
Case Report | DOI: https://doi.org/10.31579/2768-2757/125
General Surgery Service – Clínica CMIC. Neuquén, Argentina.
*Corresponding Author: Pablo D. San Martín, General Surgery Service – Clínica CMIC. Neuquén, Argentina.
Citation: Pablo D. San Martín, (2024), Surgical technique: "initial experience in videolaparoscopic percutaneous hybrid cholecystectomy (vphch)", Journal of Clinical Surgery and Research, 5(5); DOI:10.31579/2768-2757/125
Copyright: © 2024, Pablo D. San Martín. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 April 2024 | Accepted: 19 June 2024 | Published: 18 July 2024
Keywords: cholecystectomy; gallbladder; cholecystectomy without traces; hybrid cholecystectomy; laparoscopic cholecystectomy; percutaneous cholecystectomy
Introduction. Since the first laparoscopic cholecystectomy, less and less invasive techniques have been developed. Currently, it is possible to introduce multiple instruments into the abdominal cavity, with smaller and smaller diameters, and Hybrid Percutaneous Videolaparoscopic Cholecystectomy, a mini-laparoscopic technique, results in less visible scars.
Material and methods. A technical modification of laparoscopic cholecystectomy using percutaneous accesses with trocars, needles for the assembly of laparoscopic instruments in association with traditional instruments is described.
Results
A total of 39 successfully scheduled laparoscopic percutaneous hybrid cholecystectomies were performed in patients of both sexes of different ages with cholecystopathies. The surgeries were performed in an average time of 45 minutes, and there were no intraoperative or postoperative complications.
Conclusion
Videolaparoscopic Percutaneous Hybrid Cholacystectomy is an alternative technique that safely and effectively modifies traditional laparoscopy, has more satisfactory cosmetic results, and is potentially reproducible.
Increasingly frequent technological advances and innovations allow the development of multiple surgical techniques with a laparoscopic approach. The miniaturization and higher resolution of video cameras and monitors allowed them to be incorporated into the operative field in an almost imperceptible way, expanding the applications of laparoscopic surgery. Since Erich Müler, in 1985, developed the galloscope and performed the first laparoscopic cholecystectomy [1], surgery has focused on the development of increasingly less invasive techniques. Currently, it is possible to introduce multiple instruments into the abdominal cavity, with smaller and smaller diameters, and videolaparoscopic percutaneous hybrid cholecystectomy (VPHCh), a variant of the minilaparoscopic technique, aims to minimize morbidity with aesthetic results, which leave scars less and less visible, achieving procedures without traces, with the hybrid use of access ports by means of 3 mm diameter trocars-needles mounted by heads with laparoscopic instruments of 8 mm diameter [2] associated with traditional laparoscopic access ports of 5 or 10 mm diameter.
Retrospective review of cholecystectomies performed in the General Surgery Service of the CMIC Clinic in the city of Neuquén, and description of the videolaparoscopic percutaneous hybrid surgical approach. The patient is placed in dorsal decubitus with an inverted Trendelenburg position, the surgeon is placed on the left side with an assistant, and the surgical instrument on the right side with a possible second assistant; A monitor is placed on both sides. After asepsis, antisepsis and placement of sterile drapes, a 10 mm arciform incision is made in the superior umbilical fold, divulsion of the subcutaneous cellular tissue and opening of the umbilical fascia, it is placed under direct vision of a 10 mm blunt trocar, according to Hasson's open technique, the first laparoscopic access is achieved. Pneumoperitoneum is performed with insufflation of the abdominal cavity with carbon dioxide (CO2), maintained at an intra-abdominal pressure of 12-14 mmHg during surgery.
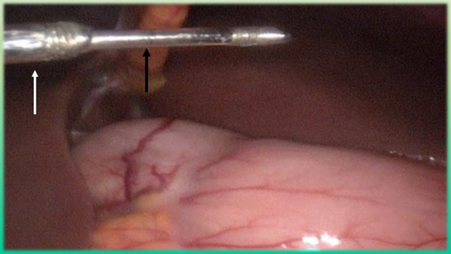
Figure 2:The laparoscope is introduced through the umbilical access, and a videolaparoscopic examination of the abdominal cavity is systematically initiated; A second 5 mm access is placed in the epigastric region under direct vision, and 3 mm percutaneous accesses are placed in the right subcostal region: medial trocar-needle below the costal rim at the level of the midclavicular line (image 1) and lateral trocar-needle above the anterosuperior iliac spine at the level of the anterior axillary line.
| Image 2. Intraoperative imaging. Externalization of the trocar-needle through the umbilical access. | |
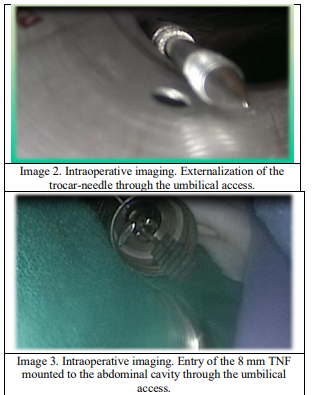 | |
| Image 3. Intraoperative imaging. Entry of the 8 mm TNF mounted to the abdominal cavity through the umbilical access. | |
Figure 3: Positioned by direct videolaparoscopic vision, the trocar-needle is externalized through the umbilical access (image 2), and extracorporeal the head is mounted with laparoscopic instruments (grasping forceps, dissector forceps) of 8 mm, armed the percutaneous trocar-needle-forceps (TNF) instruments are introduced into the abdominal cavity (2) (image 3).
According to the experience of the surgical team, VHPCh is performed with one or two TNF accesses, we will use the term four-access technique (4AT) when two TNF are used and three-access technique (3AT) when only one TNF is used.
In 4AT, the laparoscopic surgeon with a forceps in his right hand presents the vesicular fundus, the assistant with the lateral TNF pulls it towards the cephalic, dislocating the liver and exposing the gallbladder bed. With the medial TNF in your left hand, the surgeon pulls the bacinette out and down by unfolding Calot's triangle for pedicle dissection.
In 3AT, the surgeon takes the gallbladder fundus with his right hand, pulls it towards the cephalic, dislocating the liver and exposing the vesicular bed; With the TNF in his left hand, he pulls the drumstick outward and downward, unfolding Calot's triangle, and frees his right hand to continue with the pedicle dissection.
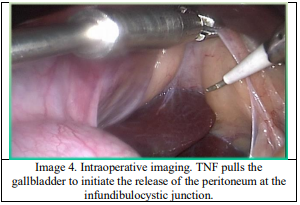 |
| Image 4. Intraoperative imaging. TNF pulls the gallbladder to initiate the release of the peritoneum at the infundibulocystic junction. |
Figure 4: In both techniques, the bacinette is pulled left and up with a TNF to begin with the release of the vesicular peritoneum through its surgical side at the infundibulocystic junction (image 4).
Imagen 5. Intraoperative imaging. Traction is observed with the TNF for identification of the pedicle elements. Cystic duct (white arrow). Cystic artery (black arrow). Lateroccystic ganglion at the tip of the dissectoral forceps.
Dynamic C-arm intraoperative cholangiography (IOC) can be performed systematically or selectively depending on the experience of the surgical team (3). Cysticotomy is performed, after performing an intra- or extracorporeal knot, leaving a redundant rope of 5-6 cm that will facilitate the ectomy; IOC is performed according to the forceps technique for cholangiography by the epigastric trocar or by percutaneous puncture under the costal ridge in projection of the cystic duct. the cystic duct.
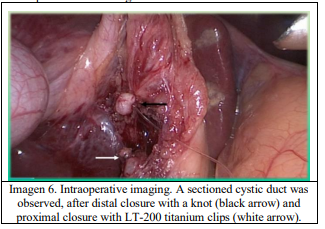 |
| Imagen 6. Intraoperative imaging. A sectioned cystic duct was observed, after distal closure with a knot (black arrow) and proximal closure with LT-200 titanium clips (white arrow). |
Figure 6: The cystic duct is closed with LT-200 titanium clips below the cysticostomy positioned with a 5 mm clipper or knots (intra or extraporcorporeal) or preformed loops (endoloop); The duct is cut with scissors (image 6).
The cystic artery is skeletonized, obliterated with LT-200 titanium clips, and sectioned.
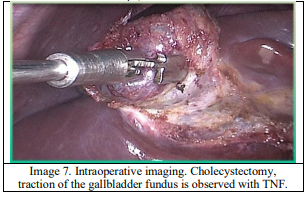 |
| Image 7. Intraoperative imaging. Cholecystectomy, traction of the gallbladder fundus is observed with TNF. |
Figure 7: Cholecystectomy is completed with monopolar hook or scissor electrocoagulation; the vesicular peritoneum is exposed for dissection at 4AT by traction and contraction of the medial and lateral TNF, which take bacinette and vesicular fundus, respectively; in 3AT by traction of the TNF, alternating position between bacinete and vesicular fundus (imagen 7).
Once the gallbladder is freed from its bed, it is washed and aspirated, and hemostasis is controlled.
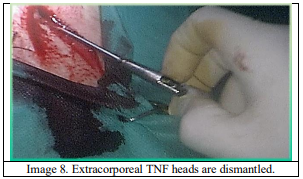 |
| Image 8. Extracorporeal TNF heads are dismantled. |
Figure 8: The vesicular ectomy is performed through the umbilical trocar, pulling it through the end of the distal knot of the cysticostomy for its externalization; If necessary, the gallbladder contents are extracted. In cases of gallbladder rupture, acute inflammatory processes or suspected neoplasms, an insulating bag is used for extraction.
Once the vesicular extraction was completed, the umbilical access was repositioned to externalize the TNF and disassemble the heads (image 8), under videolaparoscopic vision, the trocar-needle and the epigastric trocar were removed.
 |
| Image 9. Intraoperative image of the left, the aesthetic result with the closure of the incisions with polyglactin can be observed. Image on the right: aesthetic result in postoperative period of more than 5 years. |
Figure 9: The umbilical fascia is closed with 0-gauge polyglactin-910 suture; Skin synthesis of umbilical and epigastric incisions with 3-0-gauge polyglactin-910 intradermal suture (image 9).
A total of 39 scheduled VPHChs were successfully performed in patients of both sexes aged 19-73 years, with symptomatic cholecystopathies (lithiasis or polyps) with different times of evolution. The surgeries were performed in an average time of 45 (37–53) minutes, were performed by the same surgeon, and there were no intraoperative or postoperative complications. No conversion to traditional laparoscopy or open surgery was necessary. In 3 cases, intraoperative cholangiography was performed due to alteration of liver enzymes in the preoperative period. Patients began oral tolerance and ambulation on the day of surgery, hospitalization extended between 12-24 hours. Postoperative follow-up began on an outpatient basis one week after surgery, with subsequent follow-ups until six months, with good aesthetic satisfaction of the procedure (Figure 9).
The hybrid percutaneous videolaparoscopic technique is an innovative procedure potentially practicable by other surgical specialties, it is currently a technique under development. VPHCh is characterized using traditional laparoscopic instruments associated with minimally invasive TNF (trocar-needle-forceps) complexes. VPHCh can be performed by laparoscopic surgeons who are familiar with laparoscopic techniques in general, and cholecystectomy in particular; It comes with the caveat of being able to add more access ports, or even convert it to a traditional laparoscopic procedure using the same approach incisions. The advantages of VPHCh, for its implementation as a modification of the traditional technique or other minimally invasive techniques, are:
The hybrid percutaneous videolaparoscopic technique presents technical challenges at the time of admission of TNFs that require the coordination of the surgical team to avoid injury to abdominal organs.
CHPV is an alternative minilaparoscopic technique that safely and effectively modifies traditional laparoscopy, TNFs allow the seizure of organs with greater grip force than other minilaparoscopic forceps, with highly satisfactory cosmetic results, and the possibility of hospitalization in short-stay services (8) without an overnight stay. It is a potentially reproducible technique that aims to simplify the traditional technique. The hybrid percutaneous videolaparoscopic technique is innovative and has a wide field of progress in general surgery and in other specialties; It is necessary to expand the development of specific instruments, improving their quality, for this approach.
There are no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
