
Research Article | DOI: https://doi.org/10.31579/2641-0419/383
1Department of Surgery, Cardiac Surgery, University of North Carolina at Chapel Hill.
2Department of Medicine, Cardiology, University of North Carolina at Chapel Hill.
*Corresponding Author: Aurelie Merlo, MD Assistant Professor 3040 Burnett Womack 1 Dental Circle Drive Chapel Hill, NC 27514.
Citation: Panagiotis Tasoudis, William Mostertz, Mirnela Byku, Aurelie Merlo (2024), Substance Use is Associated with Increased Readmissions, but not in-hospital morbidity or long-term survival after left ventricular assist device implantation, J Clinical Cardiology and Cardiovascular Interventions, 7(7); DOI: 10.31579/2641-0419/383
Copyright: © 2024, Aurelie Merlo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 May 2024 | Accepted: 17 June 2024 | Published: 25 June 2024
Keywords: LVAD; substance use; transplant
Aim: Patients with active substance use are not eligible for heart transplantation and often undergo left ventricular assist device (LVAD) implantation. We define substance use as use of a substance that precludes transplant such as tobacco products, marijuana, illicit drug use, and excessive alcohol use. The purpose of this study is to describe and compare outcomes in patients with active or recent substance use undergoing LVAD implantation to those who do not use substances.
Materials and Methods: We performed a single-center retrospective cohort study of all patients undergoing HeartMate3 implantation during the period from 2017 to 2023. The patients were divided into those who have a current or recent history of substance use (SUD) and those who do not. The primary outcome was survival. And the secondary outcome measures included in-hospital outcomes and readmission rate. The Kaplan Meier method was used to calculate overall survival. An unadjusted multivariate cox proportion hazards model was used to assess differences in survival. Adjusted Poisson regression models were used to determine differences in readmission rates.
Results: 177 patients were included, with 55 (31%) of patients using substances at the time of implantation (mainly tobacco products and marijuana). Patients using substances were younger (p<0.001) and had a higher body mass index (p=0.012). Survival (HR 1.51, CI (0.84-2.71)) and in-hospital outcomes were not significantly different between groups (stroke, bleeding, renal failure, days in intensive care, length of stay, mortality). When adjusting for age and INTERMACS score, patients with SUD had significantly higher rates of readmissions compared to those without SUD (IRR: 1.23, 95% CI:1.02-1.50, p=0.035).
Conclusions: In conclusion, in a large single-center retrospective cohort study, patients who are using substances at the time of LVAD implantation have the same survival and in-hospital complication rates as patients who are not using substances. When adjusting for age and INTERMACS score, patients who use substances have a higher readmission rate than patients who are not using substances.
Active and recent substance use precludes patients from being listed for heart transplantation. The International Society of Heart and Lung Transplant recommends six months of abstinence from tobacco products and other substances such as marijuana, heroin, heavy alcohol use, and cocaine before being listed [1]. These recommendations are based on data showing that patients who are actively using substances have worse survival after heat transplant [2] and ongoing substance use is associated with non-adherence with medical therapy after transplantation [3]. To maximize survival after transplantation and to promote organ stewardship, transplant centers help patients who use substances demonstrate six months of abstinence prior to being listed, as this duration of pre-transplant abstinence is associated with staying substance free post-transplant [3]. Unfortunately, many patients are too sick to wait six months to demonstrate abstinence and need advanced therapies sooner. These patients often undergo left ventricular assist device (LVAD) implantation.
While, up until recently, survival after LVAD implantation did not compare to that of a heart transplant, more recent data is promising. Five-year survival (survival to transplant, recovery, or LVAD support free of debilitating stroke or reoperation for pump exchange) in the MOMENTUM 3 trial was 54% [4]. Five-year survival for heart transplant recipients is approximately 70% [5]. As patients who use substances undergo LVAD implantation live longer with their LVAD, the focus shifts towards improving outcomes other than survival, such as the ability to achieve abstinence, readmissions, the incidence of driveline infections, etc. As we continue to learn what we can achieve in terms of outcomes for all LVAD patients, so too are we learning how sub-groups of patients fare. The purpose of this study is to retrospectively describe and compare outcomes in patients who use substances undergoing LVAD implantation to those undergoing LVAD implantation who do not use substances.
This study is a single-center retrospective cohort study that includes all HeartMate3 implantations at our institution from January 2017 to June 2023. We excluded patients who underwent LVAD implantation and were listed for transplant at the time of implantation (bridge to transplant). The patients were divided into two groups – those with an active or recent history of substance use (SUD group) and those without (no SUD group).
Substance use was defined as the use of a substance precluding listing for transplantation based on our transplant centre listing criteria. This includes tobacco products, marijuana, other illicit drugs, and substantial alcohol use within six months of implantation. The primary outcome measure was overall survival. Secondary outcome measures included implant hospitalization outcomes such as survival at index hospitalization, incidence of bleeding, stroke, renal failure, days spent in the intensive care unit, and length of stay, but also longer-term outcomes such as number of readmissions and ongoing substance use at one year. Readmissions were defined as readmissions at the implanting hospital system. Median follow-up for this study was 616 [IQR 302, 1366] days. This study was conducted following our institution’s IRB (IRB # 20-0642).
Statistical analysis
Patient baseline characteristics and clinical outcomes data are expressed as frequencies with corresponding percentages for categorical variables and as median [first quartile, third quartile] for continuous data. The baseline patient characteristics were compared among the two groups using the χ2 test for categorical and the t-test for continuous variables.
The Kaplan–Meier method calculates and plots the overall survival (OS). An unadjusted multivariate Cox proportional hazards model was utilized to assess if there is any difference in OS between the SUD and no SUD groups. We used adjusted Poisson regression models to determine our readmission and reoperation outcomes. We adjusted our models accounting for the patient’s age and INTERMACS score. We used the incidence rate ratio (IRR) to express the differences in the mean number of outcomes observed in two comparative groups. An IRR >1 means that the SUD group's outcome result is most observed. Data was analysed using STATA IC 17.0 (StataCorp LLC, College Station, Texas).
A total of 199 patients underwent HeartMate3 insertion at our institution, and 177 were not listed for transplant at the time of implantation (implanted as “destination therapy”). Of those patients, 55 (31%) of them were using substances at the time of implantation (SUD group). Of the patients using substances, 33 (60%) of them were unable to be listed for transplantation solely based on substance use. Figure 1 depicts the breakdown of substance type in this study’s cohort. The majority of patients were using tobacco products and marijuana. 19 (35%) patients were using more than one substance and 16 of those patients were using either a tobacco product or marijuana. Baseline characteristics between groups are depicted in Table 1. Patients who were using substances were younger, with a median age of 54 years [45, 60] compared to 63 [56, 62] (p<0 p=0.012). >Table 1. Baseline Demographics All patients No substance use Substance Use N = 177 N= 122 N=55 N or median % or IQR N or median % or IQR N or median % or IQR p-value Age (years) 60 51-68 63 56-62 54 45-60 <0> Female Sex 43 24.3 30 24.6 13 23.6 0.526 Race African American 87 49.2 57 46.7 30 54.6 0.54 White 83 46.9 60 49.2 23 41.8 Other 7 3.9 5 4.1 2 3.6 BMI (kg/m2) 28 24-33 27 22-30 28 25-35 0.012 INTERMACS 1-2 54 31 32 26 22 40 0.262 INTERMACS 3 97 55 72 59 25 46 INTERMACS 4-6 24 14 17 14 7 13 Ischemic CM 73 41 53 43 20 36 0.467 CPB time (min) 70 50-93 70.5 48-97 66 51-90 0.1 Abbreviations. BMI, body mass index; CM, cardiomyopathy; CPB, cardiopulmonary bypass time; IQR, interquartile range; std. dev, standard deviation
Table 1. Baseline Demographics and Clinical Characteristics of 177 Patients Undergoing LVAD Implantation as Destination Therapy Divided by Those Who Use Substances and Those Who Do Not
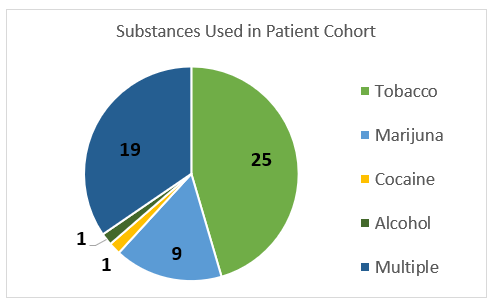
Figure 1: Pie Chart Illustrating Which Substances Were Being Used in a Cohort of 177 Patients Being Evaluated for LVAD Insertion as Destination Therapy
Figure 2 shows the Kaplan–Meier curves depicting overall survival for both groups. Overall survival was not significantly different between patients who use substances and those who do not (HR 1.51, CI (0.84-2.71). In terms of secondary outcomes, in-hospital mortality did not differ between groups and neither did incidence of in-hospital complications (Table 2).
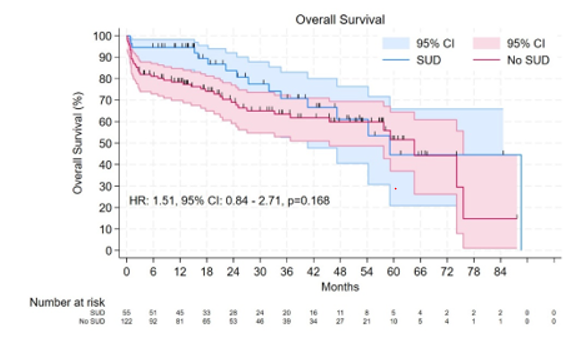
Figure 2. Overall Survival Curves Using Kaplan Meier Method of Patients who Underwent LVAD Implantation as Destination Therapy By Those Who Use Substances and Those Who Do Not
| Table 2. Postoperative Complications | |||||||
| All patients | No substance use Substance use | p-value | |||||
| N=177 | N=122 | N=55 | |||||
| N or mean | % or IQR | N or mean | % or IQR | N or mean | % or IQR | ||
| Stroke | 4 | 2.26 | 4 | 3.28 | 0 | 0 | 0.312 |
| Bleeding | 15 | 8.47 | 9 | 7.38 | 6 | 10.91 | 0.56 |
| Renal failure | 39 | 22.03 | 32 | 26.23 | 7 | 12.73 | 0.051 |
| Hours in ICU | 281.5 | 191, 413 | 234 | 175, 392 | 287 | 199, 451 | 0.396 |
| Length of Hospital Stay | 30 | 18, 42 | 31 | 17, 45 | 27 | 20, 39 | 0.677 |
| Death during implant hospitalization | 22 | 12.43 | 19 | 15.57 | 3 | 5.45 | 0.083 |
| Abbreviations. ICU, intensive care unit; IQR, interquartile range | |||||||
Table 2. Postoperative Outcomes of 177 Patients Undergoing LVAD Implantation as Destination Therapy Divided by Those Who Use Substances and Those Who Do Not
In our unadjusted model, no differences were noted between SUD and no SUD groups regarding readmissions (IRR: 1.04, 95% CI:0.87-1.26, p=0.648). However, when our model was adjusted for patients’ age and INTERMACS score, patients with SUD were found to have significantly higher rates of readmissions compared to those with no SUD (IRR: 1.23, 95% CI:1.02-1.50, p=0.035). Of note, of the 47 patients in the SUD group who were alive at one year, the majority were continuing to use substances (N = 31, 66%).
In this retrospective single-center cohort study, we show that patients with active or recent use of substances that preclude them from immediate transplant listing at the time of LVAD implantation have similar survival compared to patients who do not. However, we observed a higher hospital readmission rate in this group when adjusted for age and INTERMACS score. This study provides hope for patients who are not able to receive transplant therapy promptly, showing that LVAD implantation is an acceptable, indeed the only, alternative, so long as attention is paid to long-term and programmatic support to help with the increased burden of readmissions. The findings of this study are in keeping with recent data from the Interagency Registry for Mechanically Assisted Circulatory Support [6], which also showed no mortality differences in patients who use illicit drugs or have a history of alcohol abuse. However, that study did show that after adjusting for other covariates, a history of alcohol abuse or illicit drug use was significantly associated with the combined end point of increased device malfunction, device-related infection, or all-cause hospitalization. They also noted that the postoperative quality of life in patients with a history of alcohol abuse or illicit drug use after LVAD implantation was lower than in patients who did not use those substances at 12 and 18 months. Our data has shown no difference in mortality in these patients, but did study a different population as it also included patients using tobacco products. A subgroup analysis may show similar findings to the INTERMACS study. In contrast, our results differ, from similar studies conducted a decade ago that came from case series [7] and for a long time served as the basis for not offering LVAD therapy to these patients. Our study expands upon the more recent results by underlying readmission rates and ongoing substance use rates.
This study does not answer the question of why patients who use substances at the time of implantation are more likely to be readmitted. One hypothesis is that readmissions may be driven by infectious complications such as driveline infections. However, this was not fully captured in our study and will be the source of future research for our group. Additionally, this study does not fully capture social determinants of health and psychosocial risk factors. It is likely not to detect factors that contribute to ongoing substance use, social distress, and readmissions. Race, sex, and specific social determinants of health can influence disparities with completing an advanced therapies evaluation and undergoing LVAD implantation [8], as well as affecting outcomes following surgery [9]. What we can derive from this study is that for a centre to adequately care for these patients in the long term, a solid multidisciplinary care team, including social workers, psychologists, psychiatrists, and LVAD coordinators, is essential for success.
It was disappointing to see the high rate of ongoing substance use at one year (66%), suggesting, even more, can be done with counselling and support for these patients. It is possible that for some patients, six months of substance abstinence before heart transplantation alone is unrealistic or insufficient. That decision likely needs to be individualized for each patient [10]. This study does show that LVAD implantation is an acceptable, indeed the only, alternative for patients who are having difficulty achieving the six-month abstinence period.
While this isn’t the central topic of our study, it is essential to acknowledge the shifting landscape of marijuana use and transplantation. Marijuana is legal in several states now, suggesting its use is more acceptable, similar to alcohol and tobacco, rather than an illegal substance. ISHLT task forces encourage the development of guidelines based on data and not subjective judgement [11]. 2023 Guidelines reference studies showing marijuana is linked to decreased adherence, increased rate of infections, and problems with drug interference, and they currently recommend continuing to use a six-month period of abstinence from cannabis prior to listing for transplantation [11]. With only data from a single center, it was not possible to evaluate differences in outcomes by substance type. Still, it would be interesting to see how outcomes may differ based on substance use, especially with the majority of patients using either tobacco or marijuana. We are currently working on creating a multi-institutional registry to answer this question.
The limitations of this study are those inherent to a single-center retrospective study. The results of this study might not be generalizable to other centers due to specifics inherent to our LVAD patient population. In addition, due to the small sample size, further sub-analysis was not able to be performed, and we cannot say if a particular substance type or substance use with a specific comorbidity was associated with worse outcomes. Finally, the definition of substance use, especially for alcohol use was subjective. However, these patients were evaluated by a multidisciplinary team, including social workers and therapists who were trained in psychosocial risk assessment of patients undergoing evaluation for advanced therapies. Only one patient was excluded from listing for transplantation solely based on the use of alcohol. The remainder of patients had substance use documented by drug screen or nicotine test, in addition to patient interviews with our social work team. This analysis grouped all substances that precluded listing for transplant together. It may be true that demographic and clinical characteristics are different between patients who use illegal substances compared to legal substances such as tobacco. Nonetheless, we grouped these patient populations as we felt it to be helpful to evaluate patients who are excluded from transplant candidacy. Furthermore, subdividing into smaller groups would limit our interpretation of differences observed.
In conclusion, in a large single-center retrospective cohort study, patients using substances at the time of LVAD implantation had the same survival rates but higher hospital readmission rates compared to patients who were not using substances. With the right resources, centers can provide the benefits of LVAD therapy to these patients and expect similar outcomes to patients not using substances.
CI – confidence interval
INTERMACS - The Interagency Registry for Mechanically Assisted Circulatory Support
LVAD – left ventricular assist device
OS – overall survival
SUD – substance use
All authors declare that they have no conflicts of interest regarding the content in this manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
