
Case Report | DOI: https://doi.org/10.31579/2768-2757/080
1 Department of Plastic, Reconstructive and Aesthetic Surgery, Private Hospital of Büyükşehir, Konya, Turkey
2 Department of Plastic, Reconstructive and Aesthetic Surgery, Necmettin Erbakan University Meram Faculty of Medicine, Konya, Turkey
*Corresponding Author: Moath Zuhour, Department of Plastic, Reconstructive and Aesthetic Surgery, Private Hospital of Büyükşehir, Konya, Turkey.
Citation: Zuhour M., Baycar Z., Dadacı M., İnce B., (2023), Successful Multiple Finger Replantation; Procedure and Considerations, Journal of Clinical Surgery and Research, 4(3); DOI:10.31579/2768-2757/080
Copyright: © 2023, Moath Zuhour. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 April 2023 | Accepted: 28 April 2023 | Published: 10 May 2023
Keywords: fds transfer; finger amputation; replantation; total amputation
Multiple finger amputations require challenging surgeries and special approach. At least, the thumb and middle finger should be replanted to maintain minimal hand functions. Technically, multiple amputations are more difficult than single finger amputation and distal amputations are more difficult than proximal ones. Herein, we present a case of four finger amputation. All fingers were successfully replanted. The patient required a long period of physical rehabilitation. The patient underwent another operation because of the extensor lag of the four fingers. In the second operation a four-tail FDS transfer to the lateral bands was performed. The rehabilitation process is still ongoing.
Finger amputations are one of the most difficult operations of plastic surgery that require special equipment and skills. The degree of difficulty varies according to some factors such as the level of amputation, number of fingers involved, trauma etiology, age of the patient and comorbid diseases. Technically, multiple amputations are more difficult than single finger amputation and distal amputations are more difficult than proximal ones.
While total amputations refer to the complete separation of the finger from the body, revascularization refers to partial amputations in which the finger remains attached to the body with some tissue (1). 7-29% of patients who apply to the emergency department apply due to hand injury (2). In hand trauma, the fingers are mostly affected, with the marginal fingers (1 and 5) being more common (3). Although these traumas are mostly seen in young men, the age of incidence in both genders is 26-28 years for men and 29.31 years for women (4).
Indications for replantation include thumb amputation, multiple finger amputations, trans-metacarpal amputations and any amputation in children (5). Many goals should be considered when performing replantation surgery, such as preserving adequate finger length, maintaining protective sensation, keeping functional recovery at the highest level and preventing joint contractures [6].
In this paper, we aimed to present the operation and postoperative rehabilitation process of a case applied with 4 finger amputations as a result of work accident.
The patient applied after work accident with total amputation of 2nd ,3rd ,4th and 5th fingers of the right hand at the level of MCP joint and a dislocation of the 1st finger at IP joint with a fracture in the proximal phalanx of the same finger (Figure 1). The patient was taken immediately to the operation room. First, exploration and necrotic tissue debridement were done. Then, arteries, nerves and veins in the amputated fingers were marked. When the wound site of the right hand was explored, it was observed that the palmar arch was totally cut and the digital arteries were detached right after the branching point from the arch. It was also observed that the common digital nerves going to the 4th and 5th fingers and 3rd and 4th fingers were defective, and the other nerves were totally cut.

Figure 1: Preoperative view of the amputated fingers.
K-wires was delivered through the amputated joints first and then toward the metacarpal bones (retrograde fashion) (Figure 2). The right wrist was entered with appropriate incisions from the volar aspect, and the muscle groups were exposed. The proximal ends of the cut FDP tendons were passed through the carpal tunnel. The FDS tendons were not repaired because of potential adhesions and to keep them for reconstruction procedures that may be needed later. The FDP tendons were repaired by modified Kessler technique. After repairing the arterial ends for anastomosis; the ulnar digital artery of the 5th finger, the common digital artery to the 4th and 5th fingers, the common digital artery to 3rd and 4th fingers, the common digital artery to 2nd and 3rd fingers and the superficial palmar arch were repaired using an 8-0 Dylon suture. The anastomoses were checked for blood flow and all of them were working well. The radial digital nerve of the 2nd finger, the common digital nerve to the 2nd and 3rd fingers and the ulnar digital nerve of the 5th finger were repaired.
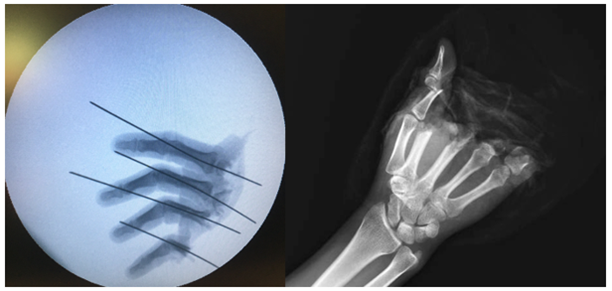
Figure 2: K-wires inserted into the amputated part.
After the bleeding control, the skin incisions were sutured (Figure 3, A). The hand was placed on a plaster splint and the procedure was terminated. On the postoperative 6th month, the patient underwent another operation due to the extensor lag of the IP joints (Figure 3, B). The FDS tendons (4-tail FDS transfer) was transferred to the lateral bands of the four fingers. The patient is still under physical therapy until the time of writing this paper.
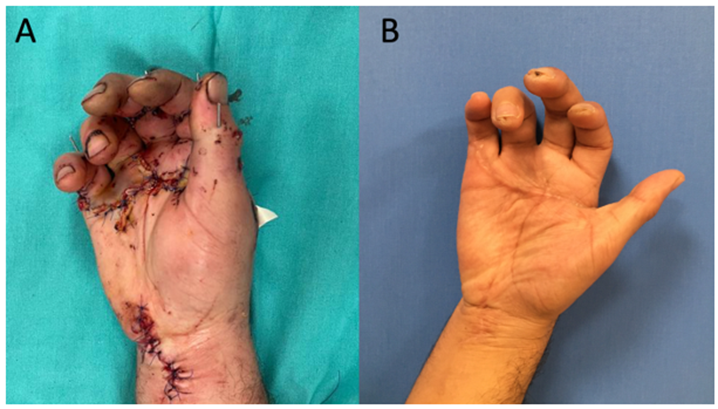
Figure 3: A: immediate postoperative view, B: late postoperative view showing the extensor lag of the fingers.
The thumb constitutes 40% of the functions of the hand. Grasping and opposing movements cannot be performed without the thumb (7). However, in order for the thumb to perform these functions, there must be at least one more finger at the opposite direction to meet it. In order to provide maximum function in multiple finger amputations, the replantation priority order proceeds as follows; thumb, middle finger, index finger, ring finger and little finger (8). In our case, only the thumb was preserved with bone fractures, while all the other fingers were amputated as an en-bloc. We replanted all of the fingers to achieve maximum function. Blood flow returned without any problems. During replantation surgery, Priority should be given to vessels and nerves after necrotic tissues and foreign materials are debrided. The neurovascular structures are first marked in the amputated parts, and then the recipient vessels are explored. This is followed by bone fixation and tendon repair. The purpose of this is to stabilize the bones after the anastomosis is done so that the anastomosis is not damaged during the fixation. After these procedures, anastomoses are made and checked for blood flow (8). If there is soft tissue loss, it is repaired with local flaps, interpolation flaps or free flaps (9). Since the incision in this case was relatively clean, no further debridement was required. However, because the trauma was in zone 3, it was very close to the joints and required careful bone fixation. According to our observation, retrograde bone fixation is easier in such a region. In order to achieve this, first retrograde entry is made through the joints on the amputated side and the wire is advanced until it exits the PIP joint. Then the wire is sent back to the metacarpal bones. The ultimate goal of replantation is a painless limb, good soft tissue coverage and a functional hand. When the acute recovery process is over, physical therapy exercises should be started. While the replanted fingers are in the splint, the patient should learn the passive and active exercises of the healthy fingers (10). In addition, intact joints that are not included in the fixation should not be forgotten. As an example, in our case, MCP and PIP joints were fixated. But the DIP joints were kept free and the patient was taught how to move them. When bone healing was confirmed by direct radiographs, K wires were removed and active and passive exercises were initiated. In such complicated cases, postoperatively, the patients should not be left to the control of physical therapy only. The surgeon who performed the operation should also follow-up the patient at frequent intervals.
Multiple finger amputations require challenging surgeries and special approach. At least, the thumb and middle finger should be replanted to maintain minimal hand functions. With good planning and analysis of the existing situation, all of the fingers can be salvaged without any loss. The patient should be informed before and after the surgery, and the importance of physical therapy should be emphasized frequently.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
