
Case Report | DOI: https://doi.org/10.31579/2641-0419/510
1Department of Anesthesiology, National Taiwan University Hospital, Taipei, Taiwan.
2Department of Surgery, National Taiwan University Hospital, Taipei, Taiwan.
*Corresponding Author: Ya-Jung Cheng, Department of Anesthesiology, National Taiwan University Hospital, No.7, Zhongshan S. Rd., Zhongzheng Dist., Taipei City 100, Taiwan.
Citation: Meng J. Lee, I-Hui Wu, Ya J. Cheng, (2025), Sudden Intraoperative Variations in Patient State Index Monitoring with Stable Cerebral Oximetry: A Case Report of Multiple Intraoperative Embolisms Following Bypass Transition in Open Repair of Type B Aortic Dissection, J Clinical Cardiology and Cardiovascular Interventions, 8(13); DOI:10.31579/2641-0419/510
Copyright: © 2025, Ya-Jung Cheng. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 August 2025 | Accepted: 11 September 2025 | Published: 17 September 2025
Keywords: intraoperative stroke; patient state index; aortic dissection open repair; cerebral oximetry
The detection of intraoperative stroke is paramount for enhancing patient outcomes during major vascular surgical procedures. Prior studies have demonstrated that alterations in cerebral blood flow (CBF) resulting from surgical interventions can be identified through a variety of neuromonitoring techniques, including electroencephalography, neurophysiological evoked potential assessments, transcranial Doppler ultrasound, and near-infrared spectroscopy. In this report, we present a case involving an open repair for type B aortic dissection that was complicated by extensive, multifocal cerebral infarctions. A notable intraoperative decline in the Patient State Index (PSI) and a concomitant rise in the Suppression Ratio (SR) were observed immediately following the transition of bypass modalities. This decline in PSI did not recover by the conclusion of the surgical procedure, despite only minor fluctuations in blood pressure and cerebral oximetry. Continuous monitoring of the PSI may facilitate the early detection and differentiation of intraoperative strokes, even in the absence of compromised CBF.
Open surgery for type B aortic dissection poses considerable risks of stroke and paraplegia.[1] Intraoperative strokes are often detected only when patients experience delayed awakening during recovery. In cardiovascular surgery, neuromonitoring commonly utilizes both the SEDLine Patient State Index (PSI) array and bilateral cerebral O3 oximeter sensors. While cerebral oximetry is recognized as an effective method for identifying cerebral ischemia, SEDLine serves as a brain function monitoring, which may be affected by distortion during bypass due to hypothermia. [2,3] In this case, however, significant intraoperative changes in PSI happened, even though cerebral blood flow and oximetry readings remained relatively stable, without recovery after weaning from bypass. Intraoperative variations in PSI monitoring, along with stable cerebral oximetry, may serve as an early warning sign of cerebral compromise rather than indicating decreased blood flow
A 65-year-old male with a history of chronic type B dissecting aortic aneurysm (DAA) extending from zone 3 to zone 9, characterized by an entry point at zone 3 and involvement of the right renal artery within the false lumen, was admitted for a scheduled open repair of the thoracic aortic aneurysm. His previous surgical history included distal abdominal aortic intimal flap fenestration enlargement and subsequent distal abdominal aortic true lumen stenting, followed by stenting of the distal thoracic aortic true lumen. Additionally, his medical history comprised sigmoid colon intramucosal carcinoma, for which he underwent laparoscopic anterior resection, as well as hypertension, type 2 diabetes mellitus, and hyperuricemia, all of which are managed with appropriate pharmacological therapy.
In the operating room, a SEDLine Patient State Index (PSI) array and bilateral cerebral O3 oximeter sensors positioned on the patient's forehead in accordance with the manufacturer's guideline besides standard monitoring, arterial and central venous lines. General endotracheal anesthesia was administered; an endobronchial blocker was employed to occlude the left main bronchus to facilitate right lung ventilation during the procedure. Following the positioning the patient in the right lateral decubitus position and a left thoracotomy, systemic heparinization was initiated, cardiopulmonary bypass (CPB) was initiated via the left common femoral vein–left common femoral artery (LCFV–LCFA) circuit[4], with systemic cooling to 34°C. Aortic cross-clamping (AXC) was performed at zones 2 and 5. The diseased descending aorta was excised and replaced with a 30mm Terumo vascular graft. Proximal anastomosis was performed. During the phase 1 CPB, the upper body was perfused by the native heart, while the lower body was supported by CPB. With acutely, compromised venous return from lower body from preparation and initiation of the phase1of CPB, anesthetic management had reversed the compromised cerebral oximetry and high PSI before starting the phase 1 CPB.
Upon completion of the proximal anastomosis, the zone 2 axillary cross-clamp (AXC) was released while the distal portion of the vascular graft remained clamped. The cardiopulmonary bypass (CPB) was transitioned to the left common femoral vein (LCFV) and the 24Fr Argyle side branch of the Terumo graft. After transition to phase 2 CPB, the flow from CPB through the 24Fr Argyle cannula was augmented to enhance perfusion to the upper body. Notably, immediately following the transition of the bypass, the Patient State Index (PSI) experienced a significant decrease to 14, accompanied by a concurrent increase in the Suppression Ratio to 50 with the unremarkable changes on cerebral oxymetry as shown in Figure 1.
Following the completion of the anastomosis of the distal descending aorta, de-airing, rewarming, and weaning from cardiopulmonary bypass (CPB) were performed sequentially. Protamine was administered to reverse heparin[5], hemostasis was achieved, and bilateral pleural chest tubes were inserted prior to layered wound closure. At the conclusion of the surgical procedure, the Patient State Index (PSI) was recorded at 21, with a Suppression Ratio (SR) of 14. The cerebral oximetry values were 64 on the right and 62 on the left. The alterations in PSI and cerebral oximetry are illustrated in Figure 1.
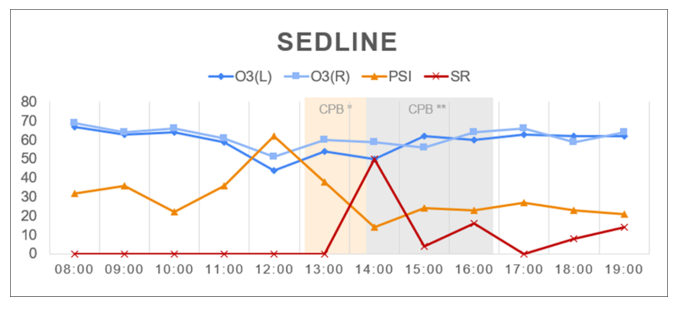
Figure 1: PSI and cerebral oximetry trend in operative room. CPB*, phase 1 cardiopulmonary bypass via lower body with upper body supplied by native heart. CPB**, phase 2 CPB transitioned to femoral vein and 24Fr Argyle side branch of Terumo graft.
Postoperatively, approximately five hours after the completion of the surgical procedure, the patient exhibited external rotation of the left upper limb, followed by a generalized tonic-clonic seizure lasting two minutes, which resolved following the administration of intravenous lorazepam [6]. Subsequently, levetiracetam was administered as a loading dose. A brain computed tomography (CT) scan revealed multiple infarctions (Figure 2), necessitating a neurologic consultation. Electroencephalogram (EEG) and magnetic resonance imaging (MRI) findings indicated diffuse brain hypoperfusion, prompting the initiation of aspirin therapy [7]. Serial imaging showed no progression of ischemic injury; however, the patient's level of consciousness remained impaired (GCS E1-2VTM2) throughout the hospitalization. Due to prolonged dependence on mechanical ventilation, a tracheostomy was performed. The patient was transferred to the Respiratory Care Center (RCC) for ventilator weaning.
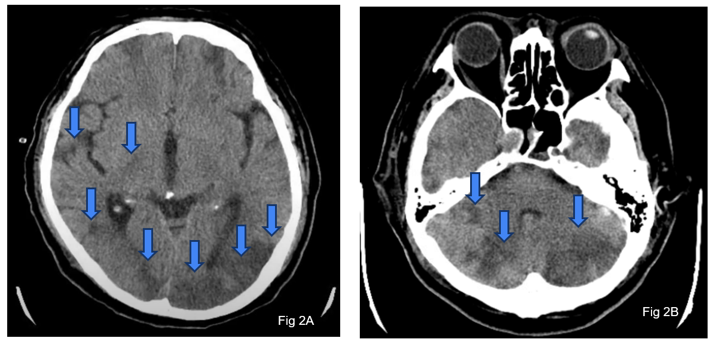
Figure 2: Postoperative brain computed tomography (CT) showed multiple supratentorial (Fig 2A) and infratentorial (Fig 2B) recent embolic infarcts
This case was complicated by extensive postoperative cerebral infarctions, despite limited changes in cerebral oximetry. Open surgery for Type B aortic dissection poses a stroke risk [1] even in the absence of carotid artery occlusion, with such events often identified during delayed awakening in the postoperative recovery phase. Compromises of cerebral blood flow (CBF) may be associated with surgical manipulations and the use of bypass, while hypothermia can influence brain neurophysiology. Previous studies have indicated that during hypothermia in the context of cardiopulmonary bypass (CPB), the Patient State Index (PSI) tends to decline while the Suppression Ratio (SR) increases; conversely, as body temperature normalizes, PSI increases and SR decreases [2]. Continuous monitoring of both cerebral oximetry and PSI may provide insights into postoperative cerebral dysfunction. In this case, despite relatively stable cerebral oximetry, notable changes in PSI were observed beginning after the transition of bypass, with no recovery by the end of the surgical procedure. It is likely that accidental embolization, rather than inadequate CBF, was the primary event responsible for the patient’s condition. Occlusion of cerebral arteries by air bubbles or dislodged atherosclerotic plaques[8] might have contributed to the patient’s development of diffuse cerebral ischemia. Once intraoperative strokes are suspected, diagnosis and the consequential managements could be started earlier. The management for air embolism includes preventing further air entry, stabilizing vital functions, placing the patient in the Trendelenburg position, administering 100% high-flow oxygen, and considering hyperbaric oxygen therapy (HBOT)[9]. For intraoperative stroke caused by atherosclerotic plaque dislodgement, the priority was to stabilize vital functions, after which intra-arterial mechanical thrombectomy might be considered as the treatment of choice, while tPA was limited by bleeding risk and heparin was not recommended [8].
Based on this experience, continuous electroencephalogram (EEG) monitoring could prove valuable on intraoperative embolic events and its recovery even in ICU [10]. Various neuromonitoring modalities, including electroencephalography [11,12], neurophysiological evoked potential measurements [13], transcranial Doppler, and near-infrared spectroscopy [3], have been reported to identify patients with acute large vessel occlusion [13]. Decreases in both the Patient State Index (PSI) and cerebral oximetry have also been observed in non-cardiac surgeries where cerebral blood flow (CBF) is compromised [14]. However, the dissociation between EEG signals and CBF may provide more details and facilitate earlier interventions.
We conclude that, in addition to cerebral hypoperfusion associated with compromised CBF, unintended neurophysiological injuries persist in cardiovascular surgeries. Simultaneous monitoring of both EEG and CBF may enhance early detection, as well as provide crucial insights for differential diagnosis and treatment.
During the preparation of this manuscript, we utilized OpenAI’s ChatGPT-4o (2024) to enhance the language and readability of the text. All content was subsequently reviewed and edited by the authors, who take full responsibility for the final version of the publication.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
