
Case Report | DOI: https://doi.org/10.31579/2690-8808/116
1 First Clinical Medical School, Lanzhou University, Lanzhou, China.
2 Department of General Obstetrics and Gynecology, the First Hospital of Lanzhou University, Key Laboratory of Gynecologic Oncology of Gansu Province, Lanzhou, Gansu 730000, China.
3 Kent State University, Ohio, USA, 44240
*Corresponding Author: Chang Liu, Department of Obstetrics and Gynecology, First Hospital of Lanzhou University, Lanzhou 730000, Gansu Province, China.
Citation: Ting Lei, Xinru Lu, Yun Lu, Chang Liu. (2022). Surgery combined with BEP chemotherapy regimens for Malignant Struma Ovarii: A case report Journal of Clinical Case Reports and Studies 3(6); DOI: 10.31579/2690-8808/116
Copyright: © 2022 Chang Liu, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 April 2022 | Accepted: 03 June 2022 | Published: 27 June 2022
Keywords: struma ovarii; chemotherapy; surgery
A case of malignant struma ovarii (MSO) diagnosed and treated by the staffs of the Department of Gynecology in the First Hospital of Lanzhou University was reported. MSO is a form of malignant germ cell tumor of the ovary with a very low incidence rate. Surgery is the primary treatment approach for it. The decision of surgical method depends on the fertility preservation requirement by the patient, the tumor conditions and staging. Adjuvant treatment should be performed postoperatively.
Struma ovarii (SO) is a rare form of monodermal teratoma that is composed entirely or predominantly (over 50%) of thyroid tissue, representing 0.5% to 1% of all ovarian tumors, or 5% of ovarian teratoma [1,2]. Those teratoma having less than 50% thyroid tissue but the thyroid tissue demonstrates historical or biological malignancy, are also considered as Struma ovarii. Malignant struma ovarii (MSO), representing 5-10% of all struma ovarii (SO), refer to those SOs that met the criteria of malignant thyroid tumors (historically malignant) or those SOs that have been found metastasized (biologically malignant) [3,4]. Only less than 300 cases of MSO have been reported so far. In previous literatures, MSO is often mistakenly used to describe stromal carcinoid of the ovary or medullary thyroid carcinoma in ovary, therefore, some researchers think it is more accurate to be named “thyroid-like carcinoma derived from ovary”5. The present study reported a case of MSO, reviewed related literature and discussed the diagnosis, treatment and prognosis of MSO.
In recent years, the incidence of MSO has been on the rise. Here, we successfully performed total abdominal hysterectomy/bilateral salpingo-oophorectomy (TAH/BSO) combined with BLM, DDP, Etoposide VP-16(BEP) treatment on a patient with MSO.
A female patient was diagnosed with an ovarian cyst at age 48 when she got the health examination (Fig. 1. A, B, and C). The patient underwent oophorocystectomyin in March 2020 due to a pelvic mass in Wuwei hospital. During the operation, a soft, cystic mass (6.0 cm 5.0 cm) with a smooth surface was found in the left ovary and (5.0 cm 4.0 cm) in the right ovary. Uterine and bilateral fallopian tubes were normal. The postoperative pathological examination results were as follows: left side: ovarian cystic teratoma with partially malignant thyroid tissue; right side: mature ovarian teratoma. The immunohistochemical results for the teratoma on the right side are TTF-1(+), TG (+), CK19/Ki-67(5%-10%), P53(<5%), Galectin-3(focal +), Syn (-), HBME (focal +). The diagnosis was clear, and the patient was suggested to be treated in a hospital with a higher level.
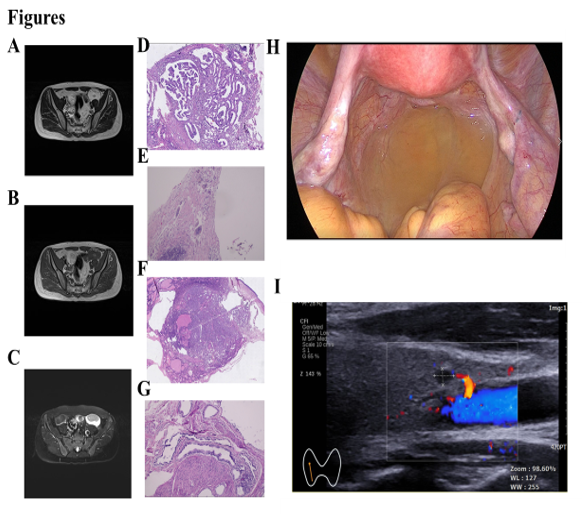
The patients came to the First Hospital of Lanzhou University for further diagnosis and treatment in April 2020. Department of Pathology consultation in our hospital showed the following: left side: ovarian cystic mature teratoma with thyroid tissue, accompanied with papillary thyroid carcinoma. The biggest diameter of cancerous foci was 9 mm (Fig. 1. D and E). Treated with BEP regime totally for 6 cycles (DDP 20mg/m2 D1-D5,VP-16: 100mg/m2 D1-D5, bleocin 30U/m2 D2), every 21 days, during which no clinical adverse effects occurred.After the fourth course of treatment, TAH/BSO was performed. No obvious abnormalities in the uterus, bilateral ovaries and fallopian tubes were observed during the operation, and the postoperative recovery was also satisfactory (Fig. 1. H). The pathology showed some degree of cellular pleomorphism in the left ovary, which was consistent with papillary thyroid cancer. The immunohistochemical results for the teratoma on the right side are: ckl (focal3+), CDX2(-), TTF-1(focal 3+), CK (focal 3+), TPO (-), ki67(focal 10%), ER (-) (Fig. 1 F and G).
The serology and imaging showed that both tumor markers and serum thyroxine were normal at the fifth month after surgery, and CT and MRI did not demonstrate any significant abnormalities. Therefore, tumor metastasis was not considered at this time. Ultrasound showed a hypoechoic nodule in the right lobe of the thyroid gland (TI-RADS III) (Fig. 1. I). Thyroid function tests reported a low thyroglobulin 4 (FT4) concentration of 0.59 (0.62-1.24 ng/dl) and a high anti-thyroglobulin antibody (TgAb) of 9.4 IU/ml (0-4.11 IU/ml). No other abnormalities were found on CT, MRI and other serological tests. After being discussed with a specialized endocrinologist, these abnormal results were not sufficient to diagnose tumor recurrence or metastasis, but close surveillance was still needed.
For MSO patients, TAH/BSO with BEP treatment may prolong survival and improve the quality of life. However, more studies are needed to further verify this regimen.
MSO is often diagnosed in female patients aged 40 to 50 years old [1]. The reported age of MSO patients ranges from 12 to 79, with an average of 43 and a median age of 48 years old. There is usually no specific clinical manifest of MSO at the early stage. The most common clinical symptoms are pelvic mass, abdominal pain and menstrual disorders. A vast majority of MSO is unilateral, more often found at the left side than the right side, and 7% of MSO are bilateral6,7. The expression of CA125 is within normal range for most of cases, with only 35% of patients showing increased CA125 level [7]. Approximately 17% of MSO patients have pseudo-Meigs syndrome, with the clinical manifests of ascites, pleural effusion and increased CA125 level. These patients often suffer from distending pain in the abdomen, poor appetite and enlarged abdominal circumference, which are similar to the symptoms of late-stage ovarian cancer. However, it is rare to find cancer cells in the ascites of MSO patients. About 9 % of MSO patients are diagnosed having primary thyroid cancer in the neck concurrently [7,8]. 5-8% of MSO patients also have hyperthyroidism. Although the underlying mechanisms behind the concurrency of MSO and hyperthyroidism is not clear, it is perhaps different from the causes of hyperthyroidism.
Usually, MSO is originated in thyroid goiter or mature cystic teratoma containing thyroid tissue6. A percent of 48% of MSO is pure thyroid goiter without other germline cells, another 48% of MSO is combined with mature cystic teratoma, and the last 4% of MSO is combined with myxoma. In 13% of MSO cases, teratoma without thyroid tissue are found in the ovary opposite to the MSO located side7. Classified by their pathological characteristics, multiple types of MSO have been reported in the literature, including papillary carcinoma (including follicular variant), follicular carcinoma (including acidophilic cell variant, clear cell variant and highly differentiated follicular carcinoma of ovarian origin), insular carcinoma and poorly differentiated carcinoma. A percent of 70% of MSO are papillary carcinoma including 44% classical papillary carcinoma and 26% follicular variant of it.
Follicular carcinoma represents approximately 30% of all MSO [8,9]. The diagnosis of MSO is mainly dependent on the postoperative pathological examination. The result of frozen section examination during the surgery is not completely accurate. Currently, there is no standardized diagnosis criterion for MSO. Most of the time, the diagnosis criteria for thyroid carcinoma located in neck is used for MSO diagnosis. The criteria for papillary carcinoma include irregular ground glass nuclei, papillary structure formed around the central core of fibrovascular tissue, and invasion of blood vessel etc. Immunobiologically, positivity of thyroglobulin (TG) and thyroid transcription factor-1 (TTF-1) is helpful for diagnosis. the expression pattern of human bone marrow endothelial cell marker-1 (HBME-1), CK-19 and CD56 is also helpful in papillary MSO diagnosis [6]. Histological malignancy does not necessarily suggest biological malignancy in MSO. Majority of MSO does not demonstrate malignancy clinically, while benign MSO defined by histological examination may metastasize out of ovary. Studies conducted by Shaco-Levy et al. revealed that large follicular structure and the lack of fibrosis are more frequently found in biologically malignant MSO, while the existence of trabecular structure is associated with benign biological behavior of the tumor.
Currently, there is no standard guideline for MSO treatment due to the rarity of MSO. Surgical removal is the primary treatment approach for MSO. Specifically, the surgical procedures include cystectomy, unilateral salpingo-oophorectomy at the affected side, total, hysterectomy and bilateral salpingo-oophorectomy, cytoreductive surgery and others6. Usually, MSO is diagnosed postoperatively. For many patients, staging procedure was not performed when they receive their first surgery. Thus, adjuvant treatments are required for these patients. Suitable adjuvant treatments include thyroidectomy combined with radioactive iodine therapy, radiotherapy and chemotherapy. The chemotherapeutic treatment can be performed by using Paclitaxel combined with Carboplatin, Etoposide, fluorouracil, Adriamycin, Vincristine or other chemotherapy drugs [7]. Most of chemotherapy are experiential chemo-treatment. Radiotherapy can be used during palliative care of patients with widely metastasis and patients who do not respond to I131 radioactive iodine therapy [8]. However, the treatment effect cannot be evaluated due to the extremely low number of cases.
It is believed that the prognosis of MSO is generally well. However, the mortality rate of MSO is no less than thyroid carcinoma. It was reported that the 5-year, 10-year and 25-year survival rate of MSO patients are 96.7%, 89.0-94.3% and 84%, respectively. Different relapse rate for MSO, ranging from 7.5% to 35%, has been reported.
The treatment plan involved in this study is subject to the patient’s informed consent and signed an informed written consent form. This case report and related images were published with informed written consent from the patient.
The authors declare that there is no conflict of interest regarding the publication of this paper.
This report is supported by Science and Technology Plan Project of Gansu Province (9).
The treatment plan involved in this study is subject to the patient’s informed consent and signed an informed written consent form. This case report and related images were published with informed written consent from the patient.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
