
Research Article | DOI: https://doi.org/10.31579/2693-7247/114
1 Associate professor, Department of Pharmacology, GSL Medical College, Rajahmundry, India.
2 Associate professor, Department of Pharmacology, Apollo medical college- Chittoor, Andra Pradesh, India.
*Corresponding Author: M Yatish Byndoor, Associate professor, Department of Pharmacology, Apollo medical college- Chittoor, Andra Pradesh, India.
Citation: Tamilisetti Vidya Sagar and Yatish Byndoor, (2023). Study to Investigate Socioeconomic, Demographic and Health Related Risk Factors among Women with Gestational Diabetes Mellitus in a Tertiary Care Health Centre in South India. J. Pharmaceutics and Pharmacology Research, 6(1); DOI:10.31579/2693-7247/114
Copyright: © 2023 M Yatish Byndoor, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 November 2022 | Accepted: 30 December 2022 | Published: 25 January 2023
Keywords: macrosomia; polycystic ovarian disease; prepregnancy body mass index; hypertension
Objective
To investigate socioeconomic and demographic risk factors in gestational diabetes mellitus and to evaluate health related risk factors like age and pre-pregnancy BMI in a tertiary care centre in south India.
Materials and methods
Hospital based non-interventional observational study, BMI and blood pressure are considered as health related variables, age, level of education, residence are considered as socioeconomic and demographic variables. Family history of diabetes, GDM, previous history of macrosomia, history of PCOD, pregnancy order are considered as obstetric variables in this study. Information about age, height, weight, gestational age, family history was collected. Body mass index was calculated using pre pregnancy weight. Gestational age was calculated from last menstrual period. GDM was diagnosed in accordance with International Association of Diabetes and Pregnancy Study Group recommendations, data was analysed using descriptive methods
Results
Out of 42 women diagnosed with GDM, 10 (23%) were above 35 years, 20 (47%) were between 25 to 35 years, 12 (28%) were below 25 years of age. GDM is detected in 39 out of 52 obese women (75%), 80 % of GDM women had diabetes in their family compared to non GDM women. Out of 42 women diagnosed with GDM, only 5 women completed bachelor’s degree, out of 42 women diagnosed with GDM, 15 were of urban residence, this shows access to better medical resources can reduce incidence of gestational diabetes. 52% of women with GDM had polycystic ovarian disease.70% of GDM women developed hypertension in pregnancy.
Conclusion
Our study shows variability of occurrence of GDM across demographic groups and geography in India. Obesity prior to pregnancy, older age, history of PCOD, were correlated with an increased risk of GDM. This suggests that, pregnancy is better planned before age of 25 years and pre-pregnancy weight reduction might lower risk of developing GDM.
Gestational diabetes mellitus (GDM) is defined as glucose intolerance with onset or first recognition during pregnancy (1) and was first recognised in 1823 (2).
World Health Organization (WHO) 1999 criteria defined GDM by fasting plasma glucose level greater 126 mg/dl or 2-h plasma glucose levels after 75 g oral glucose tolerance test greater than 140 mg/dl. Indian criteria for GDM use only 2-h criteria (DIPSI) (3, 4). Prevalence of GDM,when using WHO 1999 criteria range between 1 and 14% in different populations (5, 6, 7).
International Association of Diabetes and Pregnancy Study Groups (IADPSG) has proposed to lower FPG for diagnosis of GDM, namely to fasting blood sugar >92 mg/dl while using 2-h PG threshold of >153 mg/dl (8).WHO recently decided to adopt IADPSG criteria, hereafter named WHO 2013 criteria (9).
GDM is associated with maternal complications like preeclampsia, infection, polyhydramnios, caesarean section and fetal problems like sudden intra uterine demise, macrosomia, birth trauma, hypoglycemia, hyperbilirubinemia and respiratory distress syndrome. Not only women with GDM, their offspring’s also have increased risk for developing impaired glucose tolerance, type 2 diabetes and obesity in future i.e. two generations are at risk. (10, 11)
There is wide variability in reported prevalence estimates for GDM in India, varying from less than 4%to nearly 18%. (12, 13) Despite a government mandate to screen all pregnant women for GDM, to date there has been incomplete implementation and uptake of screening programs. (14)
To our knowledge, there has been no comprehensive national assessment of GDM and socioeconomic, demographic, and geographic factors associated with it. In this study, we investigated prevalence, socioeconomic, demographic and tried to evaluate various risk factors associated with GDM like age, family history, pre-pregnancy BMI in a tertiary care centre in south India.
The present study is a non-interventional observational study and does not involve any procedures / tests. It was conducted in a tertiary care hospital; diagnosis and management were decided by obstetrician in charge. Once consultation by obstetrician was over, pregnant women were screened for study criteria, written informed consent was taken from all participants, who fulfilled study criteria. A written permission has been obtained from Institutional Ethics Committee for the conduct of the study. A total of 100 pregnant women of 24-28 weeks of gestation were included in the study. Study period is from August 2021 to August 2022. Known diabetic women (pre gestational)/diagnosed having GDM before 24 weeks and pregnant women with any comorbidities were excluded from the study. Information about age, height, weight, gestational age, family history of diabetes, obstetric history, past history was collected. Body mass index was calculated using pre pregnancy weight. Gestational age was calculated from last menstrual period, confirmed or corrected by ultrasound gestational age. GDM was diagnosed in accordance with International Association of Diabetes and Pregnancy Study Group recommendation(IADPSG) for GDM based on 75 g 2-h OGTT: a fasting glucose >92 mg/dl, or 1-h result >180 mg/dl, or 2-h result >153 mg/dl) (8).
Body mass index (BMI) and blood pressure are considered as health related variables in this study. Gestational hypertension is diagnosed with BP of 140/90 mm Hg after 20 weeks of pregnancy. (15) BMI is assessed based on WHO criteria. (16)
Age, level of education, residence are considered as socioeconomic and demographic variables. Family history of diabetes, GDM, previous history of macrosomia, history of PCOD, pregnancy order are considered as obstetric variables in this study.
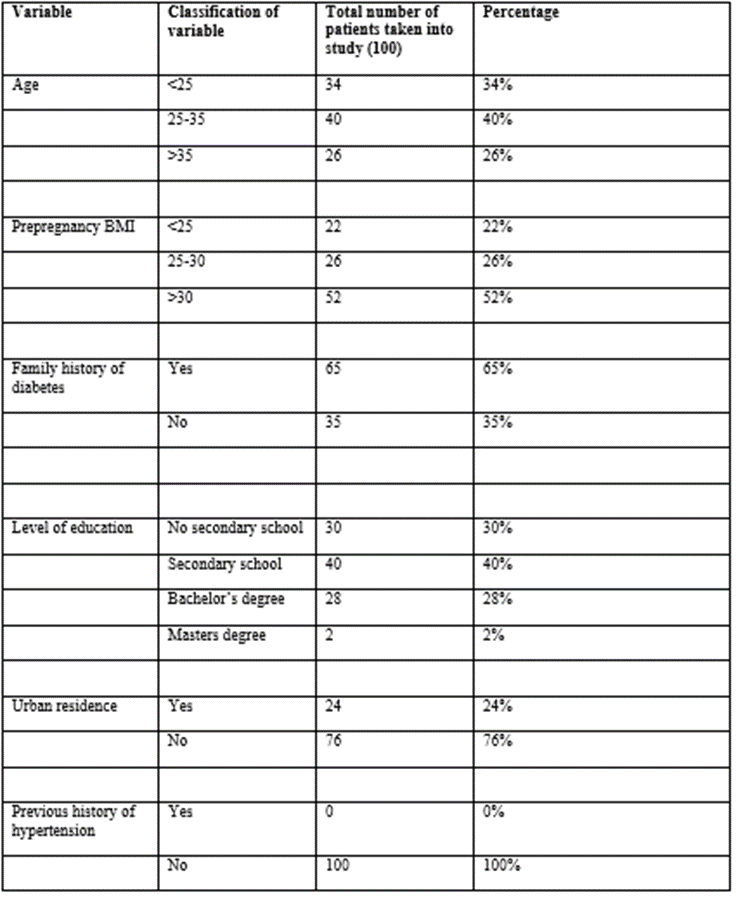
Table 1: Showing demographic, socioeconomic and health related variables of pregnant women taken into study
Out of 100 women screened for GDM, 42 were diagnosed with GDM between 24-28 weeks of gestation based on IADPSG criteria
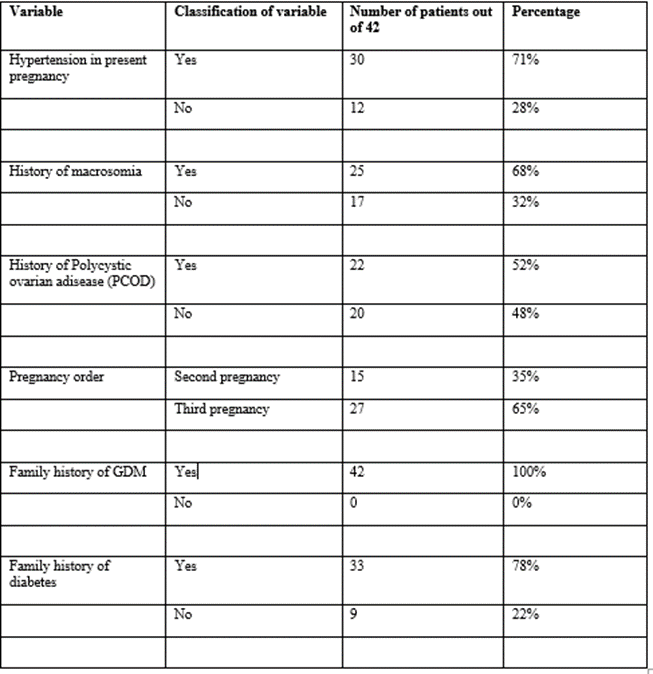
Table 2: showing Obstetric variables among women diagnosed with GDM in present study
Age
Out of 100 women taken into study, 34% were of less than 25 years, 40 % were between 25 to 35 years, 26% were of above 35 years. Out of 42 women diagnosed with GDM, 10 (23%) were above 35 years, 20 (47%) were between 25 to 35 years, 12 (28%) were below 25 years of age.
Pre pregnancy BMI
Out of 100 women, 52 were obese. GDM is detected in 39 out of 52 obese women (75%) and remaining 13 women (25%) had normal blood sugar. It shows prevalence of GDM is increasing with more pre pregnancy BMI.
Family history of Diabetes
Family history of Diabetes was seen in 65% of study population. 80 % of GDM women had diabetes in their family compared to non GDM women.
Family history of GDM
54 % of women had family history of GDM out of 100 women taken in study, out of 42 women diagnosed with GDM, almost all 100 % had family history of GDM. This shows family history plays significant role in pathogenesis of GDM.
Level of education
Out of 42 women diagnosed with GDM, only 5 women completed bachelor’s degree, showing education plays important role in generating awareness of how to prevent gestational diabetes.
Residence
Out of 42 women diagnosed with GDM, 15 were of urban residence, this shows access to better medical resources can reduce incidence of gestational diabetes
History of PCOD
In our study 52% of women with GDM had polycystic ovarian disease, PCOD women often are affected by dyslipidaemia,hyperinsulinaemia and tissue specific insulin resistance which may predispose to gestational diabetes mellitus.
History of Macrosomia
In our study, history of macrosomia is seen in 68% of GDM women. As higher amount of glucose passes through placenta into fetal circulation, extra glucose is stored as body fat causing macrosomia. For infant, it increases risk of shoulder dystocia ,clavicle fractures and brachial plexus injury and increased rate of admissions to intensive care unit and for mother, increased risk of caesarean delivery and vaginal lacerations.
Gestational hypertension
70% of GDM women developed hypertension in pregnancy, GDM and gestational hypertension common metabolic aand cardiovascular risk factors. Hyperlycaemia, insulin resistance and dyslipidaemia affect endothelial function leading to atherosclerosis and stiffness of vessels.
Increasing age is major risk factor for type 2 diabetes mellitus (17, 18).Age effect may be explained by decline in pancreatic insulin secretion capacity with age (19, 20), According to Sreekanthan et al study 75% of GDM women were above 25 years of age. (21) In our study, we noticed 66% of women with GDM were above 25 years of age. According to RCOG guidelines, pregnant women below 25 years of age are less prone to develop GDM.
In our study, we can find increased incidence of GDM in second and third pregnancy. According to Seshiah et al prevalence of GDM is rising with gravidity, from 18.1% in first pregnancy to 25.8% in grand multies. (22)
According to Sharma et al, BMI >30 was observed in 30 (64%) GDM women.(23) Similarly in our study, 75% (39/52) of GDM women were obese. Das et al and Gomez et al. reported that obesity was present in 25% and 50% of GDM women. (24) In our study we found significant association between obesity and GDM.
In our study 100% of GDM women had positive family history of diabetes which was 76% in Soheilykhah et al study. (25)
In our study 52% of women with GDM had polycystic ovarian disease (PCOD) history, similar to Bibi et al study. (26) Radon et al, found that half of PCOD diagnosed women developed GDM during pregnancy. (27) We found strong correlation between GDM and history of PCOS.
In our study, history of macrosomia is seen in 68% of GDM women. In Reece et al study, women who delivered macrosomic baby in previous pregnancy had higher risk for GDM in next pregnancy. (28)
In our study, 64% of GDM reside in rural area. Discrepancy of urban and rural in development of GDM may be associated with limited access to maternal health care and/or low socioeconomic status (29, 30).This finding implies that improvement of socioeconomic conditions may contribute to the prevention of GDM.
70% of GDM women developed hypertension in pregnancy, which shows women with GDM are at significant risk of developing hypertension. Conditions associated with increased insulin resistance may predispose patients to hypertension (31)
Limitations:
Height and weight before conception was provided by pregnant women, which may have resulted in recall bias. We cannot exclude residual confounders related to lifestyle factors. Finally, this study is lacking symptom data and weight gain in pregnancy, which could be useful.
Our study shows variability of occurrence of GDM across demographic groups and geography in India. These findings emphasize that a tailored approach in managing GDM across a diverse country like India may be needed. Obesity prior to pregnancy, older age, history of PCOD, were correlated with an increased risk of GDM. This suggests that, pregnancy is better planned before age of 25 years and pre-pregnancy weight reduction might lower risk of developing GDM. Pregnant women should be counselled about diabetogenic effect of pregnancy and risk factors for development of GDM.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
