-related lymphedema: a systematic review and meta-analysis. Microsurgery. Jul 2018;38(5):576-585. View
at Publisher |
View
at Google Scholar
Hill WKF, Deban M, Platt A, Rojas-Garcia P, Jost E, Temple-Oberle C. Immediate Lymphatic Reconstruction during Axillary Node Dissection for Breast Cancer: A Systematic Review and Meta-analysis. Plast Reconstr Surg Glob Open. May 2022;10(5):e4291. View
at Publisher |
View
at Google Scholar
Gasteratos K, Morsi-Yeroyannis A, Vlachopoulos NC, Spyropoulou G-A, Del Corral G, Chaiyasate K. Microsurgical techniques in the treatment of breast cancer-related lymphedema: a systematic review of efficacy and patient outcomes. Breast Cancer. 2021-09-01 2021;28(5):1002-1015. View
at Publisher |
View
at Google Scholar
Forte AJ, Khan N, Huayllani MT, et al. Lymphaticovenous Anastomosis for Lower Extremity Lymphedema: A Systematic Review. Indian Journal of Plastic Surgery. 2020-03-01 2020;53(01):017-024. View
at Publisher |
View
at Google Scholar
Cook JA, Sinha M, Lester M, Fisher CS, Sen CK, Hassanein AH. Immediate Lymphatic Reconstruction to Prevent Breast Cancer-Related Lymphedema: A Systematic Review. Adv Wound Care (New Rochelle). Jul 2022;11(7):382-391. View
at Publisher |
View
at Google Scholar
Ciudad P, Escandón JM, Manrique OJ, Bustos VP. Lessons Learnt from an 11-year Experience with Lymphatic Surgery and a Systematic Review of Reported Complications: Technical Considerations to Reduce Morbidity. Archives of Plastic Surgery. 2022-03-01 2022;49(02):227-239. View
at Publisher |
View
at Google Scholar
Chocron Y, Azzi AJ, Bouhadana G, Kokosis G, Vorstenbosch J. Axilla versus Wrist as the Recipient Site in Vascularized Lymph Node Transfer for Breast Cancer-Related Lymphedema: A Systematic Review and Meta-Analysis. J Reconstr Microsurg. Sep 2022;38(7):539-548. View
at Publisher |
View
at Google Scholar
Beelen LM, Van Dishoeck A-M, Tsangaris E, et al. Patient-Reported Outcome Measures in Lymphedema: A Systematic Review and COSMIN Analysis. Annals of Surgical Oncology. 2021-03-01 2021;28(3):1656-1668. View
at Publisher |
View
at Google Scholar
Shah C, Whitworth P, Valente S, et al. Bioimpedance spectroscopy for breast cancer-related lymphedema assessment: clinical practice guidelines. Breast Cancer Res Treat. Feb 2023;198(1):1-9. View
at Publisher |
View
at Google Scholar
Visconti G, Hayashi A, Salgarello M, Narushima M, Koshima I, Yamamoto T. Supermicrosurgical T-shaped lymphaticovenular anastomosis for the treatment of peripheral lymphedema: Bypassing lymph fluid maximizing lymphatic collector continuity. Microsurgery. Nov 2016;36(8):714-715. View
at Publisher |
View
at Google Scholar
Hayashi A, Yamamoto T, Yoshimatsu H, et al. Ultrasound visualization of the lymphatic vessels in the lower leg. Microsurgery. Jul 2016;36(5):397-401. View
at Publisher |
View
at Google Scholar
Mihara M, Hara H, Kikuchi K, et al. Scarless lymphatic venous anastomosis for latent and early-stage lymphoedema using indocyanine green lymphography and non-invasive instruments for visualising subcutaneous vein. J Plast Reconstr Aesthet Surg. Nov 2012;65(11):1551-1558. View
at Publisher |
View
at Google Scholar
Akita S, Unno N, Maegawa J, et al. A phase III, multicenter, single-arm study to assess the utility of indocyanine green fluorescent lymphography in the treatment of secondary lymphedema. Journal of Vascular Surgery: Venous and Lymphatic Disorders. 2022;10(3):728-737. e723. View
at Publisher |
View
at Google Scholar
Coriddi M, Dayan J, Mehrara B. Nomenclature in lymphedema surgery. Plastic and Reconstructive Surgery. 2020;146(3):385e-386e. View
at Publisher |
View
at Google Scholar
Badash I, Gould DJ, Patel KM. Supermicrosurgery: History, Applications, Training and the Future. Front Surg. 2018;5:23. View
at Publisher |
View
at Google Scholar
Danese CA, Papaioannou AN, Morales LE, Mitsuda S. Surgical approaches to lymphatic blocks. Surgery. 1968;64(4):821-826. View
at Publisher |
View
at Google Scholar
O'BRIEN BM, SYKES PJ, THRELFALL GN, BROWNING FS. Microlymphaticovenous anastomoses for obstructive lymphedema: Churchill Livingstone; 1977. View
at Publisher |
View
at Google Scholar
Clodius L, Piller NB, Casley-Smith JR. The problems of lymphatic microsurgery for lymphedema. Lymphology. Jun 1981;14(2):69-76. View
at Publisher |
View
at Google Scholar
Puckett CL, Jacobs GR, Hurvitz JS, Silver D. Evaluation of lymphovenous anastomoses in obstructive lymphedema. Plast Reconstr Surg. Jul 1980;66(1):116-120. View
at Publisher |
View
at Google Scholar
Koshima I, Inagawa K, Urushibara K, Moriguchi T. Paraumbilical perforator flap without deep inferior epigastric vessels. Plast Reconstr Surg. Sep 1998;102(4):1052-1057. View
at Publisher |
View
at Google Scholar
Koshima I, Inagawa K, Urushibara K, Moriguchi T. Supermicrosurgical lymphaticovenular anastomosis for the treatment of lymphedema in the upper extremities. Journal of reconstructive microsurgery. 2000;16(06):437-442. View
at Publisher |
View
at Google Scholar
Winters H, Tielemans HJP, Verhulst AC, Paulus VAA, Slater NJ, Ulrich DJO. The Long-term Patency of Lymphaticovenular Anastomosis in Breast Cancer-Related Lymphedema. Ann Plast Surg. Feb 2019;82(2):196-200. View
at Publisher |
View
at Google Scholar
Onoda S, Kimata Y, Matsumoto K, Yamada K, Tokuyama E, Sugiyama N. Histologic evaluation of lymphaticovenular anastomosis outcomes in the rat experimental model: comparison of cases with patency and obstruction. Plastic and reconstructive surgery. 2016;137(1):83e-91e. View
at Publisher |
View
at Google Scholar
Onoda S, Kimata Y, Matsumoto K. A Novel Lymphaticovenular Anastomosis Rat Model. Ann Plast Surg. Mar 2016;76(3):332-335. View
at Publisher |
View
at Google Scholar
Ruehm SG, Schroeder T, Debatin JrF. Interstitial MR lymphography with gadoterate meglumine: initial experience in humans. Radiology. 2001;220(3):816-821. View
at Publisher |
View
at Google Scholar
McKinnon JG, Wong V, Temple WJ, et al. Measurement of limb volume: laser scanning versus volume displacement. Journal of surgical oncology. 2007;96(5):381-388. View
at Publisher |
View
at Google Scholar
Suami H, Yamashita S, Soto-Miranda MA, Chang DW. Lymphatic territories (lymphosomes) in a canine: an animal model for investigation of postoperative lymphatic alterations. PloS one. 2013;8(7):e69222. View
at Publisher |
View
at Google Scholar
Campisi C, Michelini S, Boccardo F. Guidelines of the Societá Italiana di Linfangiologia: excerpted sections. Lymphology. 2004;37(4):182-184. View
at Publisher |
View
at Google Scholar
Damstra RJ, Halk A-B, Damstra R, et al. The Dutch lymphedema guidelines based on the International Classification of Functioning, Disability, and Health and the chronic care model. Journal of Vascular Surgery: Venous and Lymphatic Disorders. 2017;5(5):756-765. View
at Publisher |
View
at Google Scholar
Davies C, Levenhagen K, Ryans K, Perdomo M, Gilchrist L. Interventions for breast cancer–related lymphedema: clinical practice guideline from the academy of oncologic physical therapy of APTA. Physical therapy. 2020;100(7):1163-1179. View
at Publisher |
View
at Google Scholar
Gebruers N, Verbelen H, De Vrieze T, et al. Current and future perspectives on the evaluation, prevention and conservative management of breast cancer related lymphoedema: A best practice guideline. Vol 216: Elsevier; 2017:245-253. View
at Publisher |
View
at Google Scholar
McLaughlin SA, Staley AC, Vicini F, et al. Considerations for clinicians in the diagnosis, prevention, and treatment of breast cancer-related lymphedema: recommendations from a multidisciplinary expert ASBrS panel: part 1: definitions, assessments, education, and future directions. Annals of surgical oncology. 2017;24:2818-2826. View
at Publisher |
View
at Google Scholar
Lee B, Antignani PL, Baroncelli TA, et al. IUA-ISVI consensus for diagnosis guideline of chronic lymphedema of the limbs. Int Angiol. 2015;34(4):311-332. View
at Publisher |
View
at Google Scholar
Morgan P, Moffatt C. An update on the lymphoedema framework project. British Journal of Community Nursing. 2006;11(Sup5):S20-S21. View
at Publisher |
View
at Google Scholar
Perdomo M, Ryans K, Levenhagen K, Davies CC, Gilchrist L. Clinical implementation of the clinical practice guidelines for diagnosing upper-quadrant lymphedema secondary to cancer. Rehabilitation oncology. 2018;36(3):E11-E18. View
at Publisher |
View
at Google Scholar
Ridner SH, Dietrich MS, Boyages J, et al. A Comparison of Bioimpedance Spectroscopy or Tape Measure Triggered Compression Intervention in Chronic Breast Cancer Lymphedema Prevention. Lymphat Res Biol. Dec 2022;20(6):618-628. View
at Publisher |
View
at Google Scholar
Ramachandran S, Chew KY, Tan BK, Kuo YR. Current operative management and therapeutic algorithm of lymphedema in the lower extremities. Asian J Surg. Jan 2021;44(1):46-53. View
at Publisher |
View
at Google Scholar
Kung TA, Champaneria MC, Maki JH, Neligan PC. Current Concepts in the Surgical Management of Lymphedema. Plast Reconstr Surg. Apr 2017;139(4):1003e-1013e. View
at Publisher |
View
at Google Scholar
de Sire A, Losco L, Lippi L, et al. Surgical Treatment and Rehabilitation Strategies for Upper and Lower Extremity Lymphedema: A Comprehensive Review. Medicina (Kaunas). Jul 19 2022;58(7). View
at Publisher |
View
at Google Scholar
Armer JM, Ballman KV, McCall L, et al. Lymphedema symptoms and limb measurement changes in breast cancer survivors treated with neoadjuvant chemotherapy and axillary dissection: results of American College of Surgeons Oncology Group (ACOSOG) Z1071 (Alliance) substudy. Support Care Cancer. Feb 2019;27(2):495-503. View
at Publisher |
View
at Google Scholar
Masià J, Pons G, Rodríguez-Bauzà E. Barcelona lymphedema algorithm for surgical treatment in breast cancer–related lymphedema. Journal of Reconstructive Microsurgery. 2016;32(05):329-335. View
at Publisher |
View
at Google Scholar
Bolletta A, Kaciulyte J, Losco L, et al. The breast cancer-related lymphedema multidisciplinary approach: Algorithm for conservative and multimodal surgical treatment. Microsurgery. 2022. View
at Publisher |
View
at Google Scholar
Tillotson E, Thomson S, Pardo J, Granoff M, Yamamoto T, Singhal D. Improving the Patient Experience with Indocyanine Green Lymphography. Plastic and Reconstructive Surgery. 2022;150(5):1121e-1123e. View
at Publisher |
View
at Google Scholar
Pappalardo M, Lin C, Ho OA, Kuo CF, Lin CY, Cheng MH. Staging and clinical correlations of lymphoscintigraphy for unilateral gynecological cancer-related lymphedema. J Surg Oncol. Mar 2020;121(3):422-434. View
at Publisher |
View
at Google Scholar
Cheng M-H, Pappalardo M, Lin C, Kuo C-F, Lin C-Y, Chung KC. Validity of the novel Taiwan lymphoscintigraphy staging and correlation of Cheng lymphedema grading for unilateral extremity lymphedema. Annals of surgery. 2018;268(3):513-525. View
at Publisher |
View
at Google Scholar
Mihara M, Hara H, Araki J, et al. Indocyanine green (ICG) lymphography is superior to lymphoscintigraphy for diagnostic imaging of early lymphedema of the upper limbs. PloS one. 2012;7(6):e38182. View
at Publisher |
View
at Google Scholar
Al-Bustani S. A Prospective Analysis of 100 Consecutive Lymphovenous Bypass Cases for Treatment of Extremity Lymphedema. 50 Studies Every Plastic Surgeon Should Know. 2014:313. View
at Publisher |
View
at Google Scholar
Boyages J, Koelmeyer L, Suami H, et al. The ALERT model of care for the assessment and personalized management of patients with lymphoedema. Journal of British Surgery. 2020;107(3):238-247. View
at Publisher |
View
at Google Scholar
Patel KM, Lin C-Y, Cheng M-H. A prospective evaluation of lymphedema-specific quality-of-life outcomes following vascularized lymph node transfer. Annals of surgical oncology. 2015;22(7):2424-2430. View
at Publisher |
View
at Google Scholar
Jørgensen MG, Hermann AP, Madsen AR, Christensen S, Sørensen JA. Indocyanine green lymphangiography is superior to clinical staging in breast cancer-related lymphedema. Scientific Reports. 2021;11(1):1-9. View
at Publisher |
View
at Google Scholar
Tartaglione G, Ieria FP, Visconti G, et al. Rest/Stress Intradermal Lymphoscintigraphy for the Functional Imaging of the Lymphatic System. Clin Nucl Med. Dec 1 2022;47(12):1011-1018. View
at Publisher |
View
at Google Scholar
Jang S, Lee CU, Hesley GK, Knudsen JM, Brinkman NJ, Tran NV. Lymphatic Mapping Using US Microbubbles before Lymphaticovenous Anastomosis Surgery for Lymphedema. Radiology. Jul 2022;304(1):218-224. View
at Publisher |
View
at Google Scholar
Mohos B, Czedik-Eysenberg M, Steinbacher J, Tinhofer I, Meng S, Tzou CJ. Long-term Use of Ultrasound for Locating Optimal LVA Sites: A Descriptive Data Analysis. J Reconstr Microsurg. Mar 2022;38(3):238-244. View
at Publisher |
View
at Google Scholar
Visconti G, Hayashi A, Bianchi A, Tartaglione G, Bartoletti R, Salgarello M. Lymphaticovenular Anastomosis for Advanced-Stage Peripheral Lymphedema: Expanding Indication and Introducing the Hand/Foot Sign. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2022. View
at Publisher |
View
at Google Scholar
Pons G, Clavero J, Alomar X, Rodríguez-Bauza E, Tom L, Masia J. Preoperative planning of lymphaticovenous anastomosis: The use of magnetic resonance lymphangiography as a complement to indocyanine green lymphography. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2019;72(6):884-891. View
at Publisher |
View
at Google Scholar
Onoda S, Satake T, Hamada E. Super-microsurgery technique for lymphaticovenular anastomosis. Journal of Vascular Surgery: Venous and Lymphatic Disorders. Jan 2023;11(1):177-181. View
at Publisher |
View
at Google Scholar
Dip F, Lo Menzo E, Bouvet M, et al. Intraoperative fluorescence imaging in different surgical fields: Consensus among 140 intercontinental experts. Surgery. Dec 2022;172(6S):S54-S59. View
at Publisher |
View
at Google Scholar
Rebecca AM, Mahabir RC, Pflibsen L, Hillberg N, Jensen C, Casey WJ, 3rd. Indocyanine Green Lymphangiography as an Adjunct for the Optimal Identification and Management of Lymphatic Leaks in the Groin. J Reconstr Microsurg. Feb 2019;35(2):83-89. View
at Publisher |
View
at Google Scholar
Rodriguez JR, Yamamoto T. A Systematic Stepwise Method to Perform a Supermicrosurgical Lymphovenous Anastomosis. Ann Plast Surg. May 1 2022;88(5):524-532. View
at Publisher |
View
at Google Scholar
Yamamoto T, Narushima M, Doi K, et al. Characteristic indocyanine green lymphography findings in lower extremity lymphedema: the generation of a novel lymphedema severity staging system using dermal backflow patterns. Plast Reconstr Surg. May 2011;127(5):1979-1986. View
at Publisher |
View
at Google Scholar
Yang JC, Wu SC, Hayashi A, et al. Selection of Optimal Functional Lymphatic Vessel Cutoff Size in Supermicrosurgical Lymphaticovenous Anastomosis in Lower Extremity Lymphedema. Plast Reconstr Surg. Jan 1 2022;149(1):237-246. View
at Publisher |
View
at Google Scholar
Visconti G, Salgarello M, Hayashi A. The Recipient Venule in Supermicrosurgical Lymphaticovenular Anastomosis: Flow Dynamic Classification and Correlation with Surgical Outcomes. J Reconstr Microsurg. Oct 2018;34(8):581-589. View
at Publisher |
View
at Google Scholar
Bianchi A, Salgarello M, Hayashi A, Yang JC, Visconti G. Recipient Venule Selection and Anastomosis Configuration for Lymphaticovenular Anastomosis in Extremity Lymphedema: Algorithm Based on 1,000 Lymphaticovenular Anastomosis. J Reconstr Microsurg. Jul 2022;38(6):472-480. View
at Publisher |
View
at Google Scholar
Guyton AC, and John Edward Hall. . Vascular Distensibility and Functions of the Arterial and Venous Systems. Textbook of medical physiology. Vol Vol. 548. Philadelphia: Saunders; 1986. View
at Publisher |
View
at Google Scholar
Furuya M, Yamamoto T, Yamashita M, Hayashi A. The half notching method for Flow-through lymphaticovenular anastomosis. Microsurgery. Jul 2015;35(5):415-416. View
at Publisher |
View
at Google Scholar
Ayestaray B, Bekara F. pi-shaped lymphaticovenular anastomosis: the venous flow sparing technique for the treatment of peripheral lymphedema. J Reconstr Microsurg. Oct 2014;30(8):551-560. View
at Publisher |
View
at Google Scholar
Yamamoto T, Yoshimatsu H, Narushima M, et al. Sequential anastomosis for lymphatic supermicrosurgery: multiple lymphaticovenular anastomoses on 1 venule. Ann Plast Surg. Jul 2014;73(1):46-49. View
at Publisher |
View
at Google Scholar
Yamamoto T, Yamamoto N, Kageyama T, et al. Technical pearls in lymphatic supermicrosurgery. Glob Health Med. Feb 29 2020;2(1):29-32. View
at Publisher |
View
at Google Scholar
Onoda S, Satake T, Hamada E. Super-microsurgery technique for lymphaticovenular anastomosis. Journal of Vascular Surgery: Venous and Lymphatic Disorders. 2022. View
at Publisher |
View
at Google Scholar
Yamamoto T, Yoshimatsu H, Narushima M, et al. A modified side-to-end lymphaticovenular anastomosis. Microsurgery. Feb 2013;33(2):130-133. View
at Publisher |
View
at Google Scholar
Kwon JG, Jeong S, Pak CJ, Suh HP, Hong JP. Comparative Analysis between Side-to-End and End-to-End Lymphaticovenous Anastomosis for Secondary Lower Limb Lymphedema. Plast Reconstr Surg. Nov 1 2022;150(5):1138-1148. View
at Publisher |
View
at Google Scholar
Yamamoto T, Kikuchi K, Yoshimatsu H, Koshima I. Ladder-shaped lymphaticovenular anastomosis using multiple side-to-side lymphatic anastomoses for a leg lymphedema patient. Microsurgery. Jul 2014;34(5):404-408. View
at Publisher |
View
at Google Scholar
Yamamoto T. Comment: Selection of anastomosis type for lymphaticovenular anastomosis. J Plast Reconstr Aesthet Surg. Feb 2013;66(2):207-208. View
at Publisher |
View
at Google Scholar
Yamamoto T, Narushima M, Kikuchi K, et al. Lambda-shaped anastomosis with intravascular stenting method for safe and effective lymphaticovenular anastomosis. Plast Reconstr Surg. May 2011;127(5):1987-1992. View
at Publisher |
View
at Google Scholar
Fuse Y, Yamamoto T. Diamond-shaped anastomosis for supermicrosurgical side-to-side lymphaticovenular anastomosis. J Plast Reconstr Aesthet Surg. Dec 2015;68(12):e209-210. View
at Publisher |
View
at Google Scholar
Fuse Y, Yamamoto T. Half notching method for supermicrosurgical lambda-shaped lymphaticovenular anastomosis. J Plast Reconstr Aesthet Surg. Jan 2016;69(1):e13-14. View
at Publisher |
View
at Google Scholar
Kannan RY, Koshima I. A Case-control Analysis of the Knight's Move Technique in a Chicken Wing Microsurgery Model: Video Article. Plast Reconstr Surg Glob Open. Mar 2021;9(3):e3476. View
at Publisher |
View
at Google Scholar
Boccardo F, Casabona F, De Cian F, et al. Lymphatic microsurgical preventing healing approach (LYMPHA) for primary surgical prevention of breast cancer-related lymphedema: over 4 years follow-up. Microsurgery. Sep 2014;34(6):421-424. View
at Publisher |
View
at Google Scholar
Yamamoto Y, Horiuchi K, Sasaki S, et al. Follow-up study of upper limb lymphedema patients treated by microsurgical lymphaticovenous implantation (MLVI) combined with compression therapy. Microsurgery. 2003;23(1):21-26. View
at Publisher |
View
at Google Scholar
Yamamoto T, Chen WF, Yamamoto N, Yoshimatsu H, Tashiro K, Koshima I. Technical simplification of the supermicrosurgical side-to-end lymphaticovenular anastomosis using the parachute technique. Microsurgery. Feb 2015;35(2):129-134. View
at Publisher |
View
at Google Scholar
Furukawa H, Osawa M, Saito A, et al. Microsurgical lymphaticovenous implantation targeting dermal lymphatic backflow using indocyanine green fluorescence lymphography in the treatment of postmastectomy lymphedema. Plast Reconstr Surg. May 2011;127(5):1804-1811. View
at Publisher |
View
at Google Scholar
Demirtas Y, Ozturk N, Yapici O, Topalan M. Comparison of primary and secondary lower-extremity lymphedema treated with supermicrosurgical lymphaticovenous anastomosis and lymphaticovenous implantation. J Reconstr Microsurg. Feb 2010;26(2):137-143. View
at Publisher |
View
at Google Scholar
Demirtas Y, Ozturk N, Yapici O, Topalan M. Supermicrosurgical lymphaticovenular anastomosis and lymphaticovenous implantation for treatment of unilateral lower extremity lymphedema. Microsurgery. 2009;29(8):609-618. View
at Publisher |
View
at Google Scholar
Yamamoto Y, Sugihara T. Microsurgical lymphaticovenous implantation for the treatment of chronic lymphedema. Plast Reconstr Surg. Jan 1998;101(1):157-161. View
at Publisher |
View
at Google Scholar
Ishiura R, Yamamoto T, Saito T, Mito D, Iida T. Comparison of Lymphovenous Shunt Methods in a Rat Model: Supermicrosurgical Lymphaticovenular Anastomosis versus Microsurgical Lymphaticovenous Implantation. Plast Reconstr Surg. Jun 2017;139(6):1407-1413. View
at Publisher |
View
at Google Scholar
Milasan A, Farhat M, Martel C. Extracellular Vesicles as Potential Prognostic Markers of Lymphatic Dysfunction. Front Physiol. 2020;11:476. View
at Publisher |
View
at Google Scholar
Friedman R, Bustos VP, Postian T, et al. Utilizing a lower extremity vein graft for immediate lymphatic reconstruction. J Plast Reconstr Aesthet Surg. Aug 2022;75(8):2831-2870. View
at Publisher |
View
at Google Scholar
Onoda S, Satake T, Kinoshita M. Relationship Between Lymphaticovenular Anastomosis Outcomes and the Number and Types of Anastomoses. J Surg Res. Jan 2022;269:103-109. View
at Publisher |
View
at Google Scholar
Campisi CC, Ryan M, Boccardo F, Campisi C. A Single-Site Technique of Multiple Lymphatic-Venous Anastomoses for the Treatment of Peripheral Lymphedema: Long-Term Clinical Outcome. J Reconstr Microsurg. Jan 2016;32(1):42-49. View
at Publisher |
View
at Google Scholar
Spoer D, Berger L, Towfighi P, et al. Lymphovenous Coupler-Assisted Bypass (CAB) for Immediate Lymphatic Reconstruction: MedStar Georgetown University Hospital; 2022. View
at Publisher |
View
at Google Scholar
Sisk GC, Shuck JW, Lopez M, Chang EI. Lymphovenous anastomosis using the venous coupler. J Plast Reconstr Aesthet Surg. May 2020;73(5):983-1007. View
at Publisher |
View
at Google Scholar
Jing W, Narushima M. Half-transection method combined with intravascular stent for supermicrosurgical lymphaticovenular anastomosis. J Plast Reconstr Aesthet Surg. Dec 2018;71(12):1816-1834. View
at Publisher |
View
at Google Scholar
Nuri T, Ueda K, Yamada A, Hara M. Preparatory intravascular stenting technique: an easier method of supermicrosurgical lymphaticovenular anastomosis. Ann Plast Surg. Nov 2013;71(5):541-543. View
at Publisher |
View
at Google Scholar
Yamamoto T, Yoshimatsu H, Yamamoto N, Narushima M, Iida T, Koshima I. Side-to-End Lymphaticovenular Anastomosis through Temporary Lymphatic Expansion. PLoS ONE. 2013-03-25 2013;8(3):e59523. View
at Publisher |
View
at Google Scholar
Sharma P, Sharma H, St Cyr M, Griffiths M. Never fear the venous-lymphatic coupler is here! J Plast Reconstr Aesthet Surg. Feb 2015;68(2):290-291. View
at Publisher |
View
at Google Scholar
Rezkalla J, Husain M, Slack G, Sinha S. Novel use of a Synovis™ coupler device for a surgical lymphovenous anastomosis for the treatment of refractory chylothorax in a patient with central lymphatic flow disorder. Clinical Case Reports. 2022-03-01 2022;10(3). View
at Publisher |
View
at Google Scholar
Jabbour S, Chang EI. Recent advancements in supermicrosurgical treatment of lymphedema. Plastic and Aesthetic Research. 2021. View
at Publisher |
View
at Google Scholar
Jakub J, Ramaker S. Preventing Lymphedema in Axillary Lymph Node Dissection: Mayo Clinic in Florida, Jacksonville, Florida, United States|Mayo Clinic in Rochester, Rochester, Minnesota, United States; 2018. View
at Publisher |
View
at Google Scholar
Lymphovenous Bypass Procedure Before Underarm Lymph Node Surgery in Preventing Lymphedema in Patients With Inflammatory or Locally Advanced Non-inflammatory Breast: M D Anderson Cancer Center, Houston, Texas, United States. View
at Publisher |
View
at Google Scholar
Boccardo F, Valenzano M, Costantini S, et al. LYMPHA Technique to Prevent Secondary Lower Limb Lymphedema. Annals of Surgical Oncology. 2016-10-01 2016;23(11):3558-3563. View
at Publisher |
View
at Google Scholar
Boccardo FM, Casabona F, Friedman D, et al. Surgical Prevention of Arm Lymphedema After Breast Cancer Treatment. Annals of Surgical Oncology. 2011-09-01 2011;18(9):2500-2505. View
at Publisher |
View
at Google Scholar
Boccardo F, Casabona F, De Cian F, et al. Lymphedema Microsurgical Preventive Healing Approach: A New Technique for Primary Prevention of Arm Lymphedema After Mastectomy. Annals of Surgical Oncology. 2009-03-01 2009;16(3):703-708. View
at Publisher |
View
at Google Scholar
Levy AS, Murphy AI, Ishtihar S, et al. “Lymphatic Microsurgical Preventive Healing Approach (LYMPHA) for the Primary Prevention of Lymphedema: A 4-year Follow-up Matched Cohort Study”. Plastic and Reconstructive Surgery. 9900:10.1097/PRS.0000000000009857. View
at Publisher |
View
at Google Scholar
Feldman S, Bansil H, Ascherman J, et al. Single Institution Experience with Lymphatic Microsurgical Preventive Healing Approach (LYMPHA) for the Primary Prevention of Lymphedema. Annals of Surgical Oncology. 2015-10-01 2015;22(10):3296-3301. View
at Publisher |
View
at Google Scholar
Hahamoff M, Gupta N, Munoz D, et al. A Lymphedema Surveillance Program for Breast Cancer Patients Reveals the Promise of Surgical Prevention. J Surg Res. Dec 2019;244:604-611. View
at Publisher |
View
at Google Scholar
Squitieri L, Rasmussen PW, Patel KM. An economic analysis of prophylactic lymphovenous anastomosis among breast cancer patients receiving mastectomy with axillary lymph node dissection. J Surg Oncol. Jun 2020;121(8):1175-1178. View
at Publisher |
View
at Google Scholar
Chiang SN, Skolnick GB, Westman AM, Sacks JM, Christensen JM. National Outcomes of Prophylactic Lymphovenous Bypass during Axillary Lymph Node Dissection. J Reconstr Microsurg. Oct 2022;38(8):613-620. View
at Publisher |
View
at Google Scholar
Johnson AR, Fleishman A, Granoff MD, et al. Evaluating the Impact of Immediate Lymphatic Reconstruction for the Surgical Prevention of Lymphedema. Plast Reconstr Surg. Mar 1 2021;147(3):373e-381e. View
at Publisher |
View
at Google Scholar
Yoshida S, Koshima I, Imai H, et al. Line production system for multiple lymphaticovenular anastomoses. J Plast Reconstr Aesthet Surg. Aug 2019;72(8):1334-1339. View
at Publisher |
View
at Google Scholar
Center MSKC. “About Your Lymphovenous Bypass (LVB) Surgery for Lymphedema.” 1 Jan. 1970; www.mskcc.org/cancer-care/patient-education/about-your-lymphovenous-bypass-lvb-surgery-lymphedema. View
at Publisher |
View
at Google Scholar
Chan JCY, Taranto GD, Elia R, Amorosi V, Sitpahul N, Chen HC. Postoperative care after lymphaticovenous anastomosis. Arch Plast Surg. May 2021;48(3):333-335. View
at Publisher |
View
at Google Scholar
Cornelissen AJ, Beugels J, Ewalds L, et al. Effect of lymphaticovenous anastomosis in breast cancer-related lymphedema: a review of the literature. Lymphatic Research and Biology. 2018;16(5):426-434. View
at Publisher |
View
at Google Scholar
Batista BN, Germain M, Faria JCM, Becker C. Lymph node flap transfer for patients with secondary lower limb lymphedema. Microsurgery. 2017;37(1):29-33. View
at Publisher |
View
at Google Scholar
Vicini F, Shah C, Whitworth P, Walker M, Shi J. Correlation of bioimpedance spectroscopy with risk factors for the development of breast cancer-related lymphedema. Lymphatic research and biology. 2018;16(6):533-537. View
at Publisher |
View
at Google Scholar
Marchica P, D'Arpa S, Magno S, et al. Integrated Treatment of Breast Cancer-related Lymphedema: A Descriptive Review of the State of the Art. Anticancer Res. Jul 2021;41(7):3233-3246. View
at Publisher |
View
at Google Scholar
Kong X, Du J, Du X, Cong X, Zhao Q. A Meta-analysis of 37 Studies on the Effectiveness of Microsurgical Techniques for Lymphedema. Annals of Vascular Surgery. 2022-10-01 2022;86:440-451.e446. View
at Publisher |
View
at Google Scholar
Johnson AR, Kimball S, Epstein S, et al. Lymphedema Incidence After Axillary Lymph Node Dissection: Quantifying the Impact of Radiation and the Lymphatic Microsurgical Preventive Healing Approach. Ann Plast Surg. Apr 2019;82(4S Suppl 3):S234-S241. View
at Publisher |
View
at Google Scholar
Chun MJ, Saeg F, Meade A, et al. Immediate Lymphatic Reconstruction for Prevention of Secondary Lymphedema: A Meta-Analysis. J Plast Reconstr Aesthet Surg. Mar 2022;75(3):1130-1141. View
at Publisher |
View
at Google Scholar
Weiss J, Daniel T. Validation of the lymphedema life impact scale (LLIS): a condition-specific measurement tool for persons with lymphedema. Lymphology. 2015;48(3):128-138. View
at Publisher |
View
at Google Scholar
Devoogdt N, Van Kampen M, Geraerts I, Coremans T, Christiaens M-R. Lymphoedema Functioning, Disability and Health questionnaire (Lymph-ICF): reliability and validity. Physical therapy. 2011;91(6):944-957. View
at Publisher |
View
at Google Scholar
Devoogdt N, De Groef A, Hendrickx A, et al. Lymphoedema functioning, disability and health questionnaire for lower limb lymphoedema (lymph-ICF-LL): reliability and validity. Physical therapy. 2014;94(5):705-721. View
at Publisher |
View
at Google Scholar
Blome C, Augustin M, Heyer K, et al. Evaluation of patient-relevant outcomes of lymphedema and lipedema treatment: development and validation of a new benefit tool. European Journal of Vascular and Endovascular Surgery. 2014;47(1):100-107. View
at Publisher |
View
at Google Scholar
Duygu E, Bakar Y, Keser I. An important tool in lymphedema management: validation of Turkish version of the patient benefit index-lymphedema. Lymphatic Research and Biology. 2020;18(1):49-55. View
at Publisher |
View
at Google Scholar
Viehoff P, Van Genderen F, Wittink H. Upper limb lymphedema 27 (ULL27): Dutch translation and validation of an illness-specific health-related quality of life questionnaire for patients with upper limb lymphedema. Lymphology. 2008;41(3):131-138. View
at Publisher |
View
at Google Scholar
Chen WF, Eid A, Yamamoto T, Keith J, Nimmons GL, Lawrence WT. A novel supermicrosurgery training model: the chicken thigh. J Plast Reconstr Aesthet Surg. Jul 2014;67(7):973-978. View
at Publisher |
View
at Google Scholar
Hayashi K, Hattori Y, Yii Chia DS, Sakamoto S, Marei A, Doi K. A supermicrosurgery training model using the chicken mid and lower wing. J Plast Reconstr Aesthet Surg. Jun 2018;71(6):943-945. View
at Publisher |
View
at Google Scholar
Mukarramah DA, Tsukuura R, Kageyama T, et al. Side-to-side supermicrosurgical anastomosis training using chicken wing model with V-shaped traction method. Microsurgery. Mar 2021;41(3):300-301. View
at Publisher |
View
at Google Scholar
Bayramicli M, Sirinoglu H, Yalcin D. A basic experimental model for end-to-end anastomosis of vessels with diameter discrepancy. Microsurgery. May 2014;34(4):333-334. View
at Publisher |
View
at Google Scholar
Jamalian S, Jafarnejad M, Zawieja SD, et al. Demonstration and Analysis of the Suction Effect for Pumping Lymph from Tissue Beds at Subatmospheric Pressure. Sci Rep. Sep 21 2017;7(1):12080. View
at Publisher |
View
at Google Scholar
Roh K, Cho S, Park JH, et al. Therapeutic effects of hyaluronidase on acquired lymphedema using a newly developed mouse limb model. Exp Biol Med (Maywood). Mar 2017;242(6):584-592. View
at Publisher |
View
at Google Scholar
Hayashida K, Yoshida S, Yoshimoto H, et al. Adipose-Derived Stem Cells and Vascularized Lymph Node Transfers Successfully Treat Mouse Hindlimb Secondary Lymphedema by Early Reconnection of the Lymphatic System and Lymphangiogenesis. Plast Reconstr Surg. Mar 2017;139(3):639-651. View
at Publisher |
View
at Google Scholar
Will PA, Rafiei A, Pretze M, et al. Evidence of stage progression in a novel, validated fluorescence-navigated and microsurgical-assisted secondary lymphedema rodent model. PLoS One. 2020;15(7):e0235965. View
at Publisher |
View
at Google Scholar
Weiler MJ, Cribb MT, Nepiyushchikh Z, Nelson TS, Dixon JB. A novel mouse tail lymphedema model for observing lymphatic pump failure during lymphedema development. Sci Rep. Jul 18 2019;9(1):10405. View
at Publisher |
View
at Google Scholar
Yang CY, Nguyen DH, Wu CW, et al. Developing a Lower Limb Lymphedema Animal Model with Combined Lymphadenectomy and Low-dose Radiation. Plast Reconstr Surg Glob Open. Mar 2014;2(3):e121. View
at Publisher |
View
at Google Scholar
Ogino R, Hayashida K, Yamakawa S, Morita E. Adipose-Derived Stem Cells Promote Intussusceptive Lymphangiogenesis by Restricting Dermal Fibrosis in Irradiated Tissue of Mice. Int J Mol Sci. May 29 2020;21(11). View
at Publisher |
View
at Google Scholar
Daneshgaran G, Lo AY, Paik CB, et al. A Pre-clinical Animal Model of Secondary Head and Neck Lymphedema. Sci Rep. Dec 4 2019;9(1):18264. View
at Publisher |
View
at Google Scholar
Tran BNN, Angelo JP, Lee JH, et al. A novel pilot animal model for the surgical prevention of lymphedema: the power of optical imaging. J Surg Res. Jan 2018;221:285-292. View
at Publisher |
View
at Google Scholar
Chang DW, Suami H, Skoracki R. A prospective analysis of 100 consecutive lymphovenous bypass cases for treatment of extremity lymphedema. Plast Reconstr Surg. Nov 2013;132(5):1305-1314. View
at Publisher |
View
at Google Scholar
Sacchi G, Weber E, Agliano M, Raffaelli N, Comparini L. The structure of superficial lymphatics in the human thigh: precollectors. Anat Rec. Jan 1997;247(1):53-62. View
at Publisher |
View
at Google Scholar
Scavelli C, Weber E, Agliano M, et al. Lymphatics at the crossroads of angiogenesis and lymphangiogenesis. J Anat. Jun 2004;204(6):433-449. View
at Publisher |
View
at Google Scholar
Lampejo AO, Hu NW, Lucas D, et al. A Challenge for Engineering Biomimetic Microvascular Models: How do we Incorporate the Physiology? Front Bioeng Biotechnol. 2022;10:912073. View
at Publisher |
View
at Google Scholar
Taylor GI, Caddy CM, Watterson PA, Crock JG. The venous territories (venosomes) of the human body: experimental study and clinical implications. Plast Reconstr Surg. Aug 1990;86(2):185-213. View
at Publisher |
View
at Google Scholar
Dear Editorial Team,
Clinical Medical Reviews and Reports.
My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal.
Best wishes from,
Elena Popa.
Dr Elena Popa
It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.
Dr Nikolaos Andreas Chrysanthakopoulos
Dear Grace Pierce,
Editorial Coordinator of Journal of Clinical Research and Reports,
Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future.
Best wishes from,
Robert W. McGee
Robert W McGee
Dear Grace Pierce,
Editorial Coordinator of Journal of Clinical Research and Reports,
Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal.
Best wishes from,
DR Aibing Rao, Head of R&D
Aibing Rao
I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.
Kashani Mehdi
Dear Mercy Grace,
Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences,
We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage.
We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences!
Best wishes from,
Alla Konstantinovna Politova,