
Research Article | DOI: https://doi.org/10.31579/2690-4861/130
1 Clinique de l’Archette, 83 rue Jacques Monod - 45160 Olivet, France.
2 Clinique du parc Drevon, 18 cours général de Gaulle - 21000 Dijon, France.
3 Pôle Rachis Doscea, 1 allée du Dr Robert Lafon - 64100 Bayonne, France.
4 Cheltenham Spine Clinic, United Kingdom.
5 Quanta Medical Group, 16 avenue des Chateaupieds – 92500 Rueil-Malmaison, France.
6 Cousin Biotech, Allée des Roses - 59117 Wervicq-Sud, France.
7 Clinique d’Argonay, RGDS, 685 route de Menthonnex- 74370 Argonay, France.
*Corresponding Author: Doan Co-Minh, Clinique de l’Archette, 83 rues Jacques Monod- 45160 Olivet France
Citation: D. Co- Minh, C. Vajeu, L Montron, C. E. W. Aylott, R. Boulkedid. (2021) Surgical outcomes of patients with degenerative lumbar disc disease post-IntraSPINE® device fixation: Three-year prospective study. International Journal of Clinical Case Reports and Reviews. 8(1); DOI: 10.31579/2690-4861/130
Copyright: © 2021 Doan Co-Minh, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 April 2021 | Accepted: 01 June 2021 | Published: 30 July 2021
Keywords: spine surgery; IntraSPINE®; interlaminar device; degenerative lumbar disc disease; low back pain
Background: Lumbar degenerative disc disease is one of the most common conditions associated with chronic low back pain. IntraSPINE® is a novel inter-laminar device that allows more physiological rocking-type movements in flexion and extension.
Aim: To evaluate the results of patients with symptomatic Lumbar degenerative disc disease treated with an IntraSPINE® device and followed up over a 3-year period.
Materials and Methods: A Prospective longitudinal research study involving patients with imaging-confirmed Lumbar degenerative disc disease in whom conservative treatment was unsuccessful. Outcome measures were changes over baseline score on the Oswestry Disability Index (ODI), and low back and radicular pain assessed at 6, 12, 24 and 36 months postoperatively. Overall success, a composite outcome that included key safety and clinical considerations, was assessed. Secondary outcomes included satisfaction with symptoms, employment status and post-surgery medical interventions. To compare differences in longitudinal clinical score patterns over 36 months, a mixed-effect model ANCOVA with repeated measurements was performed, with adjustment for low back and radicular pain score and ODI score at baseline.
Results: 231 patients were recruited and 180 completed the study. A significant improvement in ODI score (p=0.0597), as well as in VAS (Visual Analogue Scale) scores for back (p= 0.0228) and leg pain (p<0.0001) was observed during the follow-up. For ODI score, the mean percentage decrease from inclusion to month 36 was 64.5%. These scores were respectively 66.2% for radicular pain and 46.4% for low back pain. In 73% of cases, surgery was considered successful. 89% of working patients returned to work and 68% of patients were very satisfied at month 12. Only four patients presented intraoperative complications.
A variety of diseases can cause low back pain (LBP), one of which is degenerative lumbar disc disease (DDD) [1]. When conservative treatment fails, surgery may be considered. Although the rationale for surgery is often unclear, and despite the lack of convincing evidence regarding the effectiveness of surgery in the treatment of symptomatic DDD, the number of surgical procedures performed is continually increasing [2,3]. Yet the presence of LBP and DDD can support the placement of an interspinous device (ISD) [4–8].
The reported indications for ISDs are diverse and include degenerative spinal stenosis, discogenic LBP, facet syndrome, disc herniation and instability [9, 10].
IntraSPINE® is a novel device that, unlike interspinous positioned implants, is unique in being placed more anteriorly in an interlaminar position, closer to the normal center of rotation of the motion segment [11, 12]. Mechanical advantages are thus conferred over more posteriorly positioned devices through the possibility of more physiological ‘rocking’ type movements in flexion and extension [13,14]. This enables IntraSPINE® to off-load the facet joints in extension without blocking movement. Having a more anteriorly placed fulcrum also helps control excessive flexion movements by virtue of an improved lever arm in conjunction with an intact posterior tension band [15] .
The aim of this three-year prospective study is to report the results of patients with symptomatic DDD who were treated using an IntraSPINE® device. After a follow-up period of 36 months, we evaluated the clinical and safety results of the IntraSPINE® device in the treatment of DDD patients.
A prospective study was performed throughout the period from November 21, 2012 to December 20, 2017. It was conducted at 4 French clinics specializing in spinal surgery and involved one surgeon at each clinic. Patients were recruited from November 21, 2012 to December 1, 2014.
Patients with symptomatic LBP and / or radicular pain, with imaging confirmed DDD at one or two levels in whom conservative treatment was unsuccessful, and who had undergone surgery using IntraSPINE® were included. Inclusion diagnoses were: lumbar disc herniation (LDH), foraminal stenosis and facet joint syndrome. Non-inclusion criteria were: aged < 18>
Eligible patients with a diagnosis of DDD were informed about the study and, after providing written consent, each patient was enrolled. Patients were evaluated at 6, 12, 24 and 36 months postoperatively and all underwent a postoperative MRI.
Investigational Device:
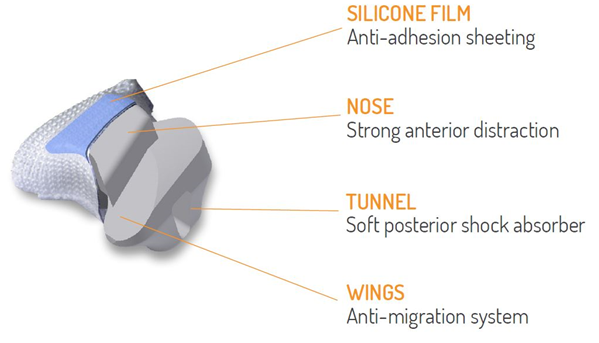
The IntraSPINE® is a dynamic interlaminar device made of medical dimethyl siloxane and covered with pure polyethylene terephthalate. The front surface is coated with a silicone film to prevent the formation of adhesions in the region of the yellow ligament or dura mater [16,17] (Figure 1). The device is available in five sizes (8, 10, 12, 14 and 16 mm) for optimal accommodation of the interlaminar space. IntraSPINE® is CE marked (March 2007) and made of materials allowing it a permanent duration of use or contact with the body.
The implant is compressed within the interlaminar space resulting in an immediate stable interference-type fit. Soft tissue in- and on-growth further secures the implant over time.
Surgical Technique:
All the participating clinics performed comparable routine spine surgical procedures as described on the manufacturer’s guidelines. All operations were performed under general anesthesia in the prone position with appropriate positioning precautions and hips and knees flexed.
Implanting IntraSPINE® is performed according to the following technique: incision of the interspinous ligament, trying to preserve the supraspinatus ligament. The distractor provided is used to improve access to the interlaminar space. Metal trials that are also available in 5 sizes are used to accurately size the interlaminar space.
The selected implant is briefly immersed in saline and then compressed with a simple holder which narrows the cranio-caudal dimension of the implant to facilitate simple lateral insertion.
Data collection
All data were collected using Quanta view eCRF and the Evamed database. Baseline evaluations, including basic demographic data and employment status, were conducted before surgery. Disc degeneration was assessed using the Pfirrmann grading system.
Furthermore, surgical data were collected. Variables of interest including discharge disposition, length of stay and post-surgical complication were also obtained from patient’s charts and physician’s notes.
Assessments of disability status and pain
Disability functional assessment was measured using the Oswestry disability index (ODI)[18], both preoperatively and at 6, 12, 24 and 36 months of postoperative follow-up.
Low back and radicular pain were also assessed on a visual analogue scale (VAS)[19] at each visit on a horizontal 100-mm scale ranging from 0 mm, “no pain”, to 100 mm, “the worst pain imaginable”. Patients were not shown the records of their earlier assessments.
Success was achieved if postoperative improvement at month 36 in terms of ODI score was at least 30%, and in the absence of complications, including revision surgery (reoperation) at the treated level, removal of the implant, infection or re-herniation or any other adverse event related to surgery or the device.
Post-surgery and satisfaction data
Secondary measures included patient work status and return-to-work data. Other medical interventions, including medication use and physical therapy were collected. The Likert scale was used to assess the grade of satisfaction with current symptoms and with care (1: Not satisfied at all, 4: Very satisfied).
Complications
A systematic assessment of complications including infection, hematoma, deep venous thrombosis, vascular injury, was carried out. Moreover, surgeons were asked to record intraoperative complications such as cerebrospinal fluid leakage. Throughout the entire course of the study, information was also collected on Adverse Events (AEs) and Serious Adverse Events (SAEs) occurring at any time point. Recurrent lumbar disc herniation (at the operated level) was also taken into account. Recurrent herniation was confirmed using MRI and classified as either symptomatic re-herniation (painful and requiring surgery) or non-symptomatic re-herniation (confirmed by MRI but not requiring reintervention).
Statistical analysis
Data analyses were performed using SAS Version 9.4 (SAS Institute, Cary, NC USA software). Data are presented as median and interquartile ranges (25th-75th percentiles) for continuous variables and number (percentage) for categorical variables.
To compare differences in longitudinal clinical score patterns over 36 months, a mixed-effect model ANCOVA with repeated measurements was performed, with adjustment for low back and radicular pain score and ODI score at baseline.
Safety data were described over the study period (number, seriousness, outcomes, and causal relationship with IntraSPINE® implant). Two-sided tests with type I error α = 0.05 were applied to all analyses.
A total of 231 patients were included in the study. Of these, 180 (78%) completed the study with an average follow-up of 2.7 years (Figure 2: Study flow chart).

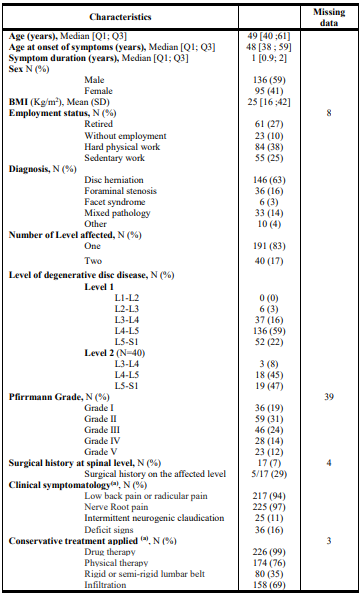
Baseline characteristics of the 231 included patients are shown in Table 1. Median age was 49 years (Q1; Q3: 40; 61). The majority of patient being male (58.9%) and employed (62 %). A median work stoppage of 30 days (Q1; Q3: 30; 90) was prescribed for 71/139 (51 %) employed patients. Disc herniation was the most common reported diagnosis (63%).
About 83% of the patients had degenerative disc disease at a single level, with L4/5 being most commonly affected (59%).
Among patients, 59 (31%) were classified as Pfirrmann Grade II. Drug therapy before surgery was prescribed for 99 % of patients and 76 % had physical therapy.
We report a national multicenter observational prospective study on the effects of a novel interlaminar device, “IntraSPINE®”, in a cohort of patients presenting DDD.
Our study found that complications related to surgery or to the device were very few, with only four patients presenting intraoperative complications (spinal fluid leak) which were unrelated to specific use of IntraSPINE®. This is consistent with the results of Leeet al who reported no complications such as myocardial infarction, pulmonary embolism, cerebrovascular accident, acute renal failure, mortality, deep venous thrombosis, ileus or urinary tract infection[20].
It is widely accepted that lumbar degenerative disc disease (DDD), as characterized by disc dehydration and loss of disc height, is one of the most common conditions associated with and predisposing to chronic low back pain [21,22].
Among options in treating symptomatic DDD, the inter-spinous devices ISD may be used to try and restrict painful motion.Inter-spinous space distraction may contribute to indirect decompression of the neural foramen and spinal canal but at the expense of lordosis. Theoretically, this enlarges the neural foramen in patients with spinal stenosis and neurogenic claudication [23]. However, inducing segmental kyphosis with any form of instrumentation would generally be considered a disadvantage and to be avoided. Also, a posteriorly placed interspinous implant is at a mechanical disadvantage in controlling abnormal flexion movement and is therefore less likely to be effective in ‘protecting’ the disc and reducing discogenic back pain.
The limitations of ISDs led to the development of the interlaminar device IntraSPINE® with its unique anterior positioning in the inter-laminar space [24] . IntraSPINE® provides both a fulcrum and support through the middle column of the spine, thereby contributing to the spine’s passive subsystem of stability. This unique positioning closer to the instant axis of rotation and nearer the sagittal axis of the facet joints allows the implant to more effectively off-load the facet joints in extension[13,20–26].
Also, an intact posterior tension band enables control of abnormal or excessive flexion movement, thereby ‘protecting’ the degenerate disc. In this way, IntraSPINE® has the potential to mitigate both facet and discogenic pain [24,27].
In this study, IntraSPINE® showed very good results, with an improvement in ODI score and in VAS back and leg pain scores during follow-up. The reduction in pain appeared to persist for two years, although scores increase slightly from 24 to 36 months, but nevertheless remained lower than baseline values. These results were also observed in the systematic review by Parker et al. in which the short-term and long-term incidence of recurrent back pain after primary single-level lumbar discectomy ranged from 3% to 34% and 5% to 36%, respectively[28] .
These results appear consistent with those in studies about ISD. Buric et al. showed that the outcomes after surgery using DIAM device were best between 6 and 24 months postoperatively followed by an increase in VAS scores from 24 to 48 months [29] . Despite this increase, VAS scores remained significantly lower than the baseline values. Considering these results, ILD could very well be proposed as an alternative to ISD.
The efficacy of this interlaminar device, in addition to standard microdiscectomy, in preventing recurrence of LBP has already been published[15]. The rationale for using this interlaminar device in conjunction with discectomy to reduce the incidence of post-discectomy back pain is the ability of the prosthesis to slow down disk-space collapse and control abnormal patterns of movement or micro-instability [30].
Our results show that 89% of active patients returned to work after surgery within an average of 3 months. Moreover, day case surgery was achieved in almost 3% of cases. Healthcare costs for LBP are increasing rapidly[31]. Direct and indirect costs of LBP associated with loss of earnings or changes in productivity are very high [32,33]. Hence, it is essential to develop treatments that are both clinically effective and, no less importantly, cost effective.
In this study, 16/146 (11%) of patients with disc herniation experienced symptomatic postoperative disc re-herniation. This result is consistent with the literature, which reports re-herniation rates of between 5 and 18% [34–36]. Regarding this aspect, since the IntraSPINE® maintains close to normal movement of the affected segment, it behaves just like a “normal” segment and thus with the same probability of recurrences. Although in theory IntraSPINE® has the potential to reduce disc re-herniation by abolishing excessive flexion movement and protecting the disc [37], a study in a significantly larger patient population is needed to achieve the requisite statistical power to provide proof. In addition, some experts are of the opinion that re-herniation occurred due to the relatively small size of the implants (8 mm), but this hypothesis remains to be confirmed too.
Regarding the further surgery, IntraSPINE® did not manage to rule out this factor. According to the experience of the surgeons who took part in the study, in the rare event that removal of the IntraSPINE® is necessary to gain access to the spinal canal, the device is easily removed without damaging the surrounding soft tissues, bone or dura mater. This is because IntraSPINE® is coated with a film of non-adherent silicone on the surface in contact with the dura mater or yellow ligament, effectively preventing the formation of adhesions to these layers.
The material composition of IntraSPINE®, comprising a silicone core and an outer shell reinforced by continuous wound PET fiber, is similar to ISP devices such as DIAM[29] or synthetic intervertebral disc prostheses [38]. According to the authors of the latter report, the combination of these materials represents a composite that mimics the architecture of the intervertebral disc and presents similar viscoelastic properties, making the device able to support/replace the function of the disc itself [38].
One limitation of our study was possible bias related to the fact that this was an observational study. The absence of a control group receiving standard care (surgery) without device insertion prevented us from confirming that the improvement in patient outcome post-operatively is related to the IntraSPINE® device alone. However, our results are consistent with the comparative study of Corriero et al. showing the absence of low back pain during the follow-up period in 74% of patients who received the IntraSPINE® implant, compared with only 41% of patients treated by simple stand-alone microdiscectomy who remained pain-free [15]. Moreover, numerous randomized studies assessing the efficacy of ISD found a significantly greater improvement in ODI score, as well as VAS back and leg pain scores, among patients with an ISD compared with those treated with stand-alone surgery[39,40]. These results suggest that the use of an implant may confer additional benefits over un-instrumented surgery in terms of patient outcome. Although some studies reports that Interspinous process decompression is still considered investigational and poor clinical results in the medical literature will continue to limit the appeal of these devices to many surgeons in the future [41]
Another limitation was that some patients would be inevitable lost to follow-up since this was a study with multiple follow-up appointments over three years, it. This potentially introduces a bias in the final analysis that could lead to under- or over-estimation of the outcomes following surgery. However, despite a long follow-up period, 78% of patients completed the study, which is relatively acceptable and reduces this potential bias [42].
Another limitation consists in the absence of radiological data. It would have been interesting to measure post-operative lordosis using standing X-rays to assess sagittal balance and segmental alignment following IntraSPINE® insertion. Previous radiological studies of IntraSPINE® devices suggest that the implant does not affect sagittal balance [24,43] and that it also maintains the biomechanics of the spine in an effective manner with slowing down or partial reversal of the natural progression of the degenerative cascade[26]. Radiological enlargement of the neural foramen has also been reported previously [23,24].
Supporting this, in vitro studies have shown that ISDs distract the posterior part of the functional spinal unit, reposition and unload the facet joints, and reduce intervertebral pressure, particularly on the posterior part of the disc [44].
In summary, the findings of this study are promising and demonstrate that successful patient outcomes can be achieved using the IntraSPINE® device for a range of degenerative diseases, with improvements in both back/leg pain and disability, sustained at 3 years. Implantation of the IntraSPINE® device was straightforward and there were no device-specific complications. Use of the IntraSPINE® in the treatment of degenerative disease of the lumbar spine has been evaluated and discussed in published papers.
The findings of this study coupled with other published research results suggest that IntraSPINE® may confer additional benefits in terms of back pain reduction and disability outcomes when used in conjunction with decompression or microdiscectomy in comparison to stand-alone decompressive procedures. A helpful future trial would single-blindly randomize the implantation of IntraSPINE® to patients undergoing a decompressive procedure so as to produce a matched control group. In addition, economic evaluation will be conducted in future trials to assess the cost effectiveness of using IntraSPINE®. The results of such follow-up trials are expected to establish a robust clinical basis for the effects of IntraSPINE® in this patient population.
This study was funded by Cousin Biotech. The funder had no role in the interpretation or reporting of results. One of the Author (FH) is employee of Cousin Biotech Company involved in the manufacture of a device examined in this study.
This study received a favorable opinion from ethical committee of Clinique d’Argonay.
D.C, C.V, L.M and M.L performed patient’s recruitment and data collection. N.W performed data monitoring. R.B, H.R, and O.Z. analysed the data. All authors discussed the results and commented on the manuscript. R.B wrote the paper with input from all authors. C.A worked on the manuscript and correct it.
We are grateful for the contribution of Dr. José Manuel Cabezudo, Prof. Giancarlo Guizzardi and Prof. Gualtiero Innocenzi for their proofreading and commentary on this manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
