
Case Report | DOI: https://doi.org/10.31579/2690-4861/210
1 Department of Obstetrics and Gynaecology, Lady Hardinge Medical College,New Delhi, India.
*Corresponding Author: Kanika Chopra, Department of Obstetrics and Gynaecology, Lady Hardinge Medical College,New Delhi, India.
Citation: K chopra, Reena Y, B. Meena, Sukriti Ghai, Prerna Tayal (2022). Super-Refractory Status Epilepticus in Pregnancy-An Exigent
Management. International Journal of Clinical Case Reports and Reviews. 11(1); DOI: 10.31579/2690-4861/210
Copyright: © 2022 Kanika Chopra, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 March 2022 | Accepted: 31 March 2022 | Published: 04 April 2022
Keywords: status epilepticus; refractory status epilepticus; super-refractory status epilepticus; pregnant
Super-refractory status epilepticus is known as the seizure that persist beyond 24 hours even after administration of intravenous anesthesia drugs. It is a rare diagnosis especially in pregnant population and thus its management is also limited to case series and reports. Our case presented with this diagnosis and we managed it with three tier system of pharmacological agents and termination of pregnancy. Unfortunately, exact cause of the SRSE in our case was not found and patient has been discharged on dual antiepileptic drugs along with antidepressants with follow up in neurology out-patient department. It is important to keep one self-aware of the treatment protocol in cases of status epilepticus other than due to eclampsia.
Status epilepticus is defined as seizures that last longer than 5 minutes or two or more seizures without return to consciousness in between the seizures [1]. Status epilepticus turn refractory when seizures are recurrent despite two appropriately selected anti-epileptic drugs including benzodiazepine [2]. Super-refractory status epilepticus is defined when seizures persist beyond for at least 24 hours even after administration of intravenous anesthesia drugs [3]. Super-refractory status epilepticus is seen in 12-26% of general population with its incidence not known in pregnancy [4]. Any type of status epilepticus is associated with significant maternal and fetal morbidity and mortality. The causes of status epilepticus in pregnant women are hypertension, stroke, trauma, viral encephalitis, cavernous angioma, pyridoxine deficiency, reversible cerebral vasoconstriction syndrome, subarachnoid hemorrhage, NMDA receptor antibody mediated autoimmune encephalitis, non-compliance to anti-epileptic drugs and hormonal changes in pregnancy [5]. Management of any variant of status epilepticus pregnancy is challenging with non-availability of specific guidelines [5]. We, present this case of super-refractory status epilepticus with non-identification of any specific cause and gradual improvement post-delivery with titration of multiple anti-epileptic drugs. This review will help the obstetricians dealing with pregnant woman with status epilepticus.
Patient, 20-year-old, Primigravida at 32 weeks of gestation presented to our hospital emergency with complaint of recurrent seizures since last 12 hours. On presenting to our emergency, she again had recurrent seizure episodes without gain of consciousness in between. On enquiring from accompanying attendants, we found that patient was carrying well her pregnancy with two antenatal visits in a nearby health center. There was history of headache for 5 days prior to presenting along with low grade fever. She had normal blood pressure records till now and there was no history of seizures or head trauma. On examination, her Glasgow coma scale was E1V1M1 i.e., 3/15. Her vitals were, temp 37.40 C, pulse rate 110 beats per minute, blood pressure 122/76 mmHg which remained normal all throughout her stay, respiratory rate 34 per minute and saturation at room air 95%. There was no pallor, icterus, edema, cyanosis or generalized lymphadenopathy or signs of meningeal irritation. Bilateral pupils were mid-dilated and deep tendon reflexes were absent. On cardiovascular examination, S1S2 were normal and on chest examination, bilateral coarse crepts were present which was most probably due to aspiration. Obstetric examination revealed a gravid uterus corresponding to 32 weeks. Fetus was in cephalic presentation and fetal heart sound was 120 beats per minutes. Arterial blood gas analysis (ABG) was done along with remaining baseline blood investigations i.e., complete blood count, liver and kidney function tests, serum calcium levels, random blood sugars, antinuclear antibody, RA factor and sepsis panel. Chest Xray, ECG and Fundus examination were also done.ABG was suggestive of metabolic acidosis, hemoglobin was 9.7 gm%, total leucocyte counts 27,000/mm3, platelet count 2.59 lakh/mm3, liver and kidney function tests were normal, serum calcium and magnesium levels were also normal. Urine routine microscopy did not reveal proteinuria or any other significant findings. ANA and RA factors were negative. Procalcitonin, high sensitive C-reactive protein, lactate dehydrogenase were 0.4 µg/L, 4.5 mg/dl and 265U/L respectively. Chest Xray, ECG and fundus examination were normal. The management was started simultaneously along with the investigation panel. She was given intravenous injection of midazolam 2mg stat and following airways, breathing and circulation, oxygen was started at 4L/minute, mouth gag was placed, she was nursed in left lateral position, side bed railings raised and IV cannula secured. As, she had another seizure episode in less than 2 minutes of last fit, she had drop of saturation to less than 60 % and also fall in blood pressure. Loading dose of injection levetiracetam given, noradrenaline started and was intubated. She was started on midazolam and rocuronium infusion. Inspite of being under anesthesia, she continued to have seizures. Loading dose of injection valproate was given and doses of both antiepileptic drugs titrated to increasing doses gradually. She was also started on injection piperacillin tazobactam combination with clindamycin considering the possibility of sepsis. Termination of pregnancy was planned and she delivered on day 2 of her presentation and had atonic post-partum hemorrhage which was managed medically. Baby was admitted in NICU. NCCT head and EEG was planned to identify the possible cause of status epilepticus. NCCT head revealed sub centimetric calcified granuloma and EEG was normal. As per neurologist and physician opinion, these findings were not the reason for her seizures. On day 5 of her presentation and after 24 hours of seizure free period, patient was extubated and was continued on two anti-epileptic drugs which were gradually tapered from intravenous to oral dosing. All her cultures sent were negative for any growth and her antibiotics were also stopped on day 7 of her presentation. On day 12 of presentation, patient complaint of low mood and suicidal tendency, psychiatric opinion was sought and started on antidepressant (selective serotonin reuptake inhibitor) along with antiepileptic drugs. Patient is doing well on above mentioned drugs and have been advised follow up in neurology and physiatry departments.
Status epilepticus (SE) has an incidence of 12.6 per 100,000 in general population [4]. Incidence of super-refractory status epilepticus is not known in general population and more so rare in pregnant population. Our case was of a super-refractory status epilepticus. Status epilepticus may become refractory in patients with severe brain injury due to either trauma, stroke or infections. In others, causes may be heterogenous. In previously healthy patients, refractory or super refractory status epilepticus (RSE/SRSE) is referred to as new onset. These can be convulsive or non-convulsive or both types can exist together.
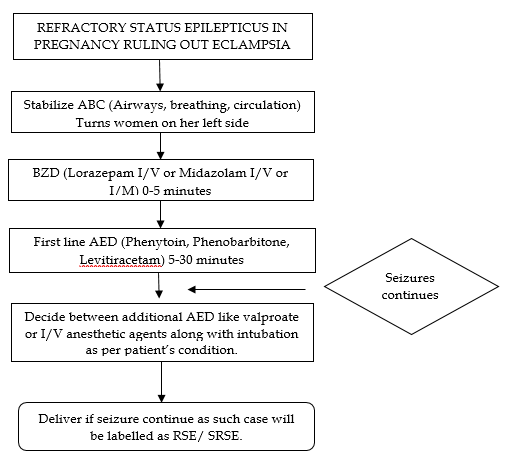
After continuous seizure activity for more than 30 minutes they can become self-sustaining. Convulsive type of seizures can cause more harm to the patient in the form of aspiration pneumonia, pulmonary edema, myocardial ischemia leading to sudden hypotension and renal failure. Two of these complications were seen in our case as well. Such events are known to be catastrophic to the fetus as well by causing fetal hypoxia. SE can be life threatening and thus warrants multidisciplinary management. The causes of status epilepticus in pregnancy are defined but, in many cases, we may not be able to find a definite cause as in our case. Hormonal alteration in pregnant women can have an effect in exciting seizure activity. Decrease in blood estrogen levels will excite the activity of glutamate decarboxylase enzyme and synthesis of gamma amino butyric acid in brain will decrease thus exciting the epileptic seizures [6]. Exacerbated response of maternal immune system to fetus may be the source of autoimmunity to brain [7]. In a review by K.R. Rajiv et al, around twenty-nine cases of status epilepticus were included and the most common cause of SE was eclampsia [5]. They also emphasized the lack of treatment protocol for SE in pregnancy and suggested one such which are more the less similar to the protocol we followed in our case as seen in figure 1. Benzodiazepine, anti-epileptic drugs and anaesthesia drugs are the three tiers of pharmacological treatment to terminate seizures. Treating gynecologist should be aware of the protocol so that in settings where neurologists are not available, they can do the management and prevent morbidity and mortality of both the mother and the fetus. Another aspect of the treatment is planning termination of pregnancy as in a study by H. Alibas et al, it was found that RSE resolved post-delivery and thus the reason for planning termination in our case as well [3]. In another case reported by Chinedu G Obikili et al, patient presented at 32 weeks of gestation with status epilepticus which gradually improved post-delivery [8].
SRSE diagnosis and management is challenging especially in pregnant population. If left untreated can be associated with high maternal and fetal morbidity as well as mortality. As the treatment protocol existing for SE due to eclampsia, there should be a well-defined investigation panel and treatment regimen in order to ensure optimal management. Aim should be to identify the underline cause, abort the seizures and plan appropriate fetal management. There should be a standard operating protocol in each health center dealing with such cases
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
