
Research Article | DOI: https://doi.org/10.31579/2692-9759/107
1 Cardiology department, Faculty of Medicine, Alexandria University, Egypt.
*Corresponding Author: Gehan Magdy, Cardiology department, Faculty of Medicine, Alexandria University, Egypt.
Citation: Magdy G., Salah E. Tahhan, Fatema A. Z. Ahmed, Hasanein M., (2023), Study of Global Longitudinal Strain And N-Terminal Pro Brain Natriuretic Peptide as Predictors of Outcome in Acute St-Segment Elevation Myocardial Infarction Patients Undergoing Primary Percutaneous Coronary Interventions, Cardiology Research and Reports. 5(4); DOI:10.31579/2692-9759/107
Copyright: © 2023, Gehan Magdy. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 September 2023 | Accepted: 21 September 2023 | Published: 29 September 2023
Keywords: acute ST elevation myocardial infarction; global longitudinal strain; NT-proBNP
Objective: Acute ST-segment elevation myocardial infarction (STEMI) patients should be risk-stratified in order to enhance the outcome. Our study was designed to assess the prognostic value of N-terminal pro brain natriuretic peptide (NT-proBNP) and global longitudinal strain (GLS) of the left ventricle in patients presenting with acute STEMI and treated by primary percutaneous coronary interventions (PPCI).
Methods: the study included 100 STEMI patients treated by PPCI, their age was 55.69 ±8.70 years, all patients were subjected to analysis of NT-proBNP plasma level, and calculation of the GLS, and follow up was done for 6 months for major adverse cardiac events (MACE) occurrence.
Results: patients were divided into two groups according to MACE, group I (20 patients who had MACE), group II (80patients without MACE), the NT-proBNP was significantly higher and the GLS was significantly lower in group I, and by multivariate regression analysis GLS was shown to be the most significant predictor of MACE (p value=0.003).
Conclusions: Our study concluded that both GLS and NT-proBNP are significantly related to MACE, with GLS being the single most significant predictor for MACE in patients with acute STEMI treated by PPCI.
Acute ST-segment elevation myocardial infarction (STEMI) is one of the major contributors to adverse cardiovascular outcomes. Left ventricular ejection fraction (LVEF) is a predictive factor for outcomes in STEMI patients [1, 2]. However, the LVEF is both preload and afterload dependent, with substantial interobserver variability. Two-dimensional speckle tracking echocardiography (2D-STE) is a B-mode based approach that can assess regional myocardial deformation through measuring of global longitudinal strain (GLS), which has been shown to be less affected by loading conditions [3-7]. recent studies reported that myocardial deformation imaging by 2D-STE after acute myocardial infarction (AMI) predicts cardiovascular outcomes such as new onset heart failure (HF) and cardiovascular death [8, 9].
The plasma concentration of brain natriuretic peptide (BNP) increases after AMI, [10] and after acute coronary syndromes [11] and the levels of BNP and N-terminal pro brain natriuretic peptide (NT-proBNP) are recognized as new and useful biochemical markers for both the diagnosis and prognosis of HF [12-14]. However, data regarding the relationship between increased NT-proBNP level and adverse cardiac events after AMI is still limited. Our study is designed to assess the prognostic value of NT-proBNP and GLS of the left ventricle (LV) in patients presenting with acute STEMI and treated by primary percutaneous coronary interventions (PPCI).
Our study is a prospective cohort research and included 100 patients presented to our cardiology department (from march2019 to December 2019) by acute STEMI and underwent PPCI within 12 hour of the onset of chest pain, excluding those with LVEF≤40Percentage, previous history of percutaneous coronary interventions( PCI )or coronary artery bypass graft (CABG), left bundle branch block, atrial fibrillation , significant valvular disease, also patients with non-cardiac causes that could interfere with NT-Pro BNP level were excluded .All patients included in the study were subjected to the followings:
Demographic and clinical data: Including age, gender, weight, height, body mass index (BMI), and history of clinical risk factors, and Killip class were also assessed.
12 lead electrocardiograms (ECG): Was done to all patients to diagnose STEMI [15].
Transthoracic echocardiography: It was performed within 48 h of admission to our institution and after patients were treated by PPCI. It was done using a Philips iE33 xMATRIX echo system, and the following parameters were measured:
N T- pro BNP level: Peripheral samples of plasma were obtained on admission for measurements of NT-pro BNP, and analysis was performed using the Modular Analytics E170 NT-proBNP immunoassay (Roche Diagnostics, Mannheim, Germany) [18].
Follow up: for all patients for the occurrence of major adverse cardiovascular events (MACE) had been done for 6 months post discharge (by telephone at 1, 3, and 6 months). The primary end points for MACE occurrence in the study were (all-cause mortality, cardiovascular mortality, stroke, reinfarction, and hospitalization due to HF).
Data were analyzed using IBM SPSS software package version 20.0 (Armonk, NY: IBM Corp). Categorical variables were described using number and percent, compared using the chi-square test and continuous variables were described using mean and standard deviation, and compared using the Mann-Whitney test. The Spearman correlation coefficient, receiver operator characteristic (ROC) curve, and univariate and multivariate logistic regression tests were used, PLess than0.05 was considered statistically significant.
Our study included 100 STEMI patients (their age 55.69 ±8.70 years, and 75Percentage were males), all patients underwent PPCI with stent placement and all patients were kept on dual antiplatelet therapy, high intensity statins and by the end of 6-month patients were classified into 2 groups:
Baseline clinical and laboratory characteristics: (Table1)
There was no statistically significant difference between the two groups regarding age, gender, presence of risk factors, site of infarction, and troponin level however the Killip class II-III (MCp= 0.002), and NT pro-BNP were significantly higher in group I of patients (P Less than0.001)
Angiographic characteristics: (Table1)
All patients underwent successful PPCI with stent placement, and TIMI grade 3 flow was achieved in all patients, there was no statistically significant difference between the two groups regarding the culprit coronary artery involved, the need for thrombus aspiration, or the total number of stenotic coronary vessels.

Table 1: Clinical, laboratory, and angiographic characteristics of the two groups of patients
Echocardiographic characteristics: (Table2)
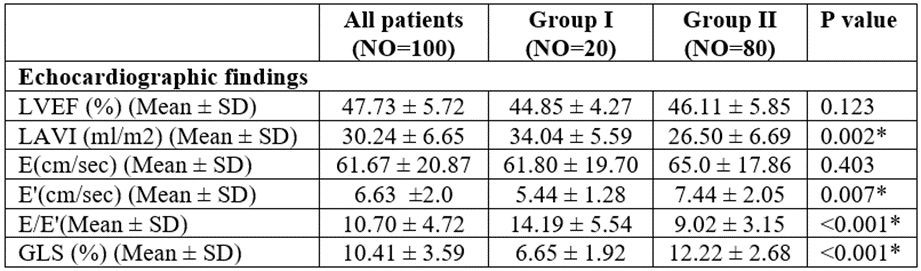
Table 2: Echocardiographic characteristics of the two groups of patients
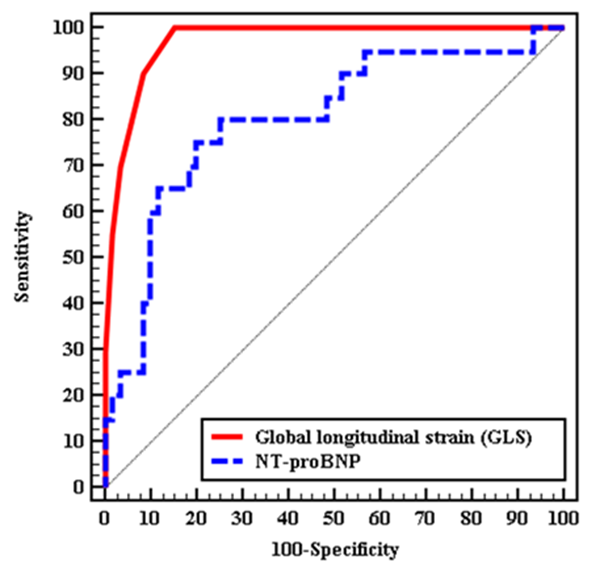
Figure 1: overlapping ROC curve for both GLS and N-proBNP to predict patients with MACE
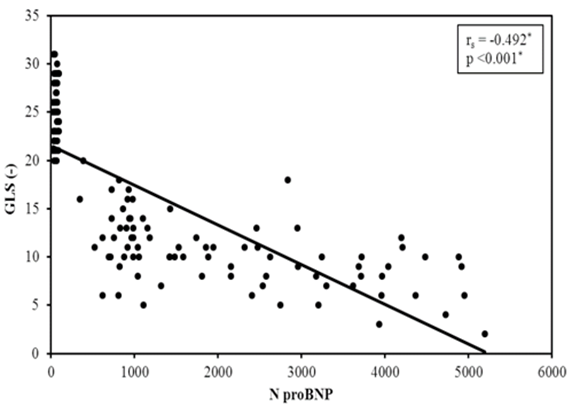
Figure 2: Correlation between NT-proBNP and GLS in cases group.
We performed univariate and multivariate COX regression analysis for the parameters affecting MACE. In univariate analysis, the highly significant predictors were the NT-pro BNP level, E/E’, and GLS with a p value Less than0.001 for all. In multivariate regression analysis, the GLS was shown to be the most significant predictor for MACE in patients with STEMI (p value=0.003, OR “95PercentageC. I” = 0.721 (0.580 – 0.896)).
One of the primary causes of mortality worldwide is AMI though the use of early PPCI is growing and has greatly reduced mortality [19]. The evaluation of GLS, which depicts the function of longitudinally oriented cardiac fibers within the subendocardium and is particularly susceptible to ischemia, has received the majority of attention [4, 5)]. According to recent studies, GLS has been linked to regional cardiac function recovery and in-hospital outcomes in patients with AMI [20.21]. Also, it has been reported that the plasma level of BNP, a neurohormone that increases immediately after AMI in response to increased wall tension [22,23]. The combination of NT-proBNP with GLS improved risk stratification for MACE reduction, and in our study we found that both GLS and NT-proBNP were among the main predictors of MACE w(p value Less than0.001), and the multivariate analysis showed that GLS was the single most significant predictor of adverse outcome, and our findings are in agreement with many published studies, Sun Hwa Lee et al. [24] who studied a total of 171 patients with anterior STEMI who underwent successful PPCI , concluded that GLS is a powerful parameter related to development of HF, which is totally in agreement with our results. Mingzhu Xu et al. [25] who studied clinical outcomes in 405 patients with STEMI treated by PPCI, they found that the level of NT-BNP was an independent predictor for in-hospital HF incidence in AMI patients with preserved LVEF. In our study NT-ProBNP was a significant predictor of MACE in univariate regression but not in multivariate model. Also, Richards, et al. [26] who studied the prognostic value of levels of BNP, (NT-proBNP), and radionuclide LVEF in 666 patients with AMI. The B-type peptides and LVEF were significant predictors of mortality, HF, and new myocardial infarction. The combination of NT-proBNP (or BNP) with LVEF substantially improved risk stratification beyond that provided by either alone. And this was completely in agreement with our results as we found that NT-proBNP is among the univariate significant predictors of MACE in AMI patients, however, our study included only patients with EF Greater than 40Percentage unlike Richards et al who included patients regardless of their EF. Actually, the relationship between GLS and NT-proBNP reflects a pathophysiological association between longitudinal myocardial fiber dysfunction and the secretion of natriuretic peptides. This couldn’t be explained by LVEF, which quantifies volume displacement, without an accurate assessment of myocardial function [27, 28]. our study is one of the few studies evaluating the incremental prognostic value of both NT pro BNP and GLS in patients presented with acute STEMI with preserved LVEF, but several studies are evaluating each one of them separately and this was in agreement of the study done by Ersbøll et al. [21] who studied 548 patients with AMI Within 48 hours of admission, assessment of GLS was performed, and NT- pro-BNP was measured, they found that GLS is significantly impaired in patients with in-hospital HF with LVEF Greater than 40Percentage, and multivariate analysis suggests that reduced GLS is the single most powerful predictor of HF occurrence.
Our study concluded that both GLS and NT-proBNP are significantly related to MACE, with GLS being the single most significant predictor for MACE in patients with acute STEMI treated by PPCI.
The present study has some limitations including; the study cohort was relatively small with short follow up time, and GLS, and NT-proBNP hasn’t been assessed at time of follow up for endpoints.
| 2D-STE | Two-dimensional speckle tracking echocardiography |
| A | Late mitral inflow velocity |
| AMI | Acute myocardial infarction |
| BNP | Brain natriuretic peptide |
| CAD | Coronary artery disease |
| e' | Mitral annulus early diastolic velocity |
| ECG | Electrocardiogram |
| HF | Heart failure |
| LAD | Left anterior descending coronary artery |
| LAVI | Left atrial volume index |
| LCX/OM | Left circumflex coronary artery/obtuse marginal |
| LV | Left-ventricle |
| LVEF | Left ventricular ejection fraction |
| MACE | Major adverse cardiovascular events |
| NT-proBNP | N-terminal pro brain natriuretic peptide |
| PCI | Percutaneous coronary interventions |
| PPCI | Primary percutaneous coronary interventions. |
| RCA | Right coronary artery |
| STEMI | ST-segment elevation myocardial infarction |
The Ethics Committee of faculty of Medicine, Alexandria University had approved the Study, and informed consent was obtained from all individual participants included in the study.
The authors declare that they have no competing interests.
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript, the whole work was done in cardiology department in the faculty of medicine, Alexandria University.
GM did the acquisition and interpretation of echocardiography data, write and revised the article, FM performed data collection, and analyzed the data ST, and MH had performed the final data analysis. All authors had read and revised the article critically for important intellectual content and final approval of the version to be published.
Authors acknowledge the staff of cardiology department, Alexandria main University Hospital for their unlimited support during the study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
