
case report | DOI: https://doi.org/10.31579/2641-0427/020
1Department of Orthopaedic and Trauma Surgery, Tergooi Hospital, the Netherlands
2Department of Radiology, Tergooi Hospital, the Netherlands
3Department of General Surgery, Tergooi Hospital, the Netherlands
*Corresponding Author: Simran Grewal, Lars den Ouden , Department of Orthopaedic and Trauma Surgery, Tergooi Hospital, the Netherlands,
Citation: Simran Grewal, Lars den Ouden, Alexander E. Scholtens, Jan P. Eerenberg, Ronald A.W. Verhagen. (2019). Surgical repair of an osseous avulsion of the adductor sleeve complex of the groin: a case report. J. Orthopaedics and Surgical Sports Medicine. 2(1); DOI:10.31579/2641-0427/020
Copyright: © 2019 Simran Grewal, Lars den Ouden. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 September 2019 | Accepted: 02 October 2019 | Published: 09 October 2019
Keywords: athletes; muscle injuries; MRI; anaesthesia; thromboprophylaxis;
Sports-related groin injuries are common among athletes. Avulsion of the tendons attached to the symphysis pubis has previously been described. These can be managed both operatively and non-operatively. To our knowledge a complete osseous avulsion of the adductor sleeve has not been described previously.
We report a case of a 56-year-old healthy man who sustained an acute osseous avulsion of the adductor sleeve complex on the left side, which was surgically repaired with bone anchors and a mesh. Return to normal activity was reached 8 weeks after immobilization and full return to play for all sports activities in 12 weeks.
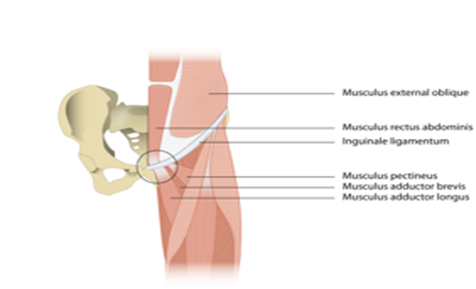
o our knowledge, no literature has been published on a complete osseous avulsion of the adductor sleeve which consists of the adductor longus, rectus abdominis and pectineus muscle. The adductor longus originates at the anterior surface of the os pubis, just lateral to the symphysis. Its insertion is at the middle third of the linea aspera. The rectus abdominis muscle is attached to the periosteum of the superior pubic ramus and is covered by the rectus sheath. The sheath is continuous with the tendon and is attached to the pubis anteriorly. The pectineus muscle lies immediately lateral to rectus abdominis on the superior pubic ramus and inserts at the pectineal line of the femur (Figure 1).
We present a case of a 56-year-old male, who incurred a traumatic osseous avulsion of his adductor sleeve complex. The operative procedure consisted of an anatomical re-attachment of the avulsed tissues and bone in combination with a mesh reinforcement of the posterior inguinal wall.
A 56-year-old healthy male sustained an injury to his left groin while he climbed over a fence next to the ice-skating rink. His left leg was forcefully abducted, extended and externally rotated. He complained of an acute pain in his left groin which was associated with a “snapping sensation”. Furthermore, he experienced immediate weakness in his leg. On clinical examination he had an antalgic gait and therefore walked with crutches. A hematoma was seen in the left groin and scrotum, with tenderness to palpation and pain on resisted adduction and resisted hip flexion.
Three days after injury, plain radiographs and magnetic resonance imaging (MRI) of the left hip were obtained to evaluate his injury. They revealed a complete osseous avulsion of his adductor sleeve complex (Figure 2).

A surgical repair of the avulsion and weak abdominal wall was performed as described in the surgical technique below.
Surgical Technique
The patient was placed supine on the operating room table. The procedure was performed under general anaesthesia.
An inguinal skin incision was made on the left side and the aponeurosis of the external oblique muscle was divided in the line of its fibres. Opening the superficial inguinal ring enabled identification of the spermatic cord and facilitated exposure of the adductor complex. At this level there was discontinuity of the adductor sleeve and the osseous fragment was found retracted from the symphysis origin and was positioned more superficially. The pubis was prepared for re-attachment of the stump by clearing the remains of the torn adductor tendon and debriding the proposed site of re-attachment.
A tension-free re-attachment of the adductor sleeve to the symphysis pubis was carried out
using 2 bone suture anchors (Fastin RC Mitek - DePuy Synthes - Amersfoort) for the fixation of the osseous fragment containing the adductor longus muscle and rectus abdominis muscle and two for the re-attachment of the pectineus muscle.
Because of weakness of the deep aspect of the anterior abdominal wall, a non-absorbable marlex mesh (ProGrip Polyester Mesh – Covidien – Eindhoven) was used to reinforce the repair in order to prevent a secondary hernia. After closing the inguinal canal, the subcutaneous tissues and skin were closed in layers using absorbable sutures. A pressure dressing was then applied. Postoperatively the patient was immobilized in a brace with 30 degrees flexion in the hip joint and 0 degrees abduction for 6 weeks. Low molecular weight heparin (LMWH) was given as thromboprophylaxis.
Follow Up
The brace was removed after 6 weeks and full weightbearing was allowed. Gradual full flexion and staged increase in abduction was started and strengthening exercises began. The patient returned to full activity without pain in 8 weeks. Physical examination revealed no tenderness over the adductor muscle group, and range of motion was equal to the contra lateral hip in flexion, extension, abduction, adduction, and rotation. Manual muscle strength testing was 5/5 with resisted adduction and identical to the contralateral hip. At 3 months postoperative he gradually returned to his previous level of sport activities with no residual symptoms.
Sport related groin injuries are common among athletes. Avulsion of the tendons attached to the symphysis pubis has previously been described. These can be managed both operatively and non-operatively. Much controversy remains regarding the optimal management of proximal adductor avulsion injuries, with some arguing for surgical fixation and others recommending conservative treatment [3-7].
Adductor tenotomy has been advised for chronic groin injuries [8]. Conservative treatment can be the choice of treatment in acute avulsions, however this may lead to chronic groin pain and decreased strength and function [5]. A surgical reattachment allows the muscle to function at its natural working length and reduces pain, but it also has the risks associated with surgical interventions.
This case report seems to be the first to describe an osseous avulsion of the adductor sleeve complex. The decision to treat this injury with acute repair was based on the character of the lesion. It was a complete osseous avulsion with an intact sleeve. A nonoperative treatment in the presented case may have led to a persistent defect with weakness of the adductors. The surgical procedure of using bone suture anchors in combination with reinforcement of the posterior wall by using a mesh was successful. Our patient returned to full activity without pain in 3 months.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
