
case report | DOI: https://doi.org/10.31579/2692-9562/086
1 Junior Resident Dept. of ENT and Head Neck Surgery Dr. Vasantrao Pawar Medical College & Research Centre, Adagaon, Nashik.
2 Associate Professor Dept. of ENT and Head Neck Surgery Dr. Vasantrao Pawar Medical College & Research Centre, Adagaon, Nashik.
3 Professor Dept. of ENT and Head Neck Surgery Dr. Vasantrao Pawar Medical College & Research Centre, Adagaon, Nashik.
4 Associate Professor Dept. of ENT and Head Neck Surgery Dr. Vasantrao Pawar Medical College & Research Centre, Adagaon, Nashik.
*Corresponding Author: Shashikant Anil Pol
Citation: Nirmala Yamgar, Shashikant Anil Pol, Shreeya Kulkarni, Rushika Patel, (2023), Surgical Management of Unusual Nasal Masses: A Case Series, J Clinical Otorhinolaryngology, 5(4); DOI:10.31579/2692-9562/086
Copyright: © 2023, Shashikant Anil Pol. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 09 March 2023 | Accepted: 22 May 2023 | Published: 09 June 2023
Keywords: nasal; orbital; otorhinolaryngologist; pathologies; paranasal sinus; histopathological; surgical
Aim: To evaluate the clinical presentation, histopathology, and surgical management of various nasal masses.
Background: Nasal masses cause symptoms ranging from minor nasal obstruction to orbital problems.
Case Presentations: A 66 yrs male with epistaxis from the left nostril. Imaging was suggestive of a neoplastic lesion. Endoscopic Excision was done which came as capillary haemangioma. An 11yrs female came with nasal blockage and eye proptosis. Imaging was suggestive of a neoplastic lesion. Biopsy showed alveolar rhabdomyosarcoma which was managed by a combined approach. An 83yrs female came with a right eye diminished vision, and proptosis. Imaging revealed a right-sided frontal sinus mucocele extending to the right orbit. Endoscopic marsupialization resulted in drastic improvement in vision. A 66yrs male with sudden diminution of vision of the left eye. Imaging revealed a lesion in the sphenoid sinus abutting the optic nerve. The lesion was removed with left optic nerve decompression. Histopathology was suggestive of tuberculosis. Significant improvement in vision was noted postoperatively. An 18yrs male with right nasal blockage and intermittent bleeding. Imaging suggestive of juvenile angiofibroma. Endoscopic removal was done. Histopathology came as nasal angiofibroma.
Discussion: Nasal endoscopy, radiological assessment, surgical intervention, and histopathological evaluation were performed on five patients which helped in making a specific diagnosis, preventing the possibility of missing unusual cases.
Conclusion: Endoscopic Surgery is the main treatment modality for various nasal masses nowadays because of advantages like scarless surgery, excellent exposure, less bleeding, low morbidity, and early recovery.
Clinical Significance: Imaging helps with pre-surgical planning and histology enables us to make accurate diagnoses.
The presence of any mass in the nose and paranasal sinuses may seem to be a straightforward issue, but it raises a lot of questions about the differential diagnosis. The majority of patients present with complaints of nasal blockage, nasal discharge, sneezing, smell disturbances, epistaxis, and ocular issues such as epiphora, proptosis, diplopia, and visual problems.1 Various differential diagnoses can be made for a sinonasal mass which could be traumatic, congenital, neoplastic, or inflammatory.2 They are primarily classified as nonneoplastic and neoplastic and further in benign and malignant among the neoplastic lesions.1 The basic course of treatment for such nasal mass is surgical excision, but because these tumors may be close to important structures such as the brain or orbit, managing the recurrent or residual disease is challenging. Hence a multidisciplinary approach using radiation and surgery is required for locoregional treatment.3 In this paper, we discuss 5 such unusual cases that we encountered in the last 6 months in tertiary care hospital including capillary hemangioma, rhabdomyosarcoma, frontal mucopyocele, and juvenile nasal angiofibroma which were managed successfully mainly with surgery and in one it was managed by combined modality treatment including ChemoRadiation followed by salvage surgery. All patients were doing fine till six months of follow-up.
Case 1:
A 64 year old male presented with bleeding from the left nostril which was associated with left-sided nasal obstruction. He was hypertensive and on regular medication. There were no complaints of nasal discharge, anosmia, or facial swelling. We did zero degree nasal endoscopy which reveals Vascular Mass which was seen attached to the posteroinferior part of the inferior turbinate and the posterior part of the nasal septum (Figure. 1a). Computed Tomography Scan of Paranasal Sinuses (plain+contrast) showed an ill-defined hypodense soft tissue density lesion measuring approximately 3.2x1.6x2.3cm in the left nasal cavity, extending posteriorly up to choana. In post-contrast study, the lesion is showing mild to moderate heterogeneous enhancement (Figure. 1b). Findings were likely suggestive of the neoplastic lesion. After getting fitness for general anesthesia and written and informed consent from the patient and attendant we did a Transnasal Endoscopic excision of the nasal mass after cauterizing the attachments between the turbinate and septum and the specimen was sent for histopathology (Figure.1c). We did a spurectomy for complete exposure of the mass. On histopathology, it showed stroma with lobular, few dilated, and thick-walled blood vessels likely suggestive of capillary haemangioma (Figure. 1d). Epistaxis was relieved immediately after mass removal. On regular follow-up, till six months there was no bleeding and the patient was doing fine with a healthy bilateral nasal cavity without any mass. In this case, as per the age and radiological findings we thought of neoplastic etiology but surprisingly on histopathology it came as capillary hemangioma which was very unusual at this age.
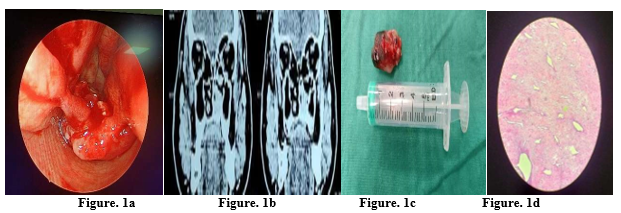
Figure. 1a: Nasal Endoscopy showing vascular mass between inferior turbinate and septum.
Figure. 1b: Contrast Enhanced Computed Tomography of Nose and PNS showing extent of lesion.
Figure. 1c: Nasal Mass after excision.
Figure. 1d: Histopathology showing Capillary Hemangioma.
Case 2:
A 10 years old female came with chief complaints of right-sided infra-orbital swelling with pain and tenderness with right nasal obstruction. She also had right-sided proptosis with severe ptosis (Figure. 2a). There were no complaints of nasal discharge, anosmia, or epistaxis. On a Computed Tomography scan of paranasal sinuses (plain+contrast), there was a large soft tissue density lesion approx. 3.4x1.7x3.3cm in the right maxillary sinus causing erosion and destruction of the medial wall, posterolateral wall, and part of the anterior wall of the right maxillary sinus. It is bulging posteriorly into masticater space, right pterygomaxillary fissure, and part of the pterygopalatine fossa. Medially the lesion is causing erosion of the right middle, inferior turbinate, right ethmoidal sinus plate, and part of the nasal septum. The lesion is causing erosion of the floor and medial wall of the right orbit and superomedial aspect with intraorbital extraconal extension seen in the right orbit indenting over the inferior rectus muscle (Figure. 2b). Findings were likely suggestive of the neoplastic lesion. We also did Magnetic Resonance Imaging (MRI) Ill-defined T1 hypointense and T2 hyperintense lesion approximately 3.4x1.7x3.3cm in the right maxillary sinus (Figure. 2c).
As Mass was completely occupying the right nasal cavity, the maxillary sinus was approached by Denker’s approach. Around 4-5ml cystic fluid aspirated from the maxillary sinus. A deeper biopsy was taken from the mass and sent for the frozen section which was suggestive of a round cell tumor probably rhabdomyosarcoma (Figure. 2d). Right orbital floor dehiscence note. After confirmation of Rhabdomyosarcoma, she underwent 4 cycles of chemotherapy. Histopathology showed cells with mildly pleomorphic, vesicular nuclei suggestive of a malignant round cell tumor probably alveolar rhabdomyosarcoma (Figure. 2g). Initially patient had given a good response to chemo and radiotherapy but after 4 cycles there was a relapse because the patient became a defaulter and not gone for chemo or radiotherapy. After a gap of about 3 weeks, the patient developed vision loss, and her globe became fixed so after getting fitness for general anaesthesia and written and informed consent we did right-sided salvage subtotal maxillectomy with orbital exenteration (Figure. 2e,f). Before taking the patient for surgery we did a repeat MRI which showed a tumor involving mainly orbit and maxillary sinus with the intracranial component in the frontal lobe. For the intracranial part, the patient underwent 23 cycles of radiotherapy and 6 cycles of chemotherapy. The patient was doing well till six months of follow-up without any relapse
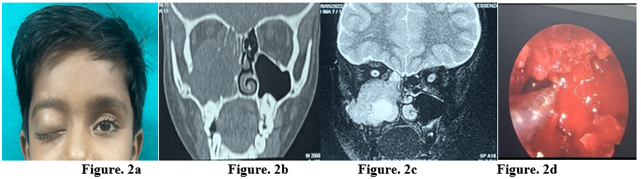
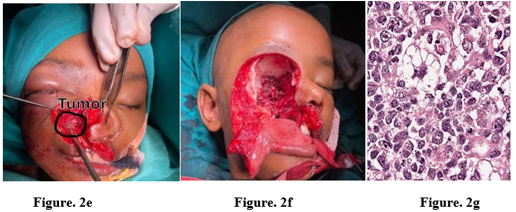
Figure. 2a: Clinical Picture showing ptosis and proptosis.
Figure. 2b: Non Contrast Computed Tomography of Nose and PNS showing extent of lesion.
Figure. 2c: Magnetic Resonance Imaging of Orbit and Brain showing extent of lesion.
Figure. 2d: Endoscopic biopsy from right maxillary sinus.
Figure. 2e: Salvage Subtotal Maxillectomy showing extent of tumor.
Figure. 2f: Intraop picture after maxillectomy and orbital exenteration.
Figure. 2g: Histopathology showing Alveolar Rhabdomyosarcoma.
Case 3:
An 83yrs old female came with chief complaints of right eye diminished vision, right eye proptosis, and swelling over the right side forehead with obvious cosmetic deformity since one year (Figure. 3a). There were no complaints of nasal obstruction, diplopia, reduced extraocular movements, headache, ocular pain, redness, discharge, or facial pain. Non-Contrast Computed Tomography (NCCT) of the Nose and Paranasal Sinuses showed an ill-defined homogenous soft tissue lesion arising from the right-sided frontal sinus showing scalloping of its anterior, posterior and medial walls with the expansion of the sinus cavity with the erosion of superior and inferior frontal sinus walls extending inferiorly to right ethmoidal air cells and right orbital cavity (Figure. 3b). It is causing inferomedial and anterior displacement of the globe abutting the right lateral rectus, superior rectus, and right optic nerve (2.0*2.2*1.5 cm in right orbit). No enhancing septae or calcification in it after contrast. Magnetic Resonance Imaging (MRI) of the Orbit and Brain showed ill-defined expansile T1 hyperintense and T2/FLAIR hyperintense soft tissue density with frontal sinus cavity expansion and erosions, extending extraconally to the right orbit (2.0*2.2*1.5cm) with the anteroinferior displacement of the right globe (Figure. 3c). We did Transnasal Endoscopic Marsupialization of the frontal sinus mucopyocele was done under General Anesthesia after getting written and informed consent from the patient and attendant. The mucopyocele was protruding between the right bulla ethmoidalis and the middle turbinate. Anterior ethmoidectomy was done and the frontal recess was cleared. After exposing the mucosa and eggshell bone, the surgical incision was made on the inferior margin of the mucopyocele, and 30 to 40 cc of pus was drained, along with exteriorizing and marsupialization (Figure. 3d). Saline irrigation was used to flush any leftover debris from the frontal sinus. There was a drastic improvement in right eye vision immediately from finger counting 2.5 meters to 6/12 with a complete reduction of the boggy swelling and proptosis (Figure. 3e). The patient was doing fine till six months of follow-up with patent and wide frontal sinus opening on endoscopy (Figure. 3f).
Figure. 3a: Clinical picture showing proptosis and cosmetic deformity.
Figure. 3b: Non Contrast Computed Tomography of Nose and PNS showing extent of lesion.
Figure. 3c: Magnetic Resonance Imaging showing extent of lesion intraorbitally.
Figure. 3d: Wide Frontal sinus opening after marsupialization.
Figure. 3e: Post op picture showing complete regression of proptosis and cosmetic deformity.
Figure. 3f: Follow up endoscopic view of patent frontal sinus.
Case 4:
We report a case of 66-year-old male presenting with the chief complaints of sudden diminution of vision in the left eye for 10 days. There was no history of nasal blockage, nasal discharge, any facial swelling or facial pain, or eye pain. Pre-operative vision assessment on the Right eye was 6/12 and for the Left eye, it was Finger counting at 3 meters. NCCT of the nose and paranasal sinuses showed an ill-defined soft tissue density in the sphenoid sinus, left optic canal abutting the superior rectus muscle, and left optic nerve with erosion seen in the superior wall of the left orbit (Figure. 4a). The patient was taken under general anesthesia for endoscopic removal of the mass after getting written and informed consent. Intraoperative observations in the sphenoid sinus, there was an unhealthy light pinkish-gritty mass, associated with bony erosion of the left orbit's superomedial wall till the level of the optic chiasma, a mass was observed compressing over the left optic nerve (Figure. 4b). The mass was completely removed, the left optic nerve was decompressed, and tissue was sent for histological analysis. Post-operative day 1 vision assessment showed significant improvement from figure counting to 6/24. The histopathological report showed ill-formed epithelioid cell granulomas with giant cells surrounded by a cuff of lymphocytes suggestive of granulomatous inflammation most common differential diagnosis being mycobacterium tuberculosis. The patient was followed after a week which showed left eye vision 6/9. It was consistent till the last follow-up of six months.
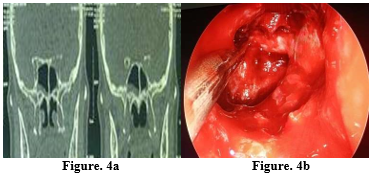
Figure. 4a: Non Contrast Computed Tomography of Nose and PNS showing extent of lesion with erosion of superolateral wall of sphenoid sinus along with compression of optic nerve.
Figure. 4b: Endoscopic view showing optic nerve decompression till chiasma.
Case 5:
An 18 years old male came with chief complaints of right nasal obstruction with right intermittent nasal bleeding since 5 months (Fig. 5a). There were no complaints of nasal discharge, anosmia, or altered sensorium. A computed tomography scan of paranasal sinuses (plain+contrast) revealed a large ill-defined soft tissue lesion noted in the nasopharynx with an epicenter at sphenopalatine foramina measuring approximately 9.3*5.0*4.7cm. It is extending laterally through the pterygomaxillary fissure, pterygopalatine fossa up to the infratemporal fossa. Widening of pterygomaxillary fissure and pterygopalatine fossa noted. The lesion is extending intracranially measuring 2.5x1.5cm. Findings were likely suggestive of juvenile angiofibroma stage 3-Andrews Fisch classification (Figure. 5b). Pre-operative embolization was done 48 hours prior to surgery. The right nasal cavity was completely occupied by mass (Figure. 5c). The maxillary sinus was approached by Denker’s approach and the mass separated from the maxillary sinus and brought medially. The posterior wall of the maxillary sinus was drilled and attachment from the infratemporal fossa was separated and brought medially (Figure. 5d). Attachment from the nasopharynx was separated and the mass was brought medially. Mass removed from the right nasal cavity. Haemostasis was achieved and the bilateral nasal cavity was packed with a merocele nasal pack. On histopathology, it showed blood vessels are lined single layer of endothelium. Stroma shows increased fibrosis and collagenisation suggestive of Angiofibroma (Fig. 5e). On the last follow-up six months the patient was fine without nasal bleeding and recurrence.
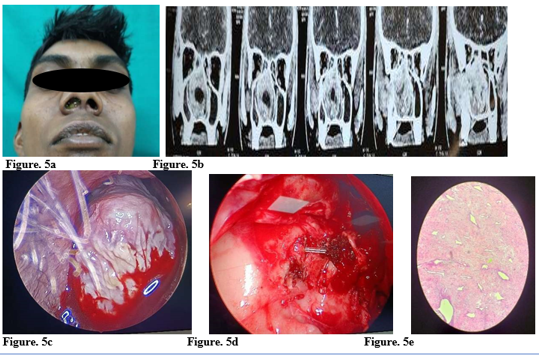
Figure. 5a: Clinical picture showing mass filling right nasal cavity with cheek swelling.
Figure. 5b: Non Contrast Computed Tomography of Nose and PNS showing extent of lesion.
Figure. 5c: Endoscopic view showing mass filled in nasal cavity.
Figure. 5d: Endoscopic view of mass after ligation of maxillary artery.
Figure. 5e: Histopathology showing Angiofibroma.
Sinonasal masses have various differential diagnoses. Malignancy should be distinguished from non-malignant lesions. Preoperative diagnosis based on proper clinical examination is consistent with histopathological diagnosis in most cases.1 Capillary hemangioma is the most common vascular tumor of the nasal cavity in the adult population.The development of the mucosal variant of capillary hemangioma most commonly occurs in the anterior nasal septum (Little's area), the inferior turbinate, and the vestibule. In our case, the capillary hemangioma developed in the posterior septum and posterior part of the inferior turbinate in 65yrs old patient.4 Rhabdomyosarcomas are rare soft tissue malignancies that occur mainly in the pediatric population. Treatment for rhabdomyosarcoma can include different combinations of surgery, chemotherapy, and radiation.5 We also treated a female pediatric patient with an alveolar variant of rhabdomyosarcoma by the combined modality of surgery and chemo/radiotherapy and the patient is doing well to date.5 Mucopyocele is a benign, mucosa-lined pseudocystic lesion of the paranasal sinus that, due to mucus secretion, has a tendency to expand giving rise to mass effect on surrounding structures. Endoscopic marsupialization is the modality of choice to achieve complete evacuation of the mucopyocele and reestablish the normal sinus outflow.6 Similarly in our case complete removal of mucopyocele by endoscopic marsupialization was done. Juvenile Nasopharyngeal Angiofibroma (JNA) is a benign, highly vascular tumor that is diagnosed on the basis of clinical and imaging features. It has a characteristic pattern of spread commonly involving the pterygopalatine fossa and pterygoid base. Endoscopic endonasal surgery is currently the treatment of choice for almost any size of tumor and is feasible even for advanced lesions.7 Similarly in our case we excised the whole tumor endoscopically which was extended intracranially.
Numerous pathologies are housed in the nasal and paranasal sinuses. In some unusual cases, histopathology and clinical diagnosis may not always coincide, which presents therapeutic challenges to otorhinolaryngologists. The interdisciplinary approach of the surgeon, a pathologist, and an oncologist should be used to provide the best possible outcomes for the patients
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
