
Case Report | DOI: https://doi.org/DOI:10.31579/2690-4861/675
1 Division of Anatomical Pathology, Department of Pathology, University of Cape Town, South Africa.
2 National Health Laboratory Service, Groote Schuur Hospital, Cape Town, South Africa.
*Corresponding Author: Jackie Chokoe Maluleke, Division of Anatomical Pathology, Department of Pathology, University of Cape Town, South Africa.
Citation: Johannes Enslin, Raymond Chimatara, Jackie C. Maluleke, (2025), Subcutaneous Collision Tumour-Malignant Melanoma and Small Lymphocytic Lymphoma/ Chronic Lymphocytic Leukemia (SLL/ CLL)- A Diagnostic Pitfall, International Journal of Clinical Case Reports and Reviews, 23(5); DOI:10.31579/2690-4861/675
Copyright: © 2025, Jackie Chokoe Maluleke. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 January 2025 | Accepted: 12 February 2025 | Published: 28 February 2025
Keywords: chronic lymphocytic leukemia; small lymphocytic lymphoma; malignant melanoma
(Cutaneous collision tumours involving two malignant neoplasms are exceedingly rare. We report a case of chronic lymphocytic leukaemia (CLL)/small lymphocytic lymphoma and malignant melanoma (MM) occurring synchronously in a subcutaneous location.
The synchronous occurrence of two distinct tumours in the same anatomical site is a rare but well-described phenomenon, referred to as a collision tumour1. In the skin, collision tumours in which both components are malignant are even more rare2, and most reported cases involve a combination of two primary malignant cutaneous neoplasms. Furthermore, associations between cutaneous malignancies and lymphoproliferative disorders are well described, including the specific association between malignant melanoma and non-Hodgkin’s lymphomas. However, to our knowledge, less than ten cases of cutaneous melanoma and lymphoma occurring as a collision tumour have previously been reported.
A 64-year-old female with a history of hypertension, chronic lymphocytic leukaemia/small lymphocytic lymphoma (CLL/SLL), and a previously excised cutaneous melanoma presented to a regional hospital with two subcutaneous nodules in the left forearm. She had no prior history of chemotherapy or radiotherapy.
We received two excision biopsies, measuring 15 x 10 x 5 mm and 10 x 8 x 5 mm, respectively. Microscopy of both fragments revealed two juxtaposed pathological processes: a melanocytic tumor, and an adjacent monomorphic small lymphocytic proliferation (figure 1).
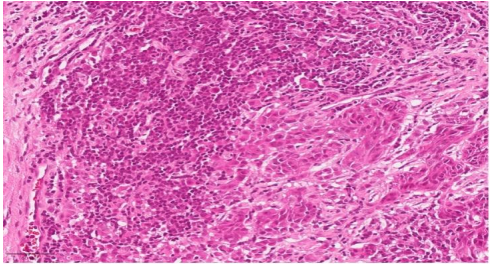
Figure 1: The histopathology image shows the collision tumour comprising the malignant melanoma with epithelioid morphology and abundant eosinophilic cytoplasm. There is interspersed small lymphocytic proliferation which is interspersed within the melanoma.
The melanocytic tumor comprised irregular nests and fascicles of epithelioid and spindle shaped cells, with abundant eosinophilic, non-pigmented cytoplasm, markedly pleomorphic nuclei with prominent nucleoli, and brisk mitotic activity (figure 2).
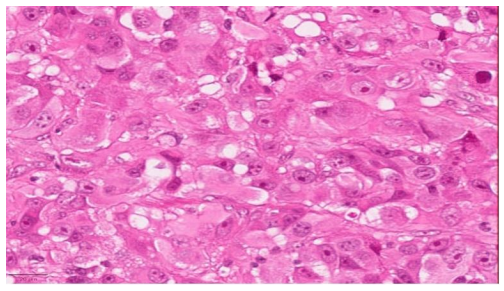
Figure 2: At high power the malignant melanoma shows irregular nests and sheets of malignant cells with epithelioid morphology with vesicular chromatin and prominent nucleoli.
Lesional tissue extended to multiple resection margins. The monomorphic small lymphocytic proliferation demonstrated no unique morphologic features (figure 3).
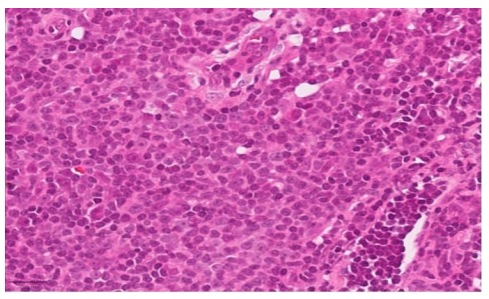
Figure 3: small lymphocytic proliferation is seen here with absence of proliferation centres.
Proliferation centers were not appreciated. Represented surrounding soft tissue demonstrated prominent associated fibrosis and severe chronic inflammation. Immunohistochemistry confirmed a recurrent melanoma, with strong positivity for HMB45 (figure 4) and S100 (figure 5), as well as an adjacent neoplastic B-cell proliferation compatible with chronic lymphocytic leukemia/small lymphocytic lymphoma. The melanoma additionally stained for SOX-10 immunohistochemical stain. The neoplastic lymphoid cells diffusely expressed CD20 (figure 6), CD5 (figure 7), CD 23, BCL2 and demonstrated negativity for CD3 and Cyclin D1. BCL2 was additionally noted to be diffusely positive in both the melanocytic and small lymphocytic components. The Ki-67 proliferative index was approximately 50% in both neoplasms. Molecular PCR studies for B-cell gene rearrangement additionally confirmed monoclonality in both the IgH and IgK genes in the small lymphocytic lymphoma/chronic lymphocytic leukaemia.
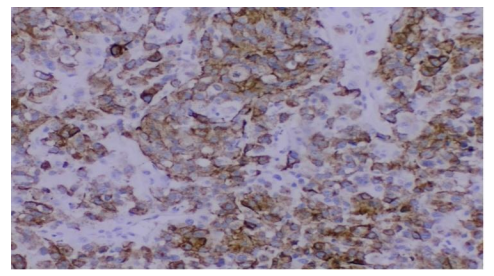
Figure 4: immunohistochemical stain showing melanoma component staining for HMB-45
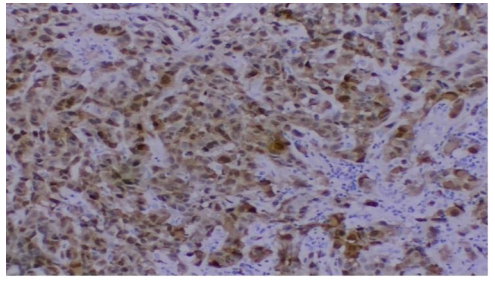
Figure 5: immunohistochemical stains showing melanoma staining for S100.
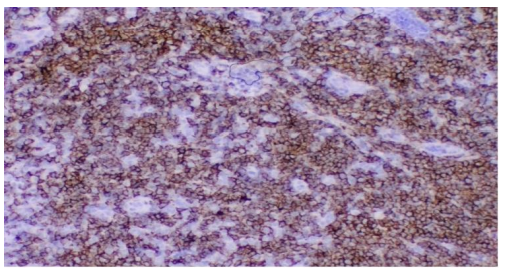
Figure 6: immunohistochemical stains showing the CLL/ SLL staining for CD20.
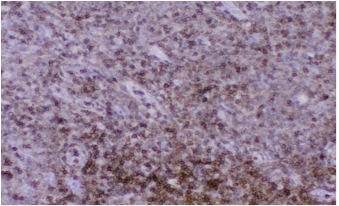
Figure 7: the CLL/ SLL component stains for CD5.
A diagnosis of a cutaneous collision tumour comprising recurrent malignant melanoma and small lymphocytic lymphoma/chronic lymphoid leukaemia (SLL/CLL) was made. The patient subsequently underwent a wide local excision and sentinel lymph node biopsy for the recurrent malignant melanoma; with reported findings including: a Breslow thickness of 19.1mm, an inadequate deep resection margin of 0.1mm, noted large vessel lymphovascular and perineural invasion, and an epicondylar sentinel lymph node positive for metastatic melanoma. No further information on the patient’s clinical course could be obtained from the referring hospital.
Synchronously diagnosed cutaneous collision tumours involving two malignant neoplasms of which one is a lymphoma are exceedingly rare. Although in our reported case the patient was known with SLL/CLL, as well as a previous malignant melanoma, given the increasing evidence of
association between melanoma and non-Hodgkin’s lymphomas (NHL), this synchronous recurrence as a collision tumour is of academic interest. The prognostic implications of a dual diagnosis and importance of the histologic detection of both components are self-explanatory.
Previously published reports of collision tumours involving malignant melanoma and non-Hodgkin’s lymphomas in intranodal locations include cases of follicular, mantle cell and, diffuse large B-cell lymphoma [3,4,5], and one case of chronic lymphocytic leukaemia (CLL)/small lymphocytic lymphoma [6]. Previously reported cases in extra-nodal locations include only two reports: [1] a case of spindle cell melanoma and SLL/CLL occurring in multiple sites [7], and [2] a case of melanoma and mantle cell lymphoma occurring in the skin 8.
Evidence of an association between cutaneous lymphoma and malignant melanoma has been reported since the year 19609. In some cohorts, an increased risk of NHL in cutaneous melanoma survivors of as high as 43%, and an increased risk of cutaneous melanoma in NHL survivors as high as 75% was demonstrated [10]. Clear though as this association is, the underlying basis is not well understood, with possible contributing factors including: previous mutagenic treatments (chemotherapy, radiotherapy, PUVA photochemotherapy11), occupational risk factors, immunosuppression (AIDS, organ transplant recipients) and alterations in common genetic pathways – particularly those involving p16/CDKN2A [10,12]. In addition to its direct mutagenic effects, the chronic inflammatory and immunosuppressive effects of ultraviolet radiation exposure may also be implicated, but are as of yet poorly understood [13, 14].
In conclusion, we report a case of a rare collision tumour diagnosed in the same biopsy specimen, comprising amelanotic malignant melanoma and chronic lymphocytic leukaemia (CLL)/small lymphocytic lymphoma. Besides the prognostic implications and hence importance of successfully detecting both an aggressive and an indolent neoplasm, the possible aetiologic links are of growing academic interest.
The authors declare no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
