
Research Article | DOI: https://doi.org/10.31579/2693-4779/186
1 Department of Medicine, Lincoln Medical Center/Weill Cornell Medicine, New York, NY, USA
2 Department of Medicine Washington University in St. Louis, St. Louis, MO, USA
3 Department of Medicine, SIU School of Medicine, Springfield, IL, USA
4 Department of Medicine, Jacobi Medical Center, New York, NY
5 Department of Medicine, University of Missouri-Kansas City, MO, USA
6 Department of Gastroenterology & Hepatology, Lincoln Medical Center, New York, NY, USA
7 Inflammatory Bowel Disease Center at New York University Langone Health, Division of Gastroenterology and Hepatology, New York, NY, USA
Grant & Financial Support: A.S.F.: NIH (R03AG078927-01), ACG Career Development Award, Crohn’s and Colitis Foundation CRA.
*Corresponding Author: Yassine Kilani, Chief Resident, Department of Medicine Lincoln Medical Center/Weill Cornell Medicine Bronx, New York, NY, USA 234 East 149th Street New York, NY 10451.
Citation: Yassine Kilani, Mohammad Aldiabat, Chee Yao Lim, Fatima Kamal SA, Priscila C. Puelo, et al, (2024), Subtypes of VenousThromboembolism in Inflammatory Bowel Disease: A Nationwide Assessment, Clinical Research and Clinical Trials, 9(3); DOI:10.31579/2693-4779/186
Copyright: © 2024, Yassine Kilani. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 31 January 2024 | Accepted: 23 February 2024 | Published: 05 March 2024
Keywords: IBD; ulcerative colitis; Crohn’s disease; venous thromboembolism
Background
Data detailing the risk of Venous Thromboembolism (VTE) subtypes among individuals with inflammatory bowel disease (IBD) remain limited. We looked to assess the odds of VTE subtypes among hospitalized individuals with IBD as compared to those without IBD.
Materials & Methods
Using the Nationwide Inpatient Sample database, we applied a multivariable regression analysis to compare the odds of primary VTE-related hospitalizations among individuals with and without IBD from 2016 to 2020, including deep venous thrombosis (DVT), pulmonary embolism (PE), portal vein thrombosis (PVT), Budd Chiari syndrome (BCS), renal vein thrombosis (RVT), and cerebral venous sinus thrombosis (CVST).
Results
Overall, there were 15,565 primary VTE-related hospitalizations among individuals with IBD, as compared to 1,449,164 among individuals without IBD. Having IBD increased the odds for DVT (aOR = 1.34, 95%CI: 1.25–1.43), PVT (aOR = 3.16, 95%CI: 2.65–3.76), and CVST (aOR=1.45, 95%CI: 1.05–2.00), without significant increase in the odds of a PE, BCS, or RVT. Further, individuals with ulcerative colitis (UC) were at a higher risk for the majority of VTE-subtypes as compared to those with Crohn’s disease (CD). Among individuals with a VTE-related hospitalization, the presence of IBD was not associated with increased mortality (aOR = 0.77, 95%CI: 0.40–1.50), but was associated with an increased length of stay (CD – 4.8 days, UC – 5.3 days, without IBD – 4.3 days, p<0.01).
Conclusions
Clinicians should retain a high index of suspicion when evaluating VTE-related symptoms among individuals with IBD, as the presence of IBD confers a higher risk of DVT, PVT and CVST related-hospitalizations, and longer stays as compared to individuals without IBD.
Inflammatory bowel disease (IBD), which includes Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic immune-mediated disease of the gastrointestinal tract and is widely prevalent. [1] In 2017, more than 6.8 million individuals globally had IBD, corresponding to a prevalence rate of 464 per 100,000 individuals in the U.S. alone. [1] As this number continues to rise, the number of individuals who will experience both disease and treatment-related adverse outcomes will also increase.
Venous thromboembolism (VTE) is of particular interest, as it carries high morbidity and mortality, and occurs more commonly among individuals with IBD. Further, with the aging of the IBD patient population [2], coupled with the growing use of JAK-inhibitors, the number of individuals with IBD who experience a VTE event may continue to rise. Recent data have even shown that rates of VTE among hospitalized patients with IBD are increasing over the past 2 decades, from 192 to 295 cases per 10,000 hospitalizations. [3]
Despite the increasing number of VTE events among individuals with IBD, there are scant data exploring its different subtypes, as the majority of studies have only focused on the incidence of deep venous thrombosis (DVT) and pulmonary embolism (PE). However, individuals with IBD have also been shown to be at increased risk for portal vein thrombosis (PVT), Budd Chiari syndrome (BCS), renal vein thrombosis (RVT), and cerebral venous sinus thrombosis (CVST). [4-12] A recent retrospective analysis of the Nationwide Inpatient Sample (NIS) database analyzed a subset of these conditions, finding that individuals with both UC and CD had higher odds of DVT, PE, PVT and mesenteric ischemia as compared to the general population. [13] However, 1) the inclusion of all individuals with VTE rather than those with a primary diagnosis of VTE may capture a percentage of individuals who develop a VTE while hospitalized, possibly influencing the odds observed 2) only a few subtypes of VTE were captured including DVT, PE, and PVT, and 3) the analysis was restricted to only one year (2016). Additionally, the finding that individuals with both UC and CD are at higher risk for VTE subtypes has not been confirmed in prior studies, including meta-analyses. [3, 5, 14, 15]
Therefore, in order to add to what is known, we conducted a large database study from 2016 to 2020 exploring differential odds of a primary VTE- related hospitalization among individuals with IBD as compared to those without IBD, including comparisons of CD and UC. Additionally, we explored differences in inpatient mortality, and length of stay for VTE- related hospitalizations among individuals with and without IBD.
Data source:
Using the National Inpatient Sample (NIS), we conducted a study of individuals hospitalized from 2016 to 2020. The NIS database was developed for the Healthcare Cost Utilization Project and is currently the largest public all-payer database in the U.S. [16] It provides U.S. regional and national estimates of inpatient hospital admissions. The NIS represents a 20% sample of hospitalizations from all non-federal acute care hospitals [17], compiled annually by multiple statewide organizations [18], and includes uniform collection of demographic and administrative data on healthcare utilization, cost, quality, and outcomes. [19] The NIS data is selected from a stratified systematic random sample of hospitalizations and is weighted to calculate national estimates for the entire U.S. [19] Since October 2015, the NIS uses International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10 CM) codes, which were used in our analysis. Data from the NIS is de-identified and publicly available, and is therefore exempt from Institutional Review Board review. According to the Data User Agreement for HCUP, cell sizes <11>Study population:
Individuals with and without IBD ≥18 years old who were hospitalized during 2016-2020 were included in the analysis. A VTE-associated hospitalization was defined as a hospitalization in which VTE was listed as a primary diagnosis. In order to capture this, we used ICD-10 CM codes for DVT, PE [20, 21], PVT, BCS [21], RVT [22], and CVST (Supplemental
Table 1). [23, 24] The presence of IBD was defined with a secondary diagnosis code for IBD, including both CD and/or UC. [3] Individuals with a diagnosis code for both UC and CD were included in our primary analysis (comparing individuals with IBD vs. without IBD), but excluded when assessing individual IBD subtypes (UC and CD).
Patient and hospital characteristics:
We captured data available within the NIS on age, sex, body mass index (BMI; ≤19.9, 20 to 24.9, 25-29.9, ≥30 kg/m2), race (non-Hispanic White, non-Hispanic Black, Hispanic, Other), primary insurance (Medicare, Medicaid, Private Insurance, Self-pay), income quartile, and hospital characteristics (region, teaching status, bed size). [15] Comorbidities were also captured as part of the Charlson comorbidity index, and categorized as 0, 1, 2, ≥ 3. [25]
Comorbid Thrombotic Conditions:
We additionally captured comorbid thrombotic conditions that can increase the risk of VTEs [26], including a prior history of VTE [3], smoking status (current or prior) [27], active malignancy [24], congestive heart failure [28], oral contraception (OCP) use, pregnancy [29], limited mobility [30], thrombophilia (including prothrombin excess, protein C deficiency, and other thrombophilia) [3], hyperhomocysteinemia [31], and concomitant immune-mediated diseases, including rheumatoid arthritis (RA), systemic lupus erythematous (SLE), and systemic sclerosis (SS; Supplemental Table 1).
| PATHOLOGY | ICD-10-CM code |
| Crohn’s disease | K50.X3 |
| Ulcerative colitis | K51.X3 |
| Deep vein thrombosis (DVT) | I80.1X, I80.2X,I82.2X, I82.4X, I82.6X, I82.890, I82.90, I82.A1, I82.B1, I82.C1, O22.3, O22.5, O22.9,O87.119,20 |
| Pulmonary embolism (PE) | I26, O88.2X19,20 |
| Portal vein thrombosis (PVT) | I8120 |
| Budd Chiarisyndrome (BCS) | I82.020 |
| Renal vein thrombosis (RVT) | I82.321 |
| Cerebral veinsinus thrombosis (CVST) | I63.6, I67.6, O22.5X, O87.3, G08.X22,23 |
| VTE history | Z86.7X, Z87.8913 |
| Nicotine dependence | F17.X27 |
| Malignancy (current) | CX, D0.X,D1.X, D3.X, D4.X24 |
| Clostridioides difficile infection | A047.X3 |
| Congestive heart failure | I09.81, I50.x, I51.81, I97.130, I97.131, I11.0, I13.0,I13.2, R57.028 |
| Chronic oral contraceptive use (OCP) | Z92.0, Z79.329 |
| Pregnancy | O.X |
| Bed confinement | Z74.0130 |
| Nephrotic syndrome | N04.X33 |
Thrombophilia (Prothrombin excess, Protein C deficiency, other thrombophilia) | D68.5X, D68.6X3 |
| Hyperhomocysteinemia | E72.1131 |
| Auto-immune diseases (SLE,RA, systemic sclerosis) | M05, M06, M32.X, M34.X32 |
Supplemental Table 1. International Classification of Diseases, Tenth Revision, ClinicalModification (ICD-10-CM) codes for the primary and secondary diagnoses.
[32]We additionally adjusted for C. difficile infection, which has been associated with VTE in patients with IBD, and as a specific confounder for RVT, we also included nephrotic syndrome. [3, 33]
Outcomes:
Our primary outcome was the odds of a primary DVT, PE, PVT, RVT, or BCS-related hospitalization among patients with UC and CD as compared to those without IBD. Secondary outcomes including inpatient mortality, length of stay, and total healthcare expenditures.
Statistical Analysis:
Baseline characteristics were compared using a t-test for continuous variables and a Chi-square test for categorical variables. A multivariable
logistic regression analysis was then applied to estimate the odds of a primary VTE-related hospitalization, as well as its subtypes, among patients both with and without IBD. Additionally, odds ratios (ORs) with 95% confidence intervals (95%CI) were also calculated to assess overall VTE- related mortality, as well as length of stay, among individuals with and without IBD. Analysis of weighted samples was completed using Stata/SE® Version 17.0 software (StataCorp, Texas, USA).
Patient Characteristics:
Overall, from 2016-2020 there were a total of 148,687,525 hospitalizations, with 1,182,655 (0.8%) corresponding to individuals diagnosed with IBD (Table 1).


CD: Crohn’s disease;UC: Ulcerative colitis; OCP: Oral Contraceptive pills; CHF: CongestiveHeart Failure; AI: Autoimmune; RA: Rheumatoid arthritis,SLE: Systemic Lupus Erythematous; SS: Systemic sclerosis
Table 1: Baseline characteristics when evaluating primaryVTE-related hospitalizations among individuals with and withoutIBD.
More specifically, 737,290 (0.5%) hospitalizations were associated with a diagnosis of CD whereas 440,495 (0.3%) were associated with a diagnosis of UC. A total of 4,870 discharges were associated with both diagnoses of CD and UC.Individuals hospitalized with IBD were more likely to identify as non- Hispanic White (81% in IBD vs. 67% in non-IBD, p<0>Table 1).
When evaluating IBD subtypes, individuals with CD were younger (mean age: 55 years ± 0.1 years in CD vs. 60 years ± 0.1 years in UC), and more likely to identify as Non-Hispanic Black (11% in CD vs. 9% in UC, p<0>Table 2).


CD: Crohn’s disease;UC: Ulcerative colitis; OCP: Oral Contraceptive pills; CHF: CongestiveHeart Failure; AI: Autoimmune; RA: Rheumatoid arthritis,SLE: Systemic Lupus Erythematous; SS: Systemic sclerosis
Table 2.Baseline characteristics when evaluating primary VTE-related hospitalizations associated with Crohn’s diseasevs.ulcerative colitis.
Prevalence of VTESubtypes:
Overall, 1,464,729 (1.0%) of all hospitalizations were associated with a primary ICD-code for VTE. On univariable logistic regression, individuals with IBD (1.3%) were more likely to have a primary VTE-related hospitalization as compared to individuals without IBD (1.0%, p<0 xss=removed>When considering all individual subtypes of VTE, we found that the presence of IBD significantly increased the odds of a primary DVT (aOR =
1.34, 95%CI: 1.25–1.43), PVT (aOR = 3.16, 95%CI: 2.65–3.76), and CVST
(aOR=1.45, 95%CI: 1.05–2.00). However, there was no significant increase in the odds of a primary PE (aOR = 1.05, 95%CI: 0.99–1.12), BCS (aOR = 1.63, 95%CI: 0.51–5.13), or RVT-related (aOR = 1.75, 95%CI: 0.63–4.84)
hospitalization (Figure 1a). This, however, was driven largely by individuals with CD who were not at increased odds of having a primary BCS (aOR = 2.55, 95%CI: 0.81–8.05), RVT (aOR = 0.91, 95%CI: 0.16–5.29), or PE (aOR
= 0.94, 95%CI: 0.87–1.01; Figure 1b). In contrast individuals with UC were at higher odds of having both a primary PE (aOR = 1.25, 95%CI: 1.15–1.36) and RVT (aOR = 3.47, 95%CI: 1.10–10.95), though there were no cases of BCS observed in this subgroup (Figure 1c).
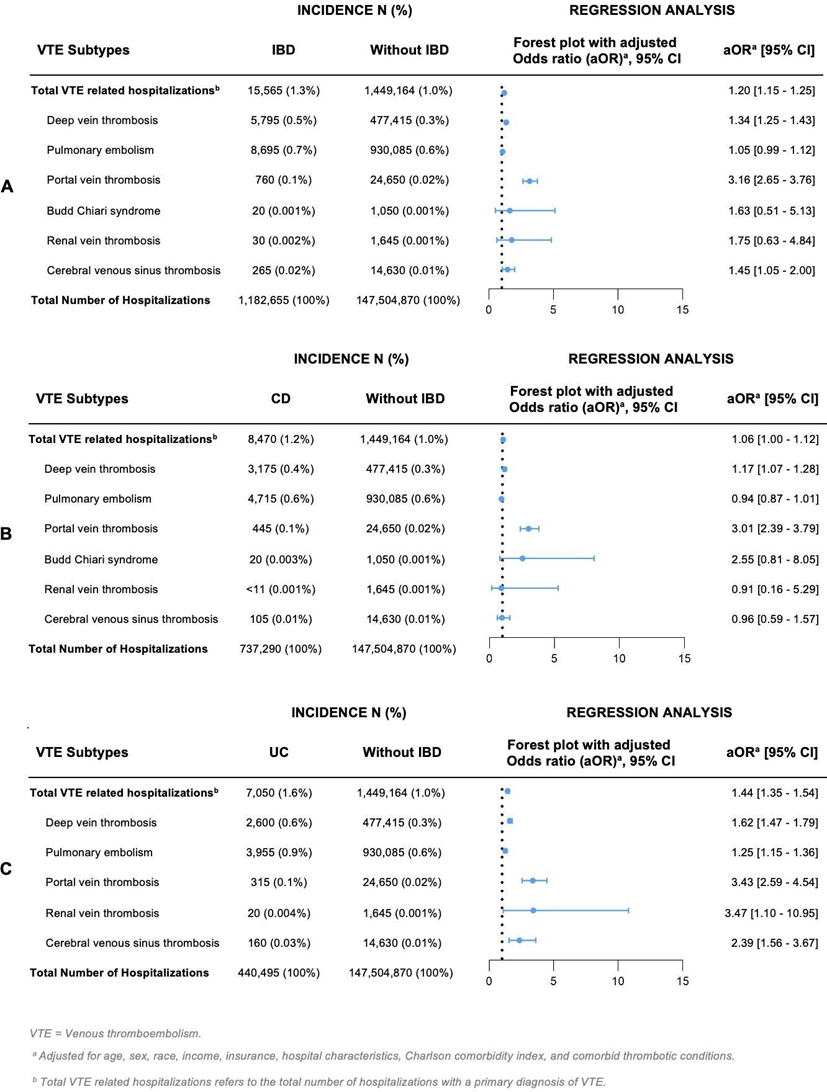
Figure 1: Prevalence and odds of venousthromboembolic (VTE) eventsamong individuals with and withoutIBD. IBD is associated with increased odds of VTE, including DVT, PVT, and CVST compared to patients without IBD, and no significant change in the odds of PE (figure 1-A). While both CD (figure 1-B) and UC (figure 1-C) are associated with increased odds of DVT and PVT, only UC increases the odds of PE, RVT, and CVST related hospitalizations (figure 1-C).
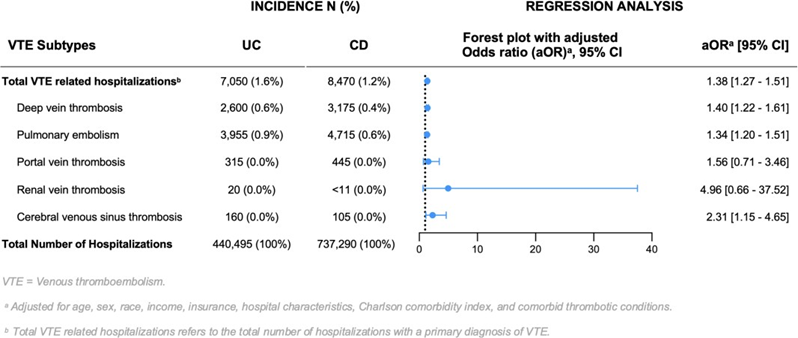
When comparing individuals with UC vs. CD, the presence of UC was associated with a higher overall VTE risk (aOR = 1.38, 95%CI: 1.27–1.51), as well as a higher risk of DVT (aOR = 1.40, 95%CI: 1.22–1.61), PE (aOR = 1.34, 95%CI: 1.20–1.51), and CVST (aOR = 2.31, 95%CI: 1.15–4.65;
Supplemental Figure1).
Mortality and Healthcare ResourceUtilization:
Among individuals with a VTE-related hospitalization, the presenceof IBD was not associated with increased mortality (aOR = 0.77, 95%CI: 0.40 – 1.50), but was associated with an increased length of stay (CD – 4.8 days, UC – 5.3 days, without IBD – 4.3 days, p<0>


*Adjusted for age, race, BMI, comorbidity index,income, insurance status,hospital characteristics, and dayof admission.
NB: Variables (Reference values): Age (18-44), Sex (Male), Race (non-Hispanic White), BMI (19-25 kg/m2), Income quartile (1st-25th percentile), Hospital size (Small), Hospital region (Northeast), Hospital teaching status (Non-teaching), Insurance status (Medicare), Day of admission (Weekday), Charlson comorbidity index (0).
Supplemental Table 2. Multivariate logistic regression analysis assessing predictors of among individuals admitted with a primary ICD code for venous thromboembolism.
In this nationwide study we found a 20% increase in the overall odds of VTE- related hospitalizations among individuals with IBD compared to those without IBD. Notably, both UC and CD were associated with higher odds of DVT and PVT, while only UC exhibited elevated risks for PE, RVT, and CVST. Additionally, the presence of IBD does not lead to a significant difference in mortality within VTE-related hospitalizations, but is associated with significantly longer lengths of stay as compared to individuals without IBD.
VTE poses a significant risk of both morbidity and mortality [34], and there is growing concern that this will continue to increase over the next decade. One contributing factor to this potential increase is the expanding use of JAK-inhibitors, coupled with the aging of the IBD patient population. [2] Further, although prior studies have shown an elevated risk of VTE among individuals with IBD, data have largely focused on the presence of DVT and PE. [4, 35, 36, 37] More specifically, these data have shown that IBD confers a 1.3 to 4-fold increase in the odds of DVT and PE. [4, 5, 15, 35, 36, 38-40] In our study, we observed similar results, as we found increased odds of DVT-related hospitalizations for individuals with both CD and UC. However, when evaluating primary PE-related hospitalizations, we found similar odds among individuals with IBD as compared to those without IBD. Further, when stratifying by subtype of IBD, we can see that this finding may largely be driven by the presence of CD, as individuals with UC had higher odds for a primary PE-related hospitalization. This is consistent with a prior meta-analysis showing no difference in rates of PE between individuals with and without IBD [41], though prior studies have shown UC to carry a higher risk of PE as compared to CD. [13, 42]
When evaluating PVT, RVT and CVST, we found similar findings. Notably, odds of a primary hospitalization for PVT were higher among individuals with both CD and UC, while hospitalization for RVT and CVST were higher only among individuals with UC. Although the pathogenesis of VTE in IBD is still incompletely understood [43, 44], prior data have shown higher levels of pro-coagulant factors (Factor V and Factor VIII) among individuals with UC as compared to individuals with CD, which may potentially contribute to the findings observed. Further, higher levels of plasminogen, a protein responsible for clot fibrinolysis, were also observed among individuals with
CD as compared to those with UC, offering an additional explanation as to
the increased risk of VTE seen among individuals with UC. [45] Last, upadacitinib, a JAK-inhibitor recently approved for treating moderate to severe IBD, has also been shown to increase the risk of VTE among individuals with UC but not CD. [46, 47]
These findings are of particular importance, as despite the higher VTE risk observed among individuals with UC, they are often less likely to receive pharmacologic VTE prophylaxis while hospitalized. [48] This is likely due to the presence of hematochezia, which can deter providers from using pharmacologic VTE prophylaxis, despite data showing it to be both safe and effective in this population. [48, 49] Further educational efforts should therefore focus on highlighting the increased risk of VTE among individuals with UC, as well as the safety and efficacy of pharmacologic prophylaxis in this population.
Additionally, although VTEs are known to increase the risk of overall mortality, there are limited data exploring whether VTEs disproportionality increase the risk for mortality among individuals with IBD as compared to those without IBD. [3, 28] Reassuringly, in our study, we did not observe that the presence of IBD significantly increased the odds of VTE related mortality, though further data are needed to confirm this. We did, however, find that VTE-related hospitalizations were associated with longer lengths of stays and healthcare related costs among individuals with IBD as compared to those without IBD. This is in accordance with prior data [14], and underscores the need to focus on preventative VTE efforts.
Our study has several strengths. This is the first study that comprehensively analyzes the risk of several VTE subtypes among individuals with IBD, including disease-based comparisons between UC and CD. Moreover, using the NIS we were able to capture 148 million hospitalizations across the U.S., ensuring adequate power and generalizability of our results. Furthermore, uniform collection of variables included in the NIS helps to mitigate potential referral and reporting biases, which are commonly encountered in single- center studies and voluntary registries. Moreover, the inclusion of individuals with a primary VTE-related hospitalization allows us to exclude individuals who may have developed a VTE during hospitalization, thereby minimizing potential confounders.
There are also methodological biases inherent to our study design. First is the reliance on ICD codes which cannot be verified by manual review, however, ICD-10 CM codes for DVT and PE have been shown to have high sensitivity for VTE related hospitalizations, though no study has evaluated this specifically within the NIS database. [21] Moreover, although data pertaining to medication use (e.g., corticosteroids), disease activity, recent hospital admission or surgery is not available in the NIS database, we adjusted for additional VTE-related risk factors such as smoking, OCP use, and comorbid thrombotic conditions (e.g., cancer, thrombophilia). Last, it should be noted that one individual can account for several admissions, though the likelihood of presenting with multiple primary VTE -related hospitalizations over the five-year study period are rare.
In sum, individuals with IBD have a higher risk for DVT, PVT, and CVST, without significant increase in the risk of PE, BCS, and RVT. Further, on subgroup analysis, we observed that individuals with UC appear to be at higher risk for the majority of VTE subtypes as compared to individuals with CD. Additionally, having IBD did not confer additional mortality risk among those with VTE-related hospitalizations, however individuals with IBD had on average longer lengths of stay. These findings hold significant clinical implications, as the identification of individuals with IBD who are at a heightened risk for specific VTE-related subtypes carries substantial clinical significance. This recognition not only informs future evaluations for VTE in the IBD patient population, but also underscores the necessity for heightened efforts in the prevention of VTE manifestations among hospitalized patients with IBD. Last, a strategic focus on post-discharge and outpatient prophylaxis initiatives may be warranted among those individuals with IBD who are at highest risk for VTE.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
