
Research Article | DOI: https://doi.org/10.31579/2768-2757/067
1 Professor of General surgery and consultant lap surgeon.
2 Consultant Gynaecologist.
3 Residential medical officers.
*Corresponding Author: J.A. Jayalal, Jayalal H., Jekin J. Sharon, (2023), Study on the Role of Diagnostic Laparoscopy in Undiagnosed Chronic Abdominal Pain- Prospective Study, Journal of Clinical Surgery and Research, 4(1); DOI:10.31579/2768-2757/067
Citation: J.A. Jayalal, Jayalal H., Jekin J. Sharon, (2023), Study on the Role of Diagnostic Laparoscopy in Undiagnosed Chronic Abdominal Pain- Prospective Study, Journal of Clinical Surgery and Research, 4(1); DOI:10.31579/2768-2757/067
Copyright: © 2023, J.A. Jayalal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 February 2023 | Accepted: 07 March 2023 | Published: 14 March 2023
Keywords: lip transfer; reconstructive surgery; autologous graft; adjuvant alternatives; liposuction
Patients with chronic abdominal pain is the most difficult to diagnose and treat. Potentially it can be unrewarding for both patients and treating physicians.
Thereby affecting patients both physically and mentally. Chronic abdominal pain is associated with poor quality of life and the onset of depressive symptoms. Most patients in this group have already undergone numerous diagnostic procedures, including upper and lower gastrointestinal endoscopies, Ct scans, and screening for undetected carcinomas, apart from routine blood investigations. This is the time when the surgeon is approached when all other non-invasive investigations have failed to reach a satisfying conclusion. Clearly diagnostic laparoscopy is an important intermediate option between refusing to explore a patient's abdomen and performing laparotomy. Diagnostic Laparoscopy with advances in optics gives the perfect visual of the whole abdomen and further gives therapeutic advantages as well, which include target biopsies, staging of cancers, and various gynaecological pathologies. Laparoscopy is as much a surgical procedure as an exploratory laparotomy, often just as informative, and a skilled laparoscopic surgeon affords a better view of the entire peritoneal cavity than usual exploratory laparotomy. Achieving a high rate of positive diagnosis from laparoscopy requires much more than trained hands, it requires a thorough background in surgery, sound clinical knowledge, and a perception of abdominal pathologies. Most importantly it avoids unnecessary negative laparotomy in many cases. Moreover, early recovery and ambulation of patients help them get back to daily chores and are a source of delight for treating doctors.
Patients will chronic abdominal pain is the most difficult to diagnose and treat. Potentially it can be unrewarding for both patients and treating physicians [1]. Thereby affecting patients both physically and mentally, Chronic abdominal pain is associated with poor quality of life [2] and the onset of depressive symptoms [3]. Most patients in this group have already undergone numerous diagnostic procedures, including upper and lower gastrointestinal endoscopies, Ct scans, and screening for undetected carcinomas, apart from routine blood investigations. This is the time when the surgeon is approached when all other non-invasive investigations have failed to reach a satisfying conclusion. Clearly diagnostic laparoscopy is an important intermediate option between refusing to explore a patient's abdomen and performing laparotomy [4]. Diagnostic Laparoscopy with advances in optics gives a perfect visual of the whole abdomen and further gives therapeutic advantages as well, which include target biopsies, staging of cancers, various gynecological pathologies Laparoscopy is as much a surgical procedure as an exploratory laparotomy, often just as informative, and a skilled laparoscopic surgeon affords a better view of the entire peritoneal cavity than usual exploratory laparotomy. Achieving a high rate of positive diagnosis from laparoscopy requires much more than trained hands, it requires a thorough background in surgery, sound clinical knowledge, and a perception of abdominal pathologies. Most importantly it avoids unnecessary negative laparotomy in many cases. Moreover, early recovery and ambulation of patients help them get back to daily shores and is the source of delight for treating doctors.
To evaluate the efficacy of Diagnostic Laparoscopy in recognizing the etiology of undiagnosed chronic abdominal pain.
Objectives of the study:
The material for this study was obtained from patients admitted in Annammal hospital, Kanyakumari District. The study group comprises 50 patients with undiagnosed chronic abdominal pain for a duration of 3 months or more between the period of July 2020 and January to December 2022. Detailed clinical history and standard clinical evaluation followed by routine blood investigations were done. A proforma for the same was prepared which included any previous h/o abdominal surgery, therapeutic intervention is done, an association of intraoperative findings with histopathology report, complications, and post-op pain relief period. Consent for the various procedures and imaging modalities was taken initially.
Inclusion Criteria:
Exclusion Criteria:
Exclusion Criteria:
All the cases of undiagnosed chronic abdominal pain <3 months duration of both sexes.
• All cases of undiagnosed chronic abdominal pain in patients less than 14 years of age.
Procedure:
All the surgeries were conducted under general anesthesia. Ryle’s tube was inserted, along with the bladder being catheterized for all the patients prior to anesthesia. Pneumoperitoneum was created by Hassan’s technique. A 10 mm umbilical camera port was inserted and 2 lateral 5mm ports depending on the area to be visualized and suspected pathology and depending upon the presence of any previous abdominal surgery scars.
Age distribution:
Our study of 50 patients with chronic pain abdomen showed a peak incidence of chronic pain abdomen in the 3rd decade. The youngest patient in our study was 45 years old and the oldest was 69 years old. The mean age of presentation was 35 years.
Sex distribution:
Our study of 50 patients shows a female preponderance (66 %) with chronic abdominal pain. 54 % of patients in our study gave a history of pain abdomen of a duration between 18 to 36 months. About 37.14% of patients presented with pain in the periumbilical region followed by diffuse pain abdomen reported in 34.8 % of patients. Around 31 patients (62.85%) in our study had undergone a previous surgery compared to 19 (37.44 %) of them without any history of abdominal surgeries. Most of the patients had a previous history of tubectomy with subsequent adhesions. In our study of 50 patients, the most common finding was postoperative adhesions, in 36%patients. Most of the patients in this group were females and had a past history of Recurrent appendicitis was us per operative diagnosis in 14.28% of our patients. The appendices felt firm to palpate per operatively. Appendectomy was done in such patients. Subsequent histopathological examination confirmed our diagnosis in most of the cases. We did laparoscopic cholecystectomy for our patients which was confirmed on HPE. 2 Patients were diagnosed with carcinoma per operatively. One of them being carcinoma pancreas and other had peritoneal deposits whose biopsy turned out to be adenocarcinoma. Mesenteric lymph node biopsy done in one patient. Diagnosis of tubercular stricture was made in one patient. This patient underwent resection and anastomosis of long segment stricture and stricturoplasty for another short segment by open method. Post operatively ATT was started, and patient was followed up. HPE confirmed tuberculosis. In 4(8.01%) of patients peritoneal and omental nodules (<5mm> Around 10 % of cases i.e., 5 patients in the current study were diagnosed with gynecological disease including corpus luteal cyst, PCOD, endometriosis, chronic ectopic. Gynecological opinion was taken in all these cases.
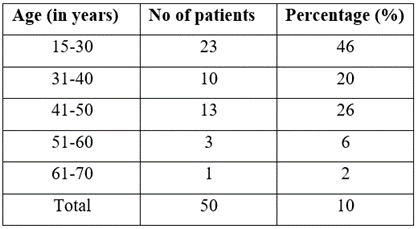
Table 1: Age distribution of patients presenting with chronic abdominal.
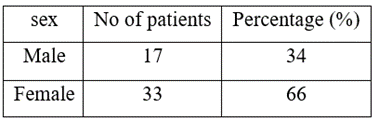
Table 2: Sex distribution of patients with chronic abdominal pain.
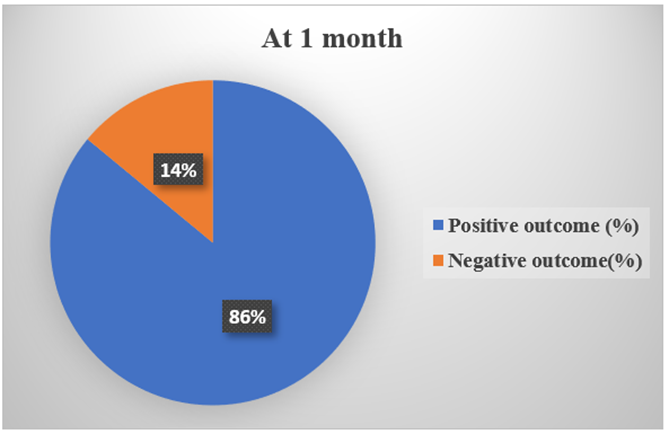
Figure 1: Sex distribution.
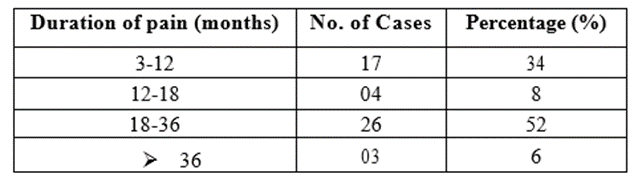
Table 3: Duration of pain before laparoscopy.
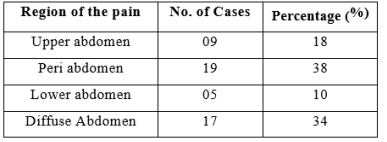
Table 4: Location of Pain.
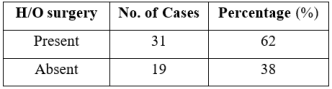
Table 5: History of previous abdominal surgeries.
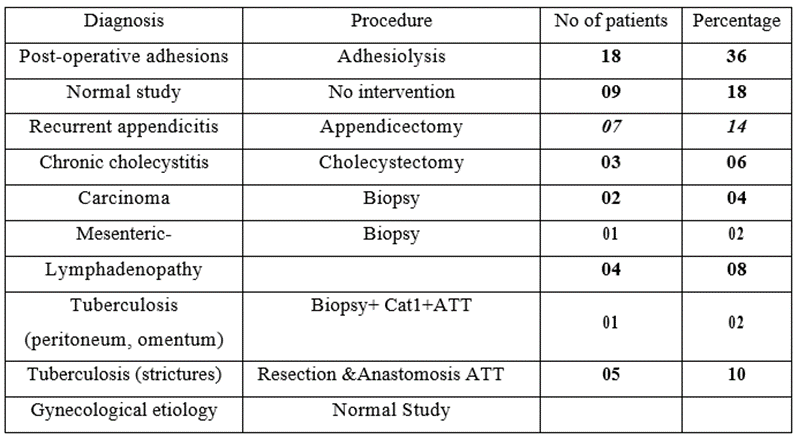
Table 6: Findings on Laparoscopy and intervention done.
Morbidity:
In most of our cases there was no post-operative complications except in three patients who developed surgical site infections which was managed conservatively with antibiotics and alternate day wound dressings. No mortality was encountered in our study.
Duration of hospital stay:
Post-operative hospital stays ranged from 4-11 days with a mean duration of stay of 5.5 days.
Duration of procedure:
The average time taken foe operative procedure was 67.l4 minutes and one patient required conversion to open procedure (due to technical difficulties).
Follow up:
During the follow up period, all the patients were reevaluated for pain. Review was done at one month and three months post operatively. Subjective assessment of pain was done, positive outcome (pain reduced/disappeared) and negative outcomes (persistence of pain/worsened) were noted. 5 patients could not be followed up

Table 7: Outcome of the procedure.
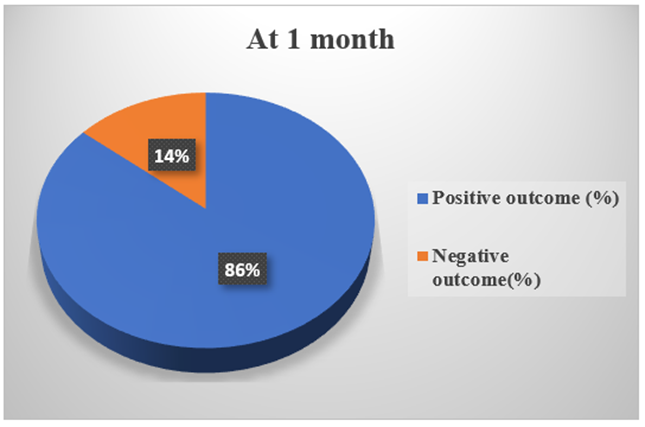
Figure 2: Outcome at 1 month.

Figure 3: Intraoperative pictures.
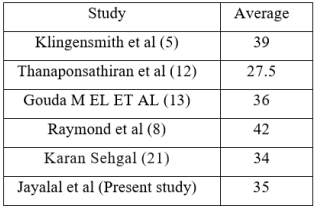
Table 8: Comparison of average age incidence.
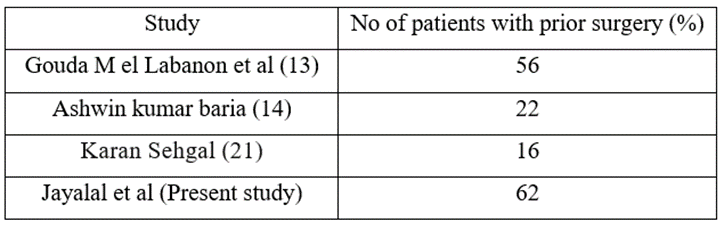
Table 9: Comparison of past history of abdominal surgeries.
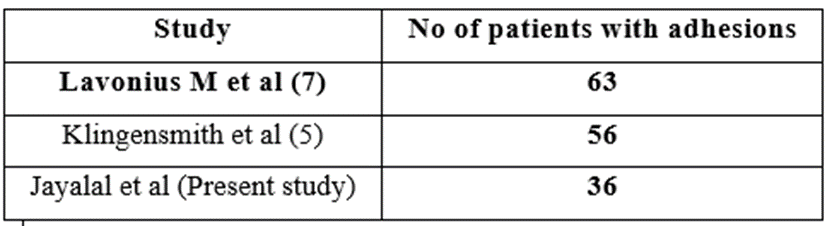
Table 10: Comparison of patients with adhesions.
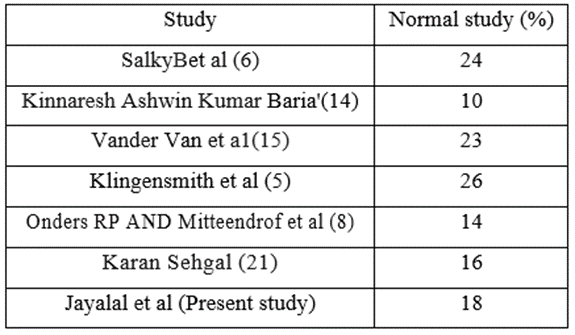
Table 11: Comparison of patients with normal study at laparoscopy.
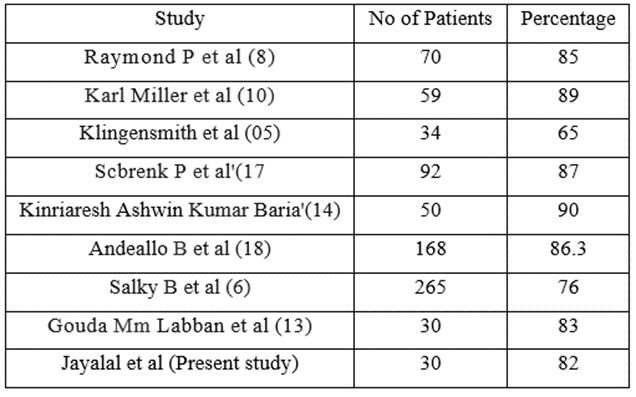
Table 12:

Table 13: Therapeutic efficacy.
The aim of our study was to study efficacy of diagnostic laparoscopy as an investigative, therapeutic modality in diagnosis and management of patients with chronic abdominal pain, for which prospective study of 50 patients with duration of pain more than 3 months who were admitted in surgical wards of our hospital at Kanyakumari Government medical college.
Age and sex incidence:
There were 17 males and 53 female patients in the study. The age group of patients in this study ranged from 15-69 years with mean age being 35 years. Male: Female ratio was 1:1.9.
In study involving 34 patients by Klingensmith et a1 [5] the majority were females (85 %). The average age in this study was 39 years.
In study Than aponsathron et at [12], of 30 patients with chronic right lower quadrant pain, the average age was 27.5 years.
In study Raymond et a1 [8] for utility laparoscopy in chronic abdominal pain involving 70 patients, average age 42 years.
In study by Gouda M El- Labban and Emad N Hokkam [l3] involving 30 patients, average age of presentation was 36 years.
All the above studies show that female sex was commonly afflicted by chronic pain abdomen and average age of presentation was similar.
Pain duration:
In our study duration of pain ranged from 3 months to 3 years. In study of Raymond et al [8,9] of 70 patients, duration of pain ranged from 3 months to 5 years. In study by Gouda M El-Labban and Emad N Hokkam [13] involving 30 patients, the duration of pain ranged from 3 months to 15 months.
Prior Surgery:
In our study of 50 patients, 31 patients had previous history of abdominal surgery. In study of klingensmith et al [5] involving 34 patients, most of the patients had previous history of abdominal surgery.
In study by Gouda M El-Labban and Emad N Hokkam [4,3] involving 30 patients, 3 7 had previous history of abdominal surgery.
In a study by Kinnaresh Ashwin Kumar Baria [4] involving 50 patients, 4 4 of them had a previous history of abdominal surgery.
Laparoscopic Diagnosis:
In our study laparoscopy identified pathology in 41 patients (82.85 %). No abnormality was found in remaining 09 patients (17.14%) who were just observed without any intervention.
Post-operative adhesion:
36 % of patients in our study were found to have intestinal adhesions secondary to prior surgery, mostly tubectomy (in 8 patients). Some patients had history of appendectomy (in 10), cholecystectomy (in 3), hysterectomy (in 5), and one patient history of laparotomy for hollow viscous perforation. Adhesiolysis was done as a therapeutic procedure. Lavonius M et al [7] in their study of 46 patients reported post-operative adhesions in 63
Laparoscopy has an effective diagnostic accuracy and therapeutic efficacy in management of patients who presented with chronic pain abdomen, especially in whom conventional methods of investigations have failed to give an explanation.
Laparoscopy is safe, quick, effective modality of investigation for chronic abdominal pain. Diagnostic laparoscopy has a high diagnostic and therapeutic efficacy. Ability to find a cause for abdominal pain or exclude a more major cause, not only avoids any further investigations but also plays a significant role in satisfaction for the patient and relatives.
Laparoscopy has an added benefit of diagnostic and therapeutic intervention, which can be carried out in same sitting, thereby avoiding the need for another hospitalization or another exploration of abdomen.
With the help of diagnostic laparoscopy, all the unnecessary laparotomies can be avoided in patients with normal findings, who don’t need any surgical interventions.
Hence, Diagnostic laparoscopy had an authoritative role in management of patients with chronic abdominal pain.
Summary:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
