
Research Article | DOI: https://doi.org/10.31579/2692-9759/062
1Republican Specialized Center of Surgery named after academician V. Vahidova.
2Bukhara State medical institute after named Abu Ali ibn Sina
*Corresponding Author: Abdumadjidov, professor of the department surgical disease and reanimation, Bukhara State Medical institute
Citation: Abdumadjidov Kh, Buranov H.J, Isomitdinov B.Sh. (2022) Surgical Correction of Tricuspid Component of Patients with Multi-Vessel Heartdefect.. J. Cardiology Research and Reports 4(5); DOI: 10.31579/2692-9759/062
Copyright: © 2022, Abdumadjidov Khamidulla Amanullaevich, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 March 2022 | Accepted: 17 May 2022 | Published: 05 May 2022
Keywords: tricuspid component; multi-vessel heartdefect; tricuspid pathology
The analysis of results of surgical correction of 326 (8%) patients with tricuspid pathology in rheumatic multi-valve heart defects. The age of our patients ranged from 12 to 74 years (mean 36.7 + 9.4). Women were 220 (67.5%), while men - 106 (32.5%). According to the degree of circulatory disorders, patients were divided according to the classification of chronic heart failure (CHF) in NYHA, where in functional class III were assigned 24 (7.4%), and to IY functional class NYHA - 302 (92.6%) patients. The clinic is the most commonly used plastic fibrous ring by De Vega. Of the 262 (80.5%) operated by the method of De Vega, at 26.9% after correction of regurgitation on tricuspid valve (TC) virtually disappeared, at 62.8% - regurgitation decreased from a low of 1 degree, and the remaining 10.3% were operated last was reduced to 2 (moderate) degree. In 8 (2.46%) cases of infective endocarditis was made "open" correction - prosthetics TC biological prosthesis. Known methods of creating a bicuspid tricuspid valve - Kay Reed Kay Boyd used in 13.4% of cases, but in recent years because of the low efficiency of data communication techniques greater preference for annuloplasty by De Vega.
The study showed: when hemodynamically insignificant defects from TC correction can be avoided. When regurgitation grade 2-3 (combination of stenosis and insufficiency) seemed tricuspid component defect correction. Due to the possibility of complication ventricular insufficiency in cases with highpulmonary hypertension hyper corrections unacceptable.
According to statistics, the cause of the combined heart disease is often a rheumatism, approximately 60-65% of cases, in the development of multi-valve heart defects also reveal rheumatoid history. Based on data from the statistics - a year in our country is in need of surgical correction of acquired heart diseases, about 14-15 thou. patients, of whom half are diagnosed multivalve heart defects [2; 4; 6, 7].
Progress cardiac science of recent decades confirms the possibility of correction of multi-valve heart defects with a fairly good result. This is facilitated by the improvement of methods of diagnostics and surgical tactics, the development of different ways of reconstructive operations, the improvement of anesthesia and improved methods to protect the myocardium and postoperative management of this difficult group of patients. In patients with multi-valve heart disease is difficult to resolve the issue - whether correcting accompanying Moderate malformation of the tricuspid valve (TV)? Conservative tactics, as experience shows, is justified only when hemodynamically insignificant lesions of the tricuspid heart valve [1, 3, 5]. Thus, the defect correction of tricuspid (DCT), as well as correction of the other components of a complex multi-valve rheumatic heart disease is important in achieving good immediate and late results of operations.
The Department of Reconstructive Surgery of acquired heart defects JSC RSCS named after academician V. Vahidov over the past 12 years operated 4077 patients under extracorporeal circulation (EC) with cardioplegia (CP) and 326 (8%) cases of them performed tricuspid surgical correction. The age of our patients ranged from 12 to 74 years (mean 36.7 + 9.4). Women were 220 (67.5%), while men - 106 (32.5%). According to the degree of circulatory disorders, patients were divided according to the classification of chronic heart failure (CHF) in NYHA, where in functional class III were assigned 24 (7.4%), and to the IV NYHA functional class - 302 (92.6%) patients. Surgical correction in our patients was performed under extracorporeal circulation (EC) and cardioplegia (CP). The nature of the corrections made multi-valve, with tricuspid component is presented below.
Tricuspid surgical corrections by gender and classification
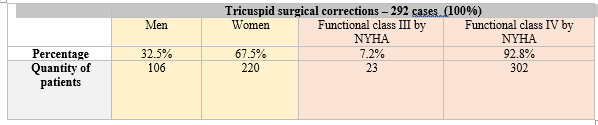
The nature of the corrections made multivalvewith tricuspid component.
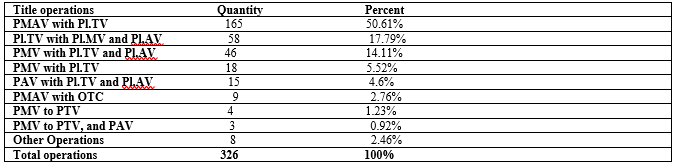
* PMAV- prosthetics of mitral and aortic valves,
Pl.TV –plasty of tricuspid valve,
Pl.MV - plasty of mitral valve,
Pl.AV - plasty of aortic valve,
PMV - prosthetics of mitral valve,
PMV - prosthetics of mitral valve,
PAV – prosthetics aortic valve,
PTV - prosthetics of tricuspid valve,
OTC - open tricuspid commissurotomy.
In the diagnosis of multi-valve of acquired heart disease in addition to general clinical research methods, used highly informative, invasive, non-invasive methods of diagnosis: electrocardiography, transthoracic and transesophageal echocardiography (TEE) with Doppler, radioscopy of the chest, computed tomography (CT), coronaroventriculography (CVG) with aortography (AG), if necessary, and angiocardiography (ACS). By the nature of the corrections made to the multi-valve tricuspid component, it can be said that performed prosthetic valves: prosthetics of mitral and aortic valves (PMAV), aortic valve replacement (AVR), mitral valve (PLA), and tricuspid valve prosthesis (PTC). Recent combined with mitral plasty (Pl.MK), aortic (Pl.AK) and tricuspid valves
According to the analysis of clinical material and the results of the executed corrections can show the following: predominantly TP heart combined with mitral disease (MD) when the congestion of the pulmonary circulation (PC) is enhanced, and partly as a compensatory mechanism of the body to progressive pulmonary hypertension (PH), there is tricuspid insufficiency (TI) varying degrees. Isolated tricuspid valve damage occurs, as we know, rarely. Therefore, the decision to issue the surgical correction of the combined TA solved more often as an additional component of the multi-valve heart disease.
By etiological causes are rheumatic TC defeat as a result of infective endocarditis, degenerative valve changes, specific and traumatic. In our practice, the most frequent causes of TP were rheumatism, infective endocarditis. Based on the above diagnostic methods, in 326 cases (8%) identified multivalve heart defects that have been performed on indications one or other "open" correction of tricuspid pathologies, combined and other corrections. In this category of patients, a variety of options for the surgical correction of the TA were performed, starting from the open tricuspid commissurotomy (OTC) with chondroplasty, ending the incompetent tricuspid valve prosthesis. The nature and amount of the executed "open" multi-valve defects correction with tricuspid component results in table №1. As we have seen, we carried the heavy volume correction of the three valves, of which the most frequently performed mitral and aortic valve replacement with plastic TK. But more fulfilled valve saves reconstructive plastic surgery in this group of patients in recent years. As we know, TC pathology develops special scenario: if the expansion of the fibrous ring (FC), TCs develops in the direction of the front and rear flaps intact remains mostly septal flap. The defeat of infective endocarditis is also developing in this direction. This creates the need to reinforce said portions FC unlike the mitral valve. In addition, the development failure, TK plays an important role development of pulmonary hypertension (PH), a high degree. As practice shows, and our observations, the need for a high degree of regurgitation TC correction specifies mandatory monitoring of regression of PH. If necessary, it is better to leave a small degree of regurgitation in the TC based regression of PH, as early postoperative overcorrection TK leads to the development of right heart failure. In view of this, we tend to choose a correction in the form of annuloplasty FC TC, sometimes in combination with an open tricuspid commissurotomy with chondroplasty. According to the literature analyzing the results to date are known several types of annuloplasty FC and TC plastics: Kay Reed, Kay Boyd, also De Vega methods (pic.1,2,3,4).
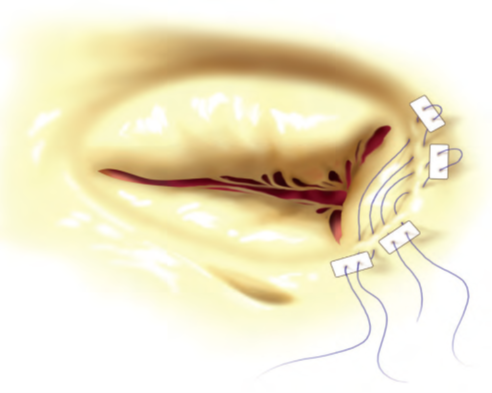
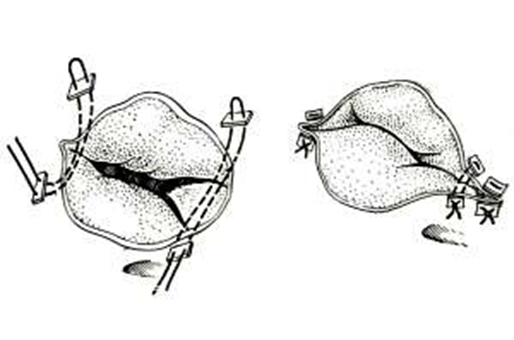

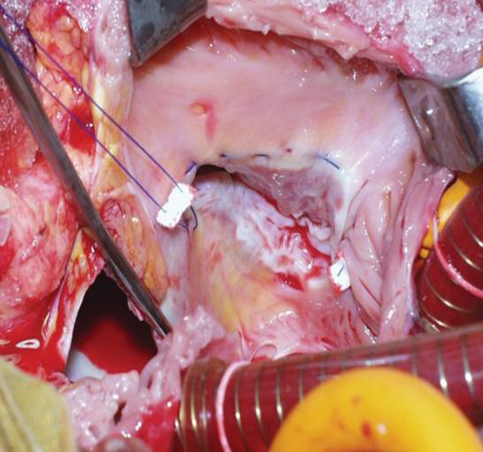
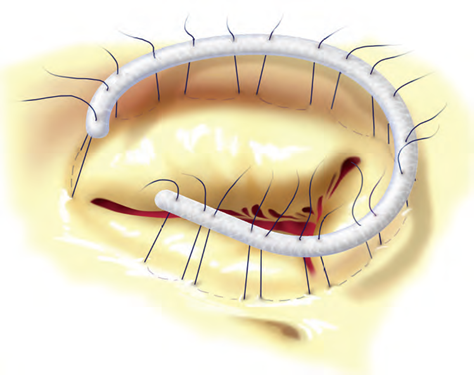
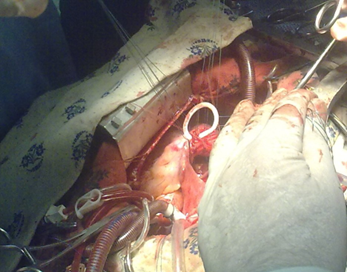
Used and annuloplasty FC TC by means of support rings (usually ring Carpentier - Edwards, 5b). Among these operations, methods, most commonly performed types of valves save corrections tricuspid heart disease. In our clinic, the most commonly used plastic for TC FC De Vega (pic.3,4). Such corrections were in 262 (80.5%) cases. From these 262 patients who was received valve save correction by method De Vega showed the 26.9% - regurgitation practically disappeared, in 62.8% - regurgitation is decreased from minimum to 1 degree and the remaining 10.3% were operated last was reduced to 2 (average) degree. Imposing double pure string in the fibrous ring TC performed with using of Ethibond 2/0 or Prolene 2 / 0-3 / 0 (pic.3,4). Monitoring the adequacy of plastics need to carry out with the help of an obturator with a diameter of 35mm (for women), and up to 40mm (for men). Sometimes applied finger adequacy of control method narrowing FC TC. The result is visually monitored and water sample. In 9 (2.76%) cases, the combined TA (i.e., stenosis and insufficiency), the latter supplemented by open commissuretomy and tricuspid chordoplastic. When TC failure due to annulodilatation annuloplasty was performed FC on a support ring, only 4 (1.23%) were applied Carpentier-Edwards ring (5b). Previously widely used and the method of creating a bicuspid TC method Kay Boyd and Kay Reed. The latter technique was performed in 13.4
1. When the relative valve insufficiency with regurgitation before the 1st. correction of tricuspid defect can be avoided.
2. The presence of regurgitation grade 2-3 TC considered indications for surgical correction of the latter.
3. If you have a high LH should refrain from overcorrection of TP, since small residual regurgitation TC in the early postoperative period is essential for preventing the development of right ventricular failure.
4. Adequately performed correction of tricuspid component with multi-valve heart defects, and improves results of surgical treatment in the immediate and in the long periods of observation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
