
Case Report | DOI: https://doi.org/10.31579/2690-4861/628
1 Department of Pediatric Anesthesia, Hôpitaux Pédiatriques de Nice CHU-Lenval, 57, avenue de la Californie, 06200 Nice, France.
2 Department of Pediatric Visceral Surgery, Hôpitaux Pédiatriques de Nice CHU-Lenval, 57, avenue de la Californie, 06200 Nice, France.
3 Department of Pediatric Otorhinolaryngology Surgery, Hôpitaux Pédiatriques de Nice CHU-Lenval, 57, avenue de la Californie, 06200 Nice, France.
4 Department of Pediatric Intensive Care Unit, Hôpitaux Pédiatriques de Nice CHU-Lenval, 57, avenue de la Californie, 06200 Nice, France.
*Corresponding Author: Charlotte Rémond, Department of Pediatric Anesthesia, Hôpitaux Pédiatriques de Nice CHU-Lenval, 57, avenue de la Californie, 06200 Nice, France.
Citation: Charlotte Rémond, Jean Bréaud, Sonanda Bailleux, Sébastien Bathélémy, François de la Brière, (2025), Sudden and Severe Hypoxia During Anesthesia Induction for A Neonatal Esophageal Atresia: Consider Accidental Esophageal Fistula Intubation, International Journal of Clinical Case Reports and Reviews, 23(3); DOI:10.31579/2690-4861/628
Copyright: © 2025, Charlotte Rémond. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 November 2024 | Accepted: 02 December 2024 | Published: 14 February 2025
Keywords: neonatal anesthesia; esophageal atresia; airway management; esophageal fistula; adverse event
A full-term neonate with type C esophageal atresia was scheduled in an emergency for surgical repair. During induction of anesthesia, the TEF was identified by a flexible tracheobronchoscopy. After endotracheal tube cuffed (ETT) insertion, ventilation was immediately impossible and led to severe hypoxia, requiring resuscitation maneuvers and an emergency percutaneous gastrostomy. The diagnosis of TEF intubation was made after ruling out the other typical causes of non-ventilation, such esophageal intubation, bronchospasm, hypovolemia, pneumothorax, obstructive secretions in ETT. After effective tracheal reintubation, the surgery proceeded normally. We did not observe any long-term sequelae.
TEF intubation during EA is a rare and poorly described event. We want to highlight this risk and the importance of having a multidisciplinary medical team present during anesthesia induction for neonatal EA surgical repair. To ensure optimal placement of ETT, this team should be able to perform real-time tracheal endoscopy, chest X-ray, or ultrasound.
Esophageal atresia (EA) is a rare, 1/3000 to 4500 births [1-4], early birth esophageal defect that occurs during pregnancy, due to an incomplete separation of the trachea and the esophagus. There are five types of esophageal atresia: type A, B, C, D, and E. The most frequent form (85%) is type C [1,4]: the upper part of the esophagus has a closed end and the lower part is attached to the trachea. EA is often associated with other neonatal defects in the digestive system, heart, kidneys, ribs or spinal column, up to the complete VACTERL syndrome (10% of EA) [1,4]. In half of the cases, the antenatal diagnosis uses non-specific ultrasound signs, like polyhydramnios [1,3]. Surgical repair, allowing the ligation of the TEF and the esophageal anastomosis should be done as soon as possible. Thoracoscopic procedure may enhance postoperative rehabilitation [1-3,5]. Perioperative management of EA with a TEF is always an anaesthetic challenge. Ventilation up to the ligation of the TEF without stomach dilatation is the main difficulty. In case of gastric dilation, a surgeon puncture can be performed in an emergency; some teams even perform a preventive preoperative gastrostomy. TEF intubation is a rare complication of EA procedure, poorly described in the literature, leading to a dramatic lack of ventilation and gastric dilation [4,6-9]. Awareness of this dramatic and underestimated adverse event enables the implementation of prevention and corrective measures for teams involved in neonatal EA management. We describe a clinical case reporting this incident whose diagnosis was late.
A three-day-old female had emergency surgery for type C esophageal atresia (EA) planned by thoracoscopy. The child was born full-term, 3480 g. The antenatal diagnosis of EA went unnoticed despite moderate polyhydramnios observed during the latest ultrasound. After birth, she had worsening feeding difficulties associated with hypersalivation respiratory distress with cyanosis, and significant bronchial congestion. The neonate received nasal oxygen and EA was diagnosed after a chest x-ray, showing a gastric tube coiled in the esophagus and gastric aeration (figure). Vertebral abnormalities were found, and a blood test and cardiac ultrasound were normal. Before anesthesia induction, the child’s weight was 2990 g, hemodynamic parameters were normal and Sp02 95% under 1 L/min nasal oxygen without CPAP. The preoperative flexible tracheoscopy in spontaneous ventilation under sevoflurane showed a large distal TEF near the carina. After an IV injection of 0.8μg sufentanil, 20 mg ketamine and 5 mg propofol, a 3.0 mm endotracheal cuffed tube (ETT) was easily inserted. We inserted the ETT to try to place its distal extremity beyond the fistula orifice. Immediately, we observed essential difficulties in mechanical ventilation leading to hypoxia (Sp02 55%) and bradycardia (60-80 bpm) with abdominal distension. We did not notice any capnogram and pulmonary auscultation was not helpful. External cardiac massage was started immediately, and the patient received 3 bolus of 50 µg adrenaline and a vascular filling of 2 g of albumin. The surgeon did a percutaneous gastric puncture with an IV cannula to deflate the gastric distension. The ETT position was checked again by laryngoscopy. We found no abnormal path of the tracheal tube or pneumothorax on the chest radioscopy done in the operating room. A tracheal suction probe did not retrieve any secretions in the ETT, but the probe was caught at its end. Therefore, the diagnosis was the accidental intubation of the esophageal fistula by the tracheal tube. We decided to remove the tube and performed another tracheal intubation. We immediately noticed an improvement in all the respiratory and hemodynamic parameters. Pulmonary auscultation was symmetrical. The entire episode lasted for few minutes, during which the resuscitation manoeuvres made it possible to maintain acceptable oxygenation and hemodynamic parameters. The surgery, initially planned by thoracoscopy, was performed by thoracotomy. The procedure was carried out without particular difficulties, and the infant was consequently transferred to the PICU. The mechanical ventilation was stopped on day 5; enteral alimentation was started by transanastomotic gastric tube on day 6. The girl was discharged from the hospital on day 26 with a good evolution without any neurologic sequelae. The 3-month follow-up was satisfactory regarding the digestive, pulmonary, and neurological aspects.
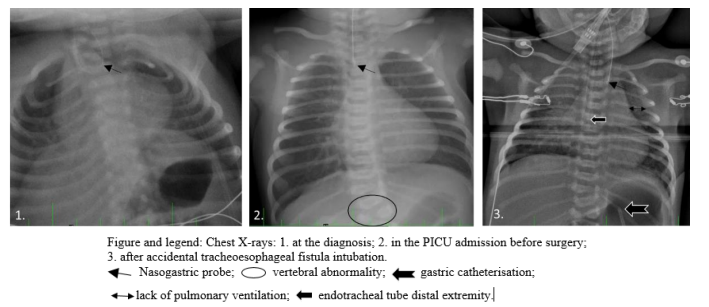
During EA surgery, accidental intubation of the tracheoesophageal fistula (TEF) has been sparsely described [4,6-9], leading in some cases to the death of the patient [7,8]. The diagnosis of EA with TEF is often delayed until after birth, with symptoms such as feeding difficulties, hypersalivation, as well as aspiration pneumonia [1,3]. EA diagnosis is confirmed when a blockage of the gastric tube in the end of the esophagus is visible on a chest X-ray (figure). The importance of identifying a TEF is currently well demonstrated in the literature [1-3,7,8,10,11]. The gold standard is a pre-operative bronchoscopy to determine the TEF characteristics (size, position, number), and to research potential tracheal abnormalities [2,3,7,10,12]. Recent studies have shown that only about half of EA cases benefit from a preoperative bronchoscopy [2,5,7]. A bronchoscopy study of 113 newborns with EA, by Holzki and al, described 67% of TEF cases above the carina, 22% within 1 cm of the carina and 11% at the carina or below it [12]. In this case, despite our experience, we initially did not consider the possibility of this adverse event leading to a delayed diagnosis of TEF intubation. We first eliminated esophageal intubation, bronchospasm, hypovolemia, pneumothorax, obstructive secretions in ETT, before considering this event. We couldn’t check the ETT placement with the bronchoscope because it was too wide, and direct laryngoscopy [8,11] and chest X-ray were not helpful (figure). Our pediatric hospital has no fiberscope thin enough to pass through a 3 mm ETT. The child’s weight might have allowed us to insert a 3.5 mm ETT, enabling us to perform a bronchoscopic control.
Various techniques have been described in the literature to prevent ventilation problems associated with TEF. The historical technique is to place distal extremity of the ETT below the orifice of the TEF: it must be placed up to the carina and then withdrawn, until obtention of symmetrical pulmonary auscultation [2-4,11]. The anesthetist can also rotate the ETT to close the TEF orifice with the bevel of the tube [2,11]. Another possibility described is to perform selective intubation in the left main bronchus until ligation of the TEF [11,13]. Still, there is always a potential risk of increasing ventilation difficulties and gas exchange disorders. Other teams have suggested using a Fogarty balloon catheter, or endobronchial blocker, to close the TEF [2-4,10,11,14]. This technique is uncommon due to implementation difficulties alongside or through the ETT and the risk of secondary displacement [3,11]. A recent article suggests performing a real-time ultrasound air visualization in the stomach to optimize the ETT placement [15]. In our case, the chest X-ray review could have suggested TEF intubation due to the absence of lung parenchyma ventilation and persistent gastric distension (Figure). The ventilation management of EA has been discussed for many years but there is still no firm consensus. This confirms the real difficulties encountered by medical teams involved in EA. The means of solving them depend on the experience of the various stakeholders (anesthetists, surgeons, otolaryngologists, neonatologists, gynecologists) and the use of all technical resources available. Due to EA’s rarity, the individual experience of each practitioner is minimal. This lack of experience leads to difficulties in setting up consensual protocols. These concerns were recently addressed by the European Reference Network on Rare Inherited and Congenital Anomalies (ERN-ICA), which published in 2020 the first international guidelines [16]. They advocate the need to manage at least 5 EA per year by specialized team, in order to develop optimal support [1]. But these recommendations rely on the uncontrollable random number of EA births. An investigation in 2012, showed that 67% of surgeons operate on 1 to 3 EA each year [2]. On the other hand, there is evidence that even skilled anesthetists may have difficulty intubating EA while excluding TEF [11,15].
While the ERN-ICA network mainly recommends diagnostic, surgical and postoperative measures for EA, only a few recommendations concerning anesthetic management and especially ventilation are given. Although the literature reports that only half of the teams perform preoperative fibroscopy in EA, there is a strong consensus on using systematic spontaneous ventilation tracheobronchoscopy before surgery. This exam allows us to characterize the fistula and may help to quantify the risk of TEF intubation when its orifice is large and near the carina. After intubation, additional measures such as real time ultrasound, chest X-ray, and ideally if possible bronchoscopic control of the ETT may also be performed [9,11,15]. The main limitation of this measure is the ability for teams to perform a bronchoscopy through an ETT with an internal diameter smaller than 3.5 mm. Another limitation is the rapid onset of hypoxia in case of TEF intubation, so only awareness of the TEF risk allows for a quick response by repositioning the ETT quickly.
Accidental intubation of the tracheoesophageal fistula during anesthesia induction for esophageal atresia is poorly described. This adverse event must be well known by anesthetic teams involved in esophageal atresia management. Awareness of this underestimated risk enables swift actions to prevent hypoxia in newborns with esophageal atresia.
This case presentation has been published with the written consent of the patient’s legal gardians
Charlotte Rémond: manuscript preparation, corresponding author
François de la Brière: manuscript preparation, reviewing.
Sonanda Bailleux; Jean Bréaud; Sébastien Barthélémy: reviewing.
The authors extend their special thanks for translation assistance to Françoise Garaud.
TEF- Tracheoesophageal Fistula
EA- Esophageal Atresia
ETT- Endotracheal Tube
IV- Intravenous
PICU- Pediatric Intensive Care Unit
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
