
Case Report | DOI: https://doi.org/10.31579/2690-4861/543
1Department of Neurosurgery, Taipei Medical University-Shuang Ho Hospital, Taiwan, ROC.
2Taipei Neuroscience Institute, Taipei Medical University, Taipei, Taiwan.
3Department of Surgery, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan.
*Corresponding Author: Chien-Min Lin and Jang Yu, Department of Neurosurgery, Taipei Medical University-Shuang Ho Hospital, No.291, Zhongzheng Rd., Zhonghe District, New Taipei City, 23561, Taiwan (R.O.C.).
Citation: Jang Yu, Bing H. Hsu, Chien M. Lin, (2024), Surgical Management And Prophylactic Antibiotic Treatment Of Pneumatic Nailer Penetrating Brain Injury: a Case Report and Literature Review, International Journal of Clinical Case Reports and Reviews, 19(3); DOI:10.31579/2690-4861/543
Copyright: © 2024, Chien-Min Lin and Jang Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 September 2024 | Accepted: 11 October 2024 | Published: 30 October 2024
Keywords: penetrating traumatic brain injury; craniotomy; prophylactic antibiotics
Penetrating traumatic brain injury (pTBI) can lead to high mortality and life-threatening complications. The thorough examination and proper treatment are required. A 30-year-old man suffered from the pTBI during work, and the non-contrast computed tomography (CT) scan was revealed the metallic rod penetrated the right temporal skull and extended into the right inferior temporal gyrus, accompanied by subarachnoid hemorrhage. After diagnosis, a right frontotemporal craniotomy with intracranial nail extraction was performed, and prophylactic antibiotics were prescribed. The patient's symptoms resolved, and he was discharged without focal neurological deficits.
pTBI is associated with a high mortality rate and poor prognosis. pTBI induced by objects such as needles, iron rods, wood pieces, and nails is uncommon. Since the introduction of pneumatic nailers in construction in 1959, several cases of intracranial injuries caused by nails have been reported. Most cases of pneumatic-nailer-induced pTBI are due to work-related incidents, but some occur as a result of suicide attempts. Surgical management may be considered due to brain parenchyma injury. This report presents a case of pneumatic-nailer-induced pTBI and the subsequent surgical management and prophylactic antibiotic treatment.
A 30-year-old man was referred to our emergency room (ER) after a nail from a pneumatic nailer penetrated his skull when working as an interior decorator. The incident occurred when he fell and accidentally fired into his right temple. He had no recent history of head injuries or systemic illnesses. In the ER, the patient’s chief complaint was cephalalgia and mild vertigo. However, he demonstrated no focal neurological deficit. His Glasgow Coma Scale score was 15, and his modified Rankin Scale (mRS) score was 0. A depression was visible in his right temporal region, with mild local inflammation (Figure. 1A).

Figure 1A: A metallic nail was inserted into the right side of the face(arrow).
A non-contrast CT scan was promptly obtained, which revealed a metallic rod with diameter of 2mm and length of 55.3mm positioned above the zygomatic process of the temporal bone; the rod penetrated the right temporal skull and extended into the right inferior temporal gyrus. The imaging also demonstrated a subarachnoid hemorrhage involving the right temporal lobe and Sylvian fissure (Figure. 1B-1D).
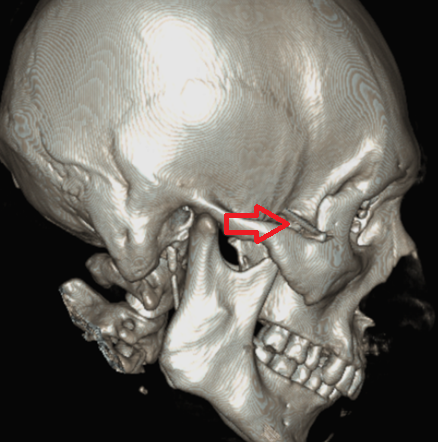
Figure 1B: A metallic rod was positioned above the zygomatic process of the temporal bone(arrow).

Figure 1C: The metallic rod had penetrated the right temporal lobe(arrow).
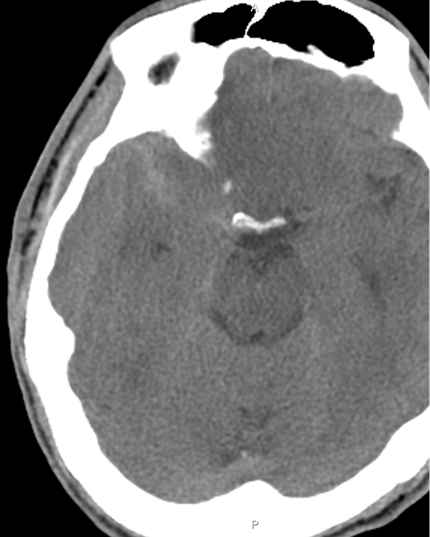
Figure 1D: The non-contrast CT scan revealed subarachnoid hemorrhage involving the right temporal lobe and Sylvian fissure.
After the surgical intervention was explained to the patient, a right frontotemporal craniotomy with intracranial nail extraction was scheduled. Under general anesthesia, the patient was positioned supine on the operating table with the head slightly tilted to the left. The operative field was meticulously prepared, sterilized, and draped using a standard aseptic technique. A curvilinear incision was made over the right frontotemporal region, posterior to the hairline and inferior to the zygomatic arch, providing direct access to the puncture site of the nail (Figure. 2A).

Figure 2A: A curvilinear incision was made over the right frontotemporal region (red dotted line).
The incision was deepened, and the galea aponeurotica was meticulously dissected from the underlying muscle layer, with caution exercised to avoid injury to the superficial temporal artery. A craniotomy measuring approximately 5 × 3 cm was performed on the right temporal bone, positioned superior to the nail (Figure. 2B).
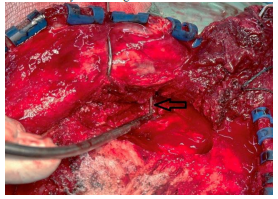
Figure 2B: The metallic nail was exposed during the craniotomy(arrow).
A dura tenting suture was placed initially to control active bleeding and prevent the formation of a secondary epidural hematoma. Profuse bleeding was noted around the nail, necessitating a pin cutter to sever the nail after the dura was carefully opened. Upon removal of the intracranial portion of the nail, oozing from multiple small vessels along the nail tract was observed. Bipolar coagulation and Surgicel, an absorbable hemostatic agent made from oxidized regenerated cellulose, were employed to achieve hemostasis. The remaining nail portion was then extracted from the skin, and the nail track was irrigated with a vancomycin solution. The bone flap was subsequently replaced and secured using mini plates. The extracted nail measured approximately 2 mm in diameter and 50 mm in length (Figure. 2C).
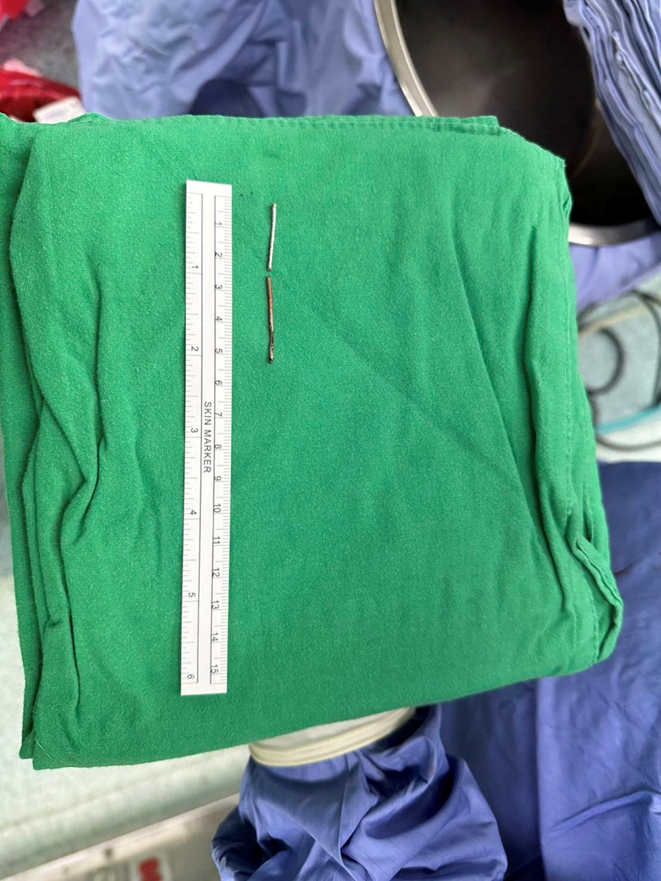
Figure 2C: A metallic nail, approximately 2 mm in diameter and 50 mm in length, was removed.
The patient was administered 500 mg of oxacillin via intravenous drip every 4 hours as part of a prophylactic antibiotic regimen, along with a prophylactic anticonvulsant. The patient’s symptoms were resolved postoperatively, and no focal neurological deficits were noted. The patient was discharged with an mRS score of 0 and demonstrated no signs of infection, seizure activity, or other neurologic deficits during the 3-month outpatient clinic follow-up.
Cases of pTBI engendered by pneumatic nailer incidents are rare, with the majority of cases occurring as a result of occupational accidents. When pTBI involves major vascular injury, it can lead to life-threatening complications. However, most cases require surgical intervention to remove the foreign object. Delaying the removal of intracranial foreign objects can result in complications such as central nervous system (CNS) infection, local inflammatory responses, and foreign-body displacement, potentially leading to further vascular and neural tissue damage.
Currently, guidelines for prophylactic antibiotic treatment following pTBI are not available. However, in cases where a CNS infection caused by methicillin-sensitive Staphylococcus aureus is suspected, nafcillin and oxacillin are the recommended antibiotics.
In our case, owing to the presence of subarachnoid hemorrhage at the penetration site, emergent surgical removal of the metallic nail was performed, and hemostasis was achieved. The penetration track was irrigated with vancomycin solution, and intravenous oxacillin was administered to prevent CNS infection.
Skull X-ray scans are effective for screening penetrating materials and detecting skull fractures; however, they have a high false-negative rate when the penetrating materials are radiolucent, such as glass, plastic, or wood.
Thus, the gold standard for diagnosis is non-contrast CT, which accurately identifies the location and characteristics of the foreign object, the trajectory of penetration, and the presence of intracranial hemorrhage and skull fractures.
Additionally, 3-dimensional CT imaging is invaluable for the detailed assessment of bony structures and assisting in preoperative planning.
In our case, non-contrast CT scan was performed to diagnose the metallic nail penetration and associated intracranial hemorrhage, followed by 3-dimensional CT imaging for preoperative planning.
For safety considerations, removing the penetrating foreign body under direct visualization is crucial to prevent complications such as subdural hematoma and intraparenchymal hemorrhage. Preoperative angiography should also be considered for a thorough evaluation, especially if vascular structures are damaged. In some cases, preoperative therapeutic embolization may be warranted. We performed a craniotomy around the foreign body and removed the metallic nail under visualization, followed by appropriate hemostasis. The literature includes a few reports of single metallic nail being removed through gentle traction under local anesthesia, and this is because intracranial hemorrhage is uncommon in such cases. However, our patient’s preoperative CT scan revealed subarachnoid hemorrhage, necessitating craniotomy under general anesthesia to control bleeding.
Careful evaluation of the patient’s psychological status is crucial in postoperative treatment, as some cases may be associated with mental health issues. Psychiatric intervention may be necessary to address any underlying psychological disorders and to prevent the recurrence of such incidents. According to the patient’s father, the injury occurred while the patient was engaged in a home renovation project. Notably, the patient had no prior history of psychological disorders. Three months postoperatively, the patient fully returned to his daily work without any neurological deficits or psychological complications.
Immediate management of pneumatic-nailer-induced brain injury is crucial, with a preference for metallic nail removal under direct visualization through craniotomy, particularly in patients presenting with preoperative hemorrhage. Although no formal guidelines exist for pTBI, prophylactic antibiotics are recommended to prevent potential infection.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
