
Case Report | DOI: https://doi.org/10.31579/2692-9759/118
1 EHS Maouche Mohand Amokrane (Ex CNMS); faculty of medicine Benyoucef Ben khedda Algiers (ALGERIA).
2 Infant medical surgical clinic, Bou-ismail Algiers, faculty of medicine Algiers (ALGERIA).
*Corresponding Author: M. Abdelbaki, EHS Maouche Mohand Amokrane, Ben Youcef Ben Khedda Faculty of Medicine (Algeria).
Citation: : M.Abdelbaki, M.Touati, (2024), Successful Percutaneous Closure of Large Aorto-Pulmonary Window in a 3-Year-Old Girl Using Occluder A DO I 6/8: A Case Report, Cardiology Research and Reports. 6(1); DOI:10.31579/2692-9759/118
Copyright: © 2024, M. Abdelbaki. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 January 2024 | Accepted: 19 January 2024 | Published: 29 January 2024
Keywords: tricuspid insufficiency; echocardiography; mitral valve replacement; tricuspid plasty; mitral narrowing; operative mortality
This case report details the diagnosis, management, and successful percutaneous closure of a large aorto-pulmonary window with associated pulmonary hypertension in a 3-year-old female patient. The intervention involved the use of an Occluder ADO I 6/8 device. The report provides a comprehensive overview of echocardiographic findings and aortoangiography results, culminating in the therapeutic strategy and outcome
TThe aorto-pulmonary window is a rare congenital heart defect characterized by a communication between the ascending aorta and the pulmonary artery. This condition can lead to significant hemodynamic consequences, including pulmonary hypertension. Percutaneous closure has emerged as a viable alternative to surgical repair, particularly in pediatric patients.
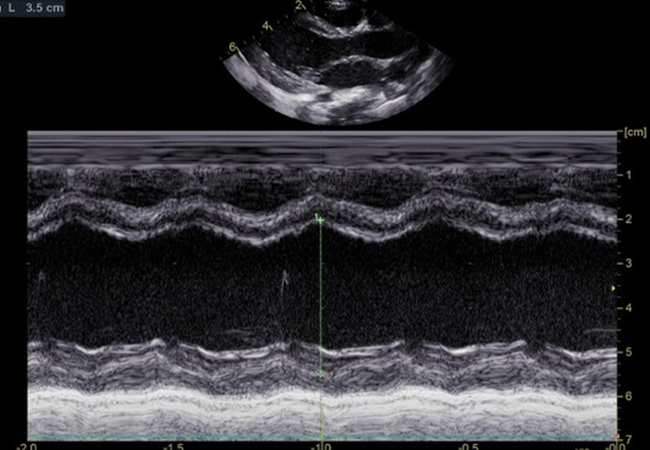
Transthoracic echocardiography showing in TM mode a Left ventriculare enlargement
The patient, a 3-year-old girl, presented with symptoms indicative of heart failure. Clinical examination and initial investigations suggested the presence of a large aorto-pulmonary window. Diagnostic Assessment: Echocardiography revealed :
Diagnostic Assessment: Echocardiography revealed :
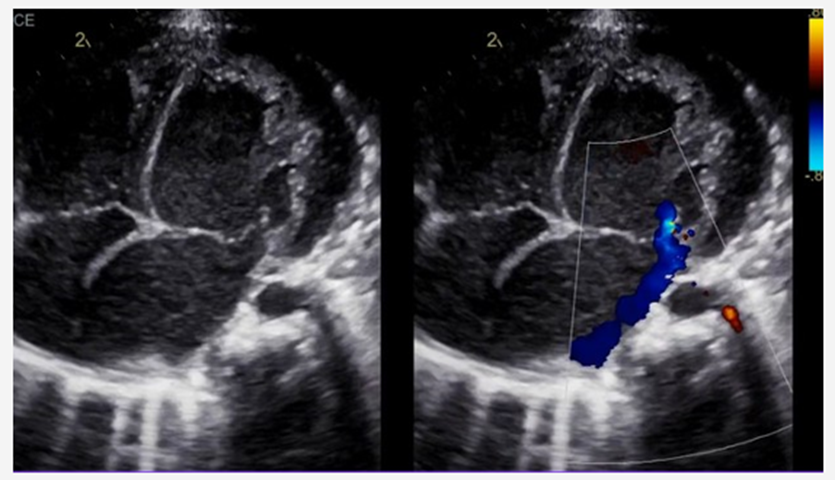
1. Identification and Characterization of the Aorto-Pulmonary Window:
A large aorto-pulmonary window was identified, measuring 5 mm in diameter.
The window was located between the ascending aorta and the main pulmonary artery.
Notably, the defect was situated at a considerable distance from the coronary arteries, reducing the risk of compromising coronary blood flow during intervention.
2. Assessment of Cardiac Chambers: Echocardiography showed signs of left ventricular overload. This was evidenced by:
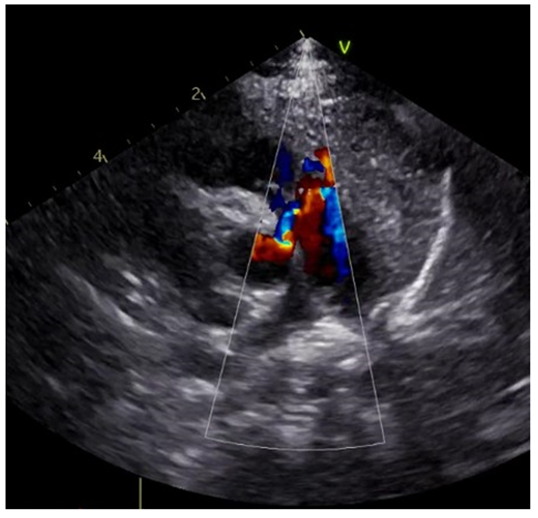
Transthoracic echocardiography showing the left to right shunt of the aorto-pulmonary window
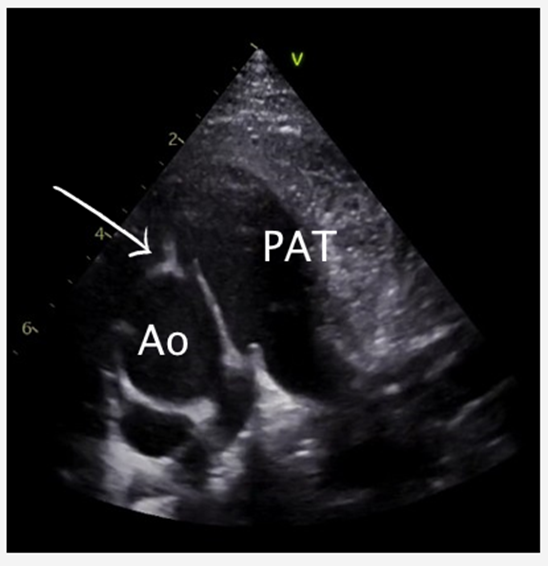
Transthoracic echocardiography showing the large aorto-pulmonary window Ao: Aorta, PAT: Pulmonary artery true
Transthoracic echocardiography showing left ventriculs enlargement
Mild to moderate enlargement of the left ventricle. Increased left ventricular end- diastolic and end-systolic dimensions. The presence of volume overload could be inferred from these findings, consistent with a significant left-to-right shunt. The left atrium was also mildly dilated, a common finding in conditions with increased pulmonary blood flow.
3. Shunt Dynamics:
A substantial left-to-right shunt was observed at the level of the aorto-pulmonary window. The shunt's impact on cardiac hemodynamics was apparent, contributing to the observed left ventricular overload.
4. Pulmonary Artery Pressure and Pulmonary Hypertension:
Pulmonary artery pressures were estimated to be elevated, suggesting mild to moderate pulmonary hypertension. This was likely a result of increased pulmonary blood flow due to the left- to-right shunt. PSE).
5. Evaluation of Valves and Great Arteries:
The atrioventricular and semilunar valves appeared structurally normal with no functional abnormalities. The aorta and pulmonary artery were evaluated, particularly focusing on their size and relationship to the defect.
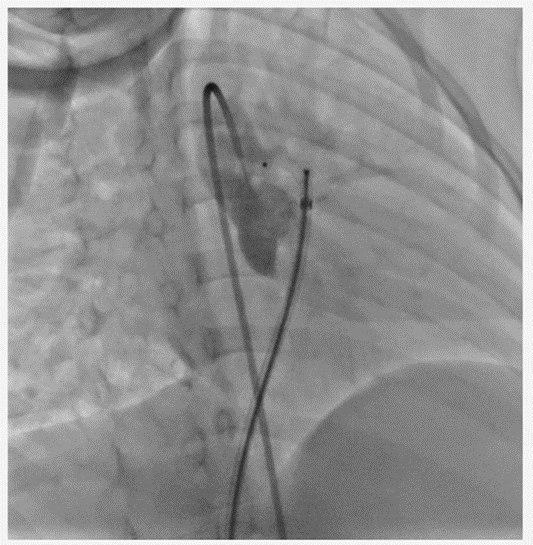
Procedure: a 6/8 PDA occluder was advanced abd deploide retrogadly from the pulmonary artery into the APW
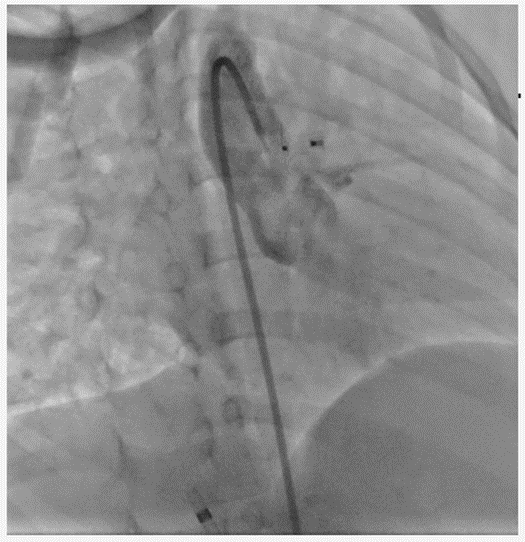
Final angiography with complete occlusion of the APW
1. Understanding Aorto-Pulmonary Window:
An aorto-pulmonary window is a rare congenital heart defect characterized by a communication between the aorta and the pulmonary artery. It can lead
to significant shunting of blood, resulting in volume overload on the left side of the heart and pulmonary hypertension.
2. Traditional Surgical Closure:
Historically, open-heart surgery was the standard approach for closing an aorto-pulmonary window.
Surgical closure involves cardiopulmonary bypass and direct suturing or patching of the defect.
While effective, surgery carries inherent risks like infection, bleeding, and the need for a longer recovery period, which can be particularly challenging in young children.
3. Advancements in Percutaneous Techniques:
With advancements in interventional cardiology, percutaneous techniques have become a viable alternative.
These procedures involve the use of catheters and closure devices, like the Occluder ADO II 6/8, inserted through the blood vessels, eliminating the need for open surgery.
4. Why Choose Percutaneous Closure?
Minimally Invasive:
Percutaneous closure is less invasive than traditional surgery. It avoids the need for a thoracotomy and cardiopulmonary bypass, reducing the risk of complications related to these procedures.
Shorter Recovery Time: The recovery period is generally shorter, and the hospital stay is reduced, which is significant for pediatric patients.
Less Traumatic: For a young child, a less invasive procedure can be less traumatic physically and psychologically.
Preservation of Cardiac
Structure: This approach preserves the integrity of the heart and chest structures, which can be beneficial in a growing child.
Technological Advancements:
The availability of specialized devices like the Occluder ADO II 6/8, designed for closing such defects, has improved the success rates of percutaneous procedures.
5. Consideration of Patient-Specific Factors:
The decision also depends on
the size and location of the defect, the patient's cardiac anatomy, and the presence of any additional cardiac anomalies.
In this case, the defect being 6 mm and away from the coronary arteries made it amenable to percutaneous closure.
The presence of left ventricular overload and mild to moderate pulmonary hypertension also warranted timely intervention, favoring a less invasive approach.
6. Risks and Limitations of Percutaneous Closure:
While percutaneous closure has many benefits, it's not devoid of risks. These include the potential for device embolization, residual shunts, or damage to adjacent cardiac structures.
The expertise of the interventional team and the availability of appropriate device sizes are crucial factors.
7. Long-Term Outcomes and Follow-Up: Long-term outcomes of percutaneous closure of aorto- pulmonary windows are generally favorable, but regular follow-up is necessary to monitor for any complications or residual defects.
Highlights the successful outcome of the intervention, with resolution of the patient's symptoms and normalization of pulmonary pressures. This case contributes to the growing body of evidence supporting the efficacy and safety of percutaneous closure techniques in pediatric patients with aorto-pulmonary window.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
