
Case Report | DOI: https://doi.org/10.31579/2641-0419/179
1Cardiothoracic surgeon, Narayana Institute of Cardiac Sciences
2Cardiothoracic surgeon, Narayana Institute of Cardiac Sciences
3Senior Consultant Cardiothoracic Surgery, Narayana Institute of Cardiac Sciences
*Corresponding Author: Ameya Kaskar, Department of Cardio-Thoracic Surgery, Narayana Institute of Cardiac Sciences, Narayana Health, #258/A, Bommasandra Industrial Area, Anekal Taluk,Bangalore-560099, Karnataka, India.
Citation: Deepak V Bohra, Ameya Kaskar, Priyankar Sinha. (2021) Surgical repair of Unruptured Pseudoaneurysm of Sinus of Valsalva in Aortic Stenosis. J. Clinical Cardiology and Cardiovascular Interventions, 4(12); Doi:10.31579/2641-0419/179
Copyright: © 2021 Ameya Kaskar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 April 2021 | Accepted: 18 June 2021 | Published: 23 June 2021
Keywords: aortic stenosis; transthoracic echocardiography
Isolated pseudoaneurysm of a sinus of Valsalva is an uncommon sequelae of infective endocarditis. It is very uncommon in native aortic valve stenosis as compared to aortic regurgitation. We present a case of a 46 year old gentleman with a severely stenotic aortic valve with infective endocarditis, and a pseudoaneurysm of the non coronary sinus of Valsalva. The pseudoaneurysm was repaired with a prosthetic patch and the aortic valve was replaced by a mechanical prosthesis. Transthoracic echocardiography and computed tomography aortogram are an ideal diagnostic tools in suspected cases. Surgery can be curative with excellent results.
Running Title : Sinus of Valsalva Pseudoaneurysm
Pseudoaneurysm of the native aortic sinus of valsalva is an uncommon condition which occurs spontaneously or secondary to infection, trauma [1]. Infective endocarditis can lead to many complications like abscess formation, pseudoaneurysms and aortocavitary fistula formation with lethal effects. These complications can occur in a preexisting diseased or normal valve. It can form aortocavitary fistulae with adjacent cardiac chambers [2]. We report a case of a severely stenotic aortic valve with infective endocarditis and pseudoaneurysm of the non coronary sinus of Valsalva (NCSOV) with a successful surgical cure.
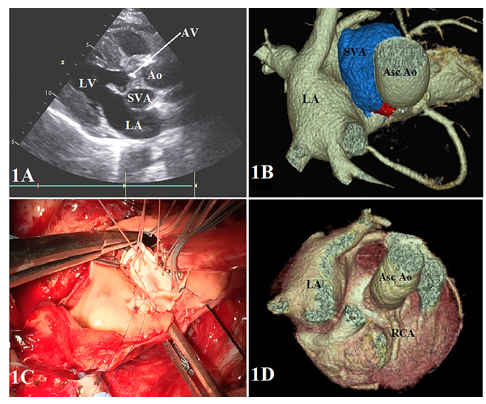
A 46 year old gentleman presented with worsening angina and dyspnea on exertion for one year. He also had history of fever one month back for which he had received intravenous cefepime for 2 weeks. A fortnight later he came to our institute. Clinical examination showed a normal hemodynamic status with a pulse rate of 82/min, blood pressure of 108/60 mm of Hg and a grade III/VI ejection systolic murmur over right sternal border. Blood cultures were negative and other hematological, biochemical and radiological investigations were satisfactory. Transthoracic echocardiography (TTE) revealed thickened aortic leaflets with multiple echogenic nodules, suggestive of healed vegetations and echo free space posterior to NCSOV (Figure 1A) with a normal ejection fraction. A computed tomography (CT) aortogram confirmed the diagnosis of an unruptured pseudoaneurysm of NCSOV (Figure 1B).
Through a median sternotomy standard cardiopulmonary bypass was established. At moderate hypothermia diastolic arrest of the heart was achieved after aortic cross clamping with cold blood cardioplegia. The defect was accessed via oblique aortotomy. The opening in the NCSOV was seen extending from the aortic annulus to the sinotubular junction.The Aortic valve was tricuspid, severely stenotic with thickened leaflets and healed vegetations. The aortic valve and infected tissues were excised. The margins of the mouth of the aneurysm were cleaned, trimmed and repaired with a prosthetic patch using polypropylene sutures (Figure 1C). Aortic valve was replaced with a mechanical aortic valve prosthesis (ST. JUDE MEDICAL Inc., Minnesota, USA). Postoperative recovery was uneventful. One year postoperatively, the patient is doing well clinically with normal CT aortogram (Figure 1D) and has good mechanical valve function.
Acquired pseudoaneurysm of the sinus of Valsalva involves the right coronary sinus (80%), followed by the noncoronary sinus (16%), and the left coronary sinus (4%) [1]. These pseudoaneurysms are mostly associated with aortic regurgitation (AR) either due to primary cuspal involvement or secondary to annular dilatation. A literature search was carried out for pseudoaneurysm secondary to infective endocarditis (Table 1).

Our case is the only case to be reported in association with aortic stenosis (AS). A high degree of suspicion should be harboured when dealing with cases of aortic stenosis with infective endocarditis. Paravalvular abscesses and pseudoaneurysms involving the sinus of Valsalva rupture occur in 1.6% of cases, to form aortocavitary fistulae with the adjacent cardiac chamber (atrium or ventricle) or intrapericardially which can be fatal [2]. Aneurysms from the noncoronary sinus usually originate from its anterior portion and project into the right atrium, whereas aneurysms arising from the posterior portion of the noncoronary sinus may rupture into the pericardium [3]. These sequelae can occur subacutely, even after completion of intravenous antibiotic therapy as seen in our case. It is important that these sequelae are diagnosed early and treated urgently.
We postulate that the venturi effect of the blood column being ejected at high velocity strikes the aortic wall with enough force to slowly erode the aortic wall. Also with the onset of an infection on the aortic valve, the infective debris could flow with the blood column, seed the damaged tissue and establish a colony on the damaged aortic wall. This colony can enlarge and eventually lead to penetration and rupture of the aortic media and endothelium forming a pseudoaneurysm. Pericardial rupture of these pseudoaneurysms are almost always unsalvageable as they present in very pre-terminal stage. Although transthoracic, transesophageal echocardiography and color flow Doppler mapping are basic non-invasive tests for evaluation, perivalvular pseudoaneurysms can sometimes be challenging to define due to limited soft tissue resolution, thus necessitating a CT aortogram or a cardiac MRI [4-6]. Follow-up evaluations are mandatory for the early detection and treatment in such patients. The pre-operative diagnosis of an infected pseudoaneurysm has important therapeutic implications. Surgical correction can vary from aortic sinus repair to a more extensive intervention like aortic root replacement [4-8]. Our case was successfully managed by thorough debridement excluding the pseudoaneurysm with a prosthetic patch and aortic valve replacement (AVR) with bileaflet mechanical valve prosthesis for aortic stenosis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
