
Case report | DOI: https://doi.org/10.31579/2578-8868/344
1Neurosurgeon Consultant, Neurosurgery Department, Policlínica Juaneda Miramar, Palma de Mallorca, Balearic Islands, Spain.
2Neurosurgeon Consultant, Neurosurgery Department, Policlínica Nuestra Señora del Rosario, Ibiza, Balearic Islands, Spain.
3Chairman of the Neurosurgery Department, Policlínica Juaneda Miramar, Palma de Mallorca, Balearic Islands, Spain.
4Chairman of the Neurosurgeon Department, Policlínica Nuestra Señora del Rosario, Ibiza, Balearic Islands, Spain.
*Corresponding Author: Gonçalo Januário, Neurosurgeon Consultant, Neurosurgery Department, Policlínica Juaneda Miramar, Palma de Mallorca and Neurosurgeon Consultant, Neurosurgery Department, Policlínica Nuestra señora del Rosario, Ibiza, Balearic Islands, Spain.
Citation: Gonçalo Januario, Pedro Llinas, (2024), Surgical management of intraventricular subependymoma, review the state of the art, J. Neuroscience and Neurological Surgery, 16(4); DOI:10.31579/2578-8868/344
Copyright: ©, 2024, Gonçalo Januário. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 25 October 2024 | Accepted: 13 November 2024 | Published: 06 December 2024
Keywords: subependymoma; glial tumors; lateral ventricle; microneurosurgery;, gross total resection; magnetic resonance
Ependymomas are glial tumors with ependymal differentiation. Represent the most common spinal cord primary tumor in adults and the third most common in pediatric population central nervous system. Although as a group they represent less than 10% of all neuroepithelial tumors.The age distribution is bimodal, first peak incidence around 5-6 years of age when infratentorial lesions predominate, a second peak in the 3th-4th decades, at which time spinal examples are most common.This group of neoplasms include subependymoma (World Health Organization [WHO] grade I), myxopapillary ependymoma (WHO grade I), ependymoma (WHO grade II), and anaplastic ependymoma (WHO grade III). The ependymoma, RELA fusion-positive, is a entity codified in the revised 4th edition of the WHO classification, present aggressive behavior and include the majority of supratentorial ependymomas.Supratentorial ependymal tumors, including ependymomas and subependymomas, more frequently arise in the lateral ventricles.We describe a clinical case of a 59 years old female that presented headache and memory disturb. The computerized tomography (CT) showed a lesion in left frontal lateral ventricle, without paraventricular extension. In magnetic resonance images (MRI) the lesion showed a isohypodensity with minimal enhancement, hypointensity on T1-weighted and hyperintensity on T2-weighted images. With a micro-craniotomy and transcortical approach was obtained a total resection of the tumor. The histological study present a diagnosis of subependymoma.The patient presented a good evolution without complication and no tumor recurrence during the follow up.
Intraventricular neuroepithelial tumors (IVT) are rare lesions that account for 2–7% of intracranial tumors and comprise different pathological entities such as ependymomas, subependymomas, central neurocytoma and glioependymal cysts.[1]
Most of the cases present benign lesions that arise from the ventricular wall or the choroid plexus.[2,3,4]
Subependymomas are rare, indolent neoplasms that are histologically classified as low grade World Health Organization (WHO) grade 1 and represents only 0.2–0.7% of all central nervous system tumours.[5,6,7,8]
This tumour, in adult population, occur in both sexes and all age groups but most frequently in the middle-aged to older individuals, typically in the fifth and sixth decade of life.[9]
The majority of cases are asymptomatic, sometimes the symptoms caused by hydrocephalus or spontaneous tumor hemorrhage may occur associated with larger tumors in the fourth, lateral and third ventricles, septum pellucidum and less commonly the spinal cord.[10]
Despite its benign nature can occur tumor recurrence and metastasis within the central nervous system following surgical resection.[11]
Compared to other intracranial tumors, there is a relative paucity of published series on subependymoma focusing on long-term post-operative outcomes. A better understanding of the long-term outcomes would not only benefit patients but also reduce health care costs.[12]
Actually the duration of follow-up required for these patients is not clear, but we recommend minimum 1 time per year during 5-10 years a clinical control and magnetic resonance images (MRI).
The surgical resection presents the treatment of choice, IVTs are regularly not targetable by radiation or systemic therapy.[13]
The aims of this study were to describe a clinical case of intracranial subependymoma treated by surgical resection and also review the literature.
A 59‐year‐old female, consulted because of 6 weeks of moderate headache, and episodic memory lapse, gait ataxia and dysarthria of several minutes’ duration. When observed presented highlighted a psychomotor slowdown affection.
In this context were made a magnetic resonance imaging (MRI), which showed a lesion located in the left lateral ventricle isointense to gray matter on T1-weighted images and hyperintense on T2-weighted images. The lesion caused expansion and scalloping of the left lateral ventricle because a partial obstruction in the foramen of Monro thus creating ipsilateral mild hydrocephalus. The third and fourth ventricles were of normal size. Also founded a bilateral atrophy of cerebral parenchyma (Figure 1, 2).
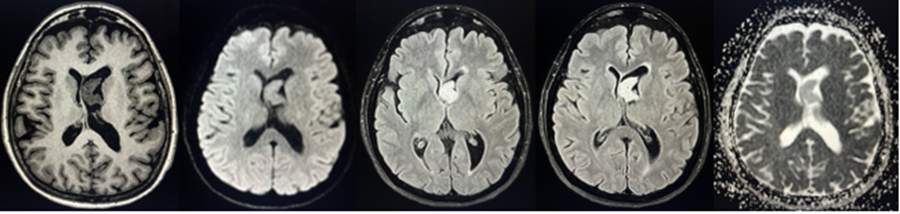
Figure 1: axial slices T1-weighted, FLAIR, DWI, present a lesion located in the left lateral ventricle.
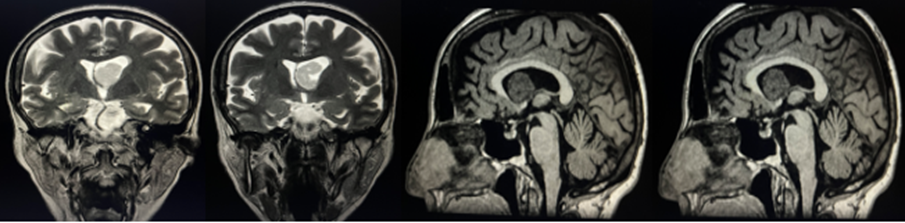
Figure 2: coronal T2-weighted and sagital T1-weighted slices, lesion located in the left lateral ventricle that cause partial obstruction in the foramen of Monro wit ipsilateral mild hydrocephalus
The patient was hospitalized in our department for further management. A few days after under general anesthesia and intraoperative monitoring we did a left parietal craniotomy and a gross total resection of the lesion was achieved, and there were no postoperatorative complications.
Histological samples were interpreted as rounded nuclei and scarce cytoplasm, and cell groups surrounded by abundant fibrillary matrix and
cystic areas. Immunohistochemistry was positive for glial fibrillary acidic protein (GFAP) and negative for neurospecific enolase, which was compatible with grade I subependymoma, according to the World Health Organization (WHO) classification. The patient is currently asymptomatic of his neurosurgical condition, with complete resolution of his speech and gait ataxia disorders. Postoperative imaging shows no tumor recurrence a year after the surgery (Figure 3)
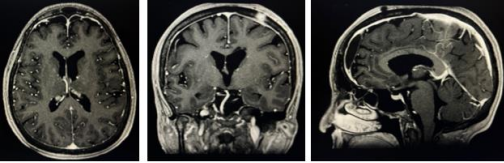
Figure 3: MRI T1-weighted with gadolinium contrast, axial, coronal and sagital slices, without tumor recurrence, no hydrocephalus or other complication.
Subependymoma is a rare, benign, slow-growing tumor that was described by Scheinker in 1945. This tumors arising from the subependymal cell plate and are commonly located in the fourth and lateral ventricles, also been reported in the third ventricle, septum pellucidum and spinal cord.[14,15]
Due to its rarity and variable imaging characteristics, reliable pre-operative diagnosis remains challenging.[16]
These tumors usually are asymptomatic and occurs more often in males. The symptoms present a directly correlation with tumor size and the majority of symptomatic subependymomas measuring 3–5 cm or greater in size. In these cases, the occurrence is also related with the tumor location particularly the supratentorial lesions more often symptomatic than fourth-ventricle tumors. The most frequent symptoms are headache, gait ataxia, vertigo or dizziness, nausea and vomiting.[17,18]
The clinical signs in small size tumors are caused for the obstruction of the cerebrospinal fluid (CSF) pathway.[19]
The natural history and the pathophysiology of subependymoma was less well understood and there has been a paradigm shift in the management of these tumors over the time.[20]
During the diagnosis process the clinical symptoms are important but not specifics for this pathology, actually the MRI its the gold standard for the diagnosis. Radiologically, subependymomas are typically well demarcated, non-enhancing, nodular lesions usually in the fourth ventricle. On pre-contrast MRI studies, they are generally hypo- or isointense to grey matter in T1 signal intensity and hyperintense on T2 modality.[21,22]
Presence of contrast enhancement is not typical for subependymoma, but rather is more frequently seen in cases of ependymoma. There were too few cases in our study to undertake any analysis of MRI features to predict the likelihood of complete resection or to develop post-operative hydrocephalus.
Actually the surgery is established as the treatment of choice for symptomatic subependymoma. Due to the technical evolution of all microneurosurgical techniques aided by neuronavigation ensure an efficient and safer approach for maximal tumor excision.[23]
With all the developments and methods have also led to a significant reduction in complication rates from 23.5–33% in the 1990s to 0–15% in more recent surgical series.[24,25]
Previous cohorts, described that hydrocephalus was the most common complication with rates between 7-23% following subependymoma resection with patients requiring treatment with ventriculoperitoneal shunt within 1 month or an endoscopic third ventriculostomy. The majority of cases still stable WHO performance status throughout follow-up and with low morbidity.[26]
During the last decades many different approaches was described to enter the lateral and/or third ventricle a variety including the frontal-transcortical, anterior/posterior interhemispheric-transcallosal and the contralateral interhemispheric-transfalcine-transprecuneal. [27,28,29,30,31,32]
The possibility to approach intraventricular tumors in patients without hydrocephalus does not alone preclude endoscopic management. In fact, the current results offer strong credence to the contention that patients traditionally considered poor candidates for a less invasive and potentially advantageous procedure should be offered an endoscopic alternative. The procedure in this clinical setting is effective in achieving the intended surgical goal and does not significantly differ from the results in patients with hydrocephalus.[33]
The approach depend like in all surgical treatments the center and surgical team experience, craniotomy and microdissection is an option, the lack of hydrocephalus in patients with intraventricular tumors does not exclude endoscopic management.[34]
The less invasive and potentially advantageous procedure should be offered an endoscopic alternative should be considered hypothetically in all the cases.[35]
Tumor location and extend of resection are the most important prognostic factors as recurrence has only been reported in case of subtotal resection.[36] Their growth rate tends to be slow. Rarely, aggressive tumors invading brain parenchyma or showing CSF dissemination are described as well.[37]
As radiation or systemic treatment do not apply for subependymomas, surgery remains the only viable option in this entity. The surgical strategy focusses on maximal but safe resection, resulting in permanent absence of the tumor. In the majority of reports, gross total resection could be achieved in >70% of patients, with low rates of mortality and morbidity.[38,39, 40]
The cases treated with stereotactic radiosurgery (SRS) has been successfully particularly for small diameter subependymoma with no tumor recurrence reported in a case following 54 months of follow-up. The SRS is a potentially important option for intracranial ependymoma patients. The overall survival after SRS was 86% at 1 yr, 50% at 3 yr, and 44% at 5 yr. Smaller total tumor volume was associated with longer overall survival (P = .006). Twenty-two patients (grade 2: n = 9, grade 3: n = 13) developed additional recurrent ependymomas in the craniospinal axis. The progression-free survival in cases treated with SRS was 71% at 1 yr, 56% at 3 yr, and 48% at 5 yr. Adult age, female sex, and smaller tumor volume indicated significantly better progression-free survival. Symptomatic adverse radiation effects were seen in 8% of cases.[41]
Actually, SRS provides another management option for residual or recurrent progressive intracranial ependymoma patients who have failed initial surgery and RT, we recommend consider this option in your cases
The intraventricular subependymomas are rare benign tumors. Depend on location and size they become symptomatic due to CSF outflow obstruction causing hydrocephalus.
The ideal treatment for a symptomatic subependymoma is total resection safe and feasible, if this is not possible, debulking of the tumor followed by SRS or radiation therapy.
Tumor resection is required for symptomatic tumors or where there is radiological uncertainty. The good neurological outcomes can be achieved with microneurosurgery or endoscopic Surgical extirpation without postoperative radiotherapy results in excellent postoperative survival and functional outcomes for this type of tumors, particularly after gross total resection. Satisfying long-term survival and also cure is possible by complete removal. Some patients will require shunting for unresolved hydrocephalus after the resection surgical procedure.
Is recommended a large follow up for this patient, with clinical and radiological control to evaluate tumor recurrence.
To the patients, particularly the patient presented in this manuscript, also to all my colleagues during my career. Also, to all members of my family for the support.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
