
Research Article | DOI: https://doi.org/10.31579/2641-0419/409
Clinique Louis Pasteur, Essey-lès-Nancy, France.
*Corresponding Author: Zukaï Chati, Clinique Louis Pasteur, Essey-lès-Nancy, France
Citation: Zukaï Chati, Samuel Tissier, Clemence Balaj, Nacima Benzaghou, Max Amor, et al, (2024), Stress CMR VS Stress Echo: Real-world multimodal cardiovascular imaging for myocardial ischemia screening. Insights from the first phase of “Nancy Ischemia Registry”, J Clinical Cardiology and Cardiovascular Interventions, 7(11); DOI: 10.31579/2641-0419/409
Copyright: © 2024, Zukaï Chati. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 September 2024 | Accepted: 24 September 2024 | Published: 01 October 2024
Keywords: stress cmr; stress echo; myocardial ischemia; real ischemia register; major adverse cardiovascular events
In a real world, the impact of different functional and anatomical imaging techniques is not really known.
Objectives
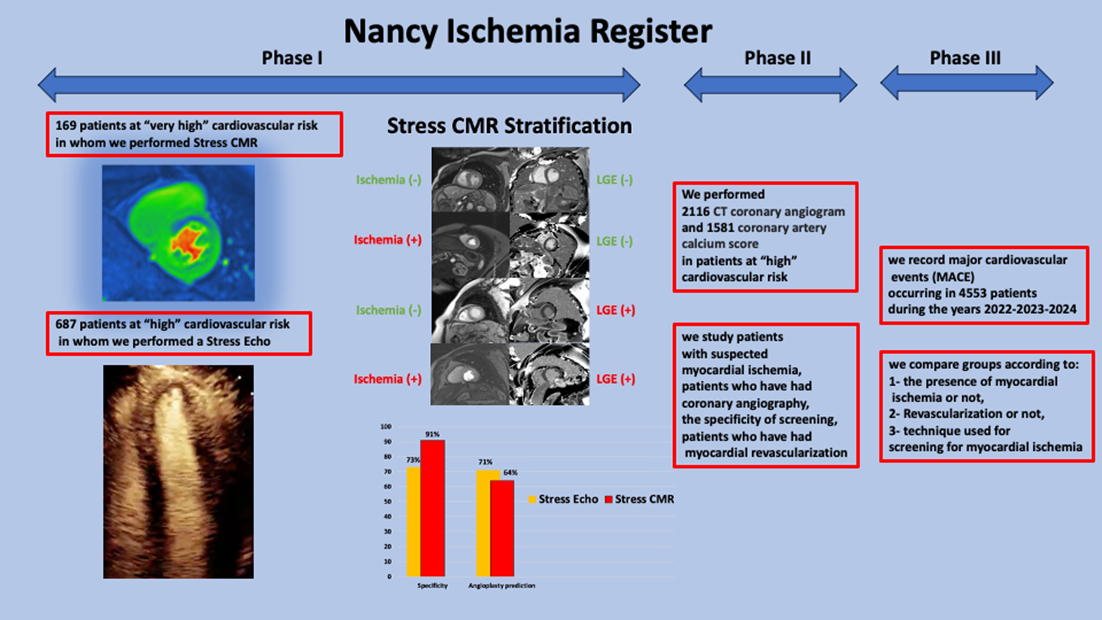
“Nancy Ischemia Registry” is a prospective registry, without inclusion or exclusion criteria, which analyzes the respective real impact and consequences of different functional and anatomical imaging techniques on major adverse cardiovascular events.
In a “first phase”, we compared two functional imaging techniques used in our center: Stress CMR and Stress Echo.
Materials & Methods
We consecutively included 169 patients in whom we performed Stress CMR and 687 patients in whom we performed Stress Echo.
Results
We detected myocardial ischemia in 59 patients by Stress CMR (35% of patients) and in 123 patients by Stress Echo (18% of patients).
Coronary angiography confirmed at least one significant lesion in 54 patients in the Stress CMR group (PPV 91%) and in 90 patients in the Stress Echo group (PPV 73%). In patients with at least one significant coronary lesion, coronary angioplasty was performed in 38 patients (64% of true positives) in the Stress CMR group versus 64 patients in the Stress Echo group (71 % of true positives).
Conclusion
Stress CMR has a better specificity than Stress Echo for the detection of myocardial ischemia. However, detection of myocardial ischemia by Stress Echo more often leads to coronary revascularization than by Stress CMR. This difference in this register is probably explained by a higher sensitivity of the Stress CMR for the detection of myocardial ischemia linked to less severe lesions, whereas the Stress Echo mainly detects more severe lesions.
Cardiovascular magnetic resonance (CMR), Major adverse cardiovascular events (MACE), CT coronary angiogram (CTCA), Coronary artery calcium score (CACS), Late gadolinium chelate enhancement (LGE), Fractional Flow Reserve (FFR), Left Anterior Descending (LAD), coronary artery disease (CAD).
Introduction
The presence of myocardial ischemia is a very important prognostic factor (1).
According to all European and American recommendations, anatomical and functional imaging is a recommended tool for the detection and management of myocardial ischemia (2-5).
We have many results from clinical trials that show the value of different techniques and the stratification of cardiovascular risk according to the presence of myocardial ischemia, the presence of myocardial sequelae or both (6-8).
However, most of these clinical trials, through inclusion and exclusion criteria, rule out short-term and long-term analyzes of certain patients, often the most severe (proximal coronary stenosis) or patients with little or no symptoms (9-11).
We wanted by "Ischemia Nancy Register", of consecutive patients without exclusion criteria, to analyze the results in current practice, real exercise, in the field of screening for myocardial ischemia. Through several phases, we will study, by longitudinal analysis, the different techniques for detecting myocardial ischemia (anatomical and functional imaging) and compare:
I- In a first phase (in this article), we compared two functional imaging techniques: Stress CMR and Stress Echo.
II- In the second phase, we will include the results using an anatomical imaging technique: CT coronary angiogram (CTCA) and coronary artery calcium score (CACS).
III- In a third phase, we wish to compare major adverse cardiovascular events (MACE) in all patients according to: 1- the presence of myocardial ischemia, 2- myocardial revascularization, and 3- the functional and anatomical detection technique.
Stress Echo has become an increasingly accessible modality for the detection of myocardial ischemia. According to the latest guidelines from European and American societies, Stress CMR has gained significant value as a functional imaging modality for screening for myocardial ischemia (4-6).
The constitution of a register “Nancy Ischemia Register” of consecutive patients could play an important role in the management of patients with chronic obstructive coronary artery disease.
In this article, we present the results of the first phase. We prospectively screened for the presence of myocardial ischemia by Stress CMR and Stress Echo in patients at high cardiovascular risk.
Study population
Between May 2021 and December 2022, we consecutively included 169 patients in whom we performed Stress CMR. the patients in this group were considered at “very high” cardiovascular risk because the majority were diabetics “with or without” a coronary history and in particular coronary angioplasty (high prevalence of myocardial Ischemia). Considering CMR stress as a very sensitive technique, in real practice, we have chosen in these very high-risk patients to benefit from optimal detection of myocardial ischemia. Stress CMR also allows us to stratify their prognosis (3).
Between January 2022 and December 2022, we consecutively included 687 patients in whom we performed a Stress Echo. patients in this group were considered at “high” cardiovascular risk; often diabetics with little coronary history (moderate prevalence of myocardial ischemia). In real practice, the detection of myocardial ischemia in this group was rather systematic, allowing us to better stratify their prognosis and intervene in the event of a positive or suspicious examination.
Stress CMR protocol:
Cine CMR sequences associated with first-pass perfusion and late enhancement form the basis of our stress CMR. All contrast-enhanced CMR studies were performed with a 3-T cardiac MRI unit (MAGNETOM Lumina, SIEMENS, Germany), and a twelve-element phased-array cardiac coil was used for signal reception. ECG gating and triggering were performed using the vector cardiographic method (Figure 1).
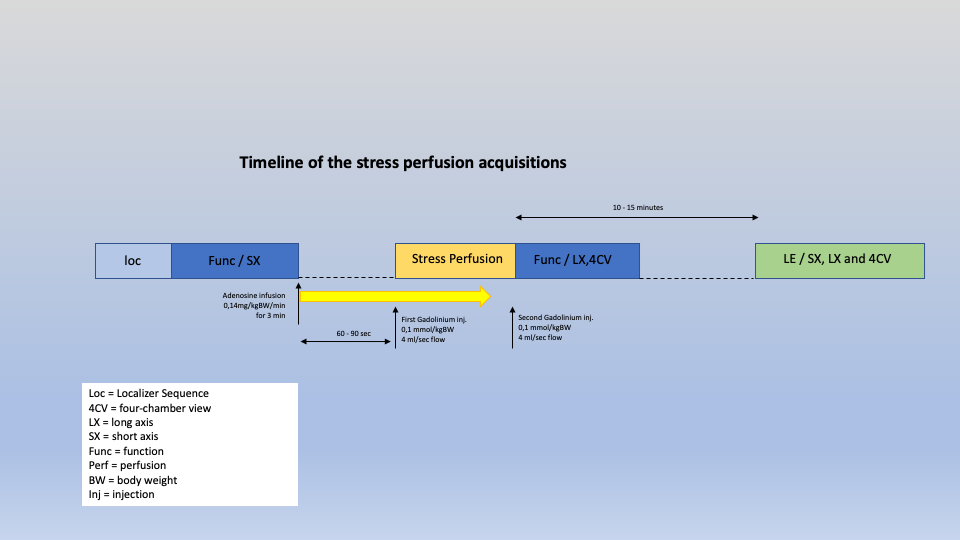
Figure 1: Stress CMR protocol
Patients were instructed not to drink coffee or tea and not to have oral β-blockers for at least 24 hours before the adenosine-induced stress MRI. The procedure is explained to the patient in detail with special emphasis on possible side effects of adenosine infusion (thoracic oppression / chest pain, dyspnea and anxiousness). Two I.V. lines are placed in each of the antecubital veins, one for adenosine and one for the gadolinium bolus connected separately.
Fast survey images were acquired first to determine the principal reference axis of the left ventricle.
The rest cine CMR is performed with cine sequences using steady-state free precession (slice thickness 8 mm, with 2 mm interslice gaps, matrix 448x448). These pulse sequences include slices covering the whole left ventricle (LV) in its short axis from base to apex and one to three long-axis slices of the LV and four-chamber views.
Perfusion CMR is based on a qualitative analysis of the enhancement of the myocardial signal during the first pass of a bolus injection of gadolinium chelate. Stress perfusion MR images were obtained with a gradient-echo sequence by using saturation recovery turbo flash sequence (TR, 158 ms; TE, 1 ms; inversion time, 95 ms; matrix, 172 x 192; section thickness, 10 mm) with movement correction. The acquisitions are performed under pharmacological stimulation during the last half of the adenosine infusion (0,14 mg/kg/min over 3 minutes) and right after injection of the bolus of gadolinium 0,1mmol/kg), ideally during a breath hold. Symptoms, heart rates and ECG activity were carefully monitored during the adenosine infusion and after imaging. The temporal resolution of perfusion sequences allows the acquisition of three to five slices within an R-R space... at least three slices in the short axis of the LV, and most often a slice in the vertical plane of the long axis and another in the horizontal plane of the long axis.
At the end of the Stress perfusion CMR acquisition, a second injection of gadolinium is done at the same dose and rate.
Late gadolinium chelate enhancement (LGE) Two-dimensional or three-dimensional phase-sensitive inversion recovery sequences can be used, 10-15 minutes after the injection of a total of 0.2 mmol/kg gadolinium chelate. Inversion time is optimized for each patient according to an inversion time scout image to optimize myocardial nulling. The slice thickness is 6 mm.
The total examination time is about 30 minutes.
Stress Echo protocol:
We used a standard protocol for stress echocardiography under dobutamine. A dose graduated from 10 to 40 µg/kg/min with four levels: rest, first level, peak, and recovery.
The heart rate had to reach 85% of the theoretical maximum rate. If needed, 0.5 to 1 mg has been given to further increase the heart rate. The recovery was gradual, and we never used a beta blocker. The criteria for positivity were based on the appearance of chest pain, ECG modification and the presence of segmental kinetics disorder of the left ventricle (≥ 3 segments). We use a Philips EPIQ CVx device (Seattle, Washington, USA) for all patients.
At this phase, our statistical data was simply performed with Microsoft Excel (Microsoft Corporation, Washington, USA). data were summarized with mean +/−95% confidence interval.
In the Stress CMR group of 169 patients, the examination was considered “positive” with suspicion of myocardial ischemia in 59 patients (35% of patients). In the Stress Echo group of 687 patients, the examination was considered “positive” with suspicion of myocardial ischemia in 123 patients (18% of patients). (table1)
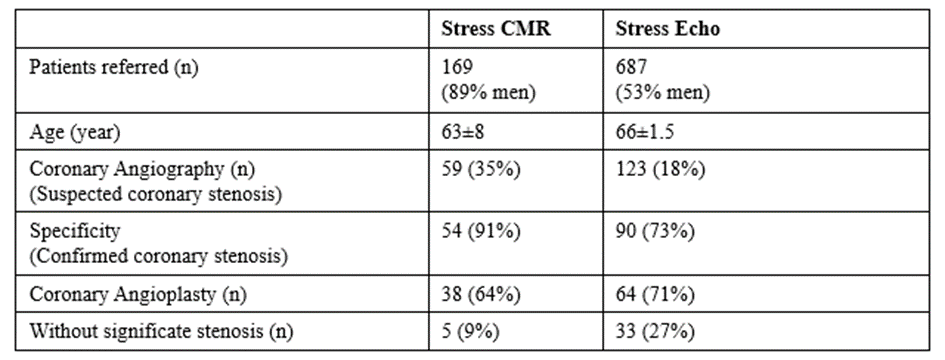
Table 1: Presentation of the population of patients participating in the phase 1 registry.
Coronary angiography was performed in patients with suspected myocardial ischemia. Coronary angiography confirmed at least one significant lesion in 54 patients in the Stress CMR group (91% Positive Predictive Value) and in 90 patients in the Stress Echo group (73% Positive Predictive Value). (Figures 1, 2)
On coronary angiography, there was no lesion considered significant in 5 patients in the Stress CMR group (9% of patients: false positives) compared to 33 patients in the Stress Echo group (27% of patients: false positives). (Figure 2).
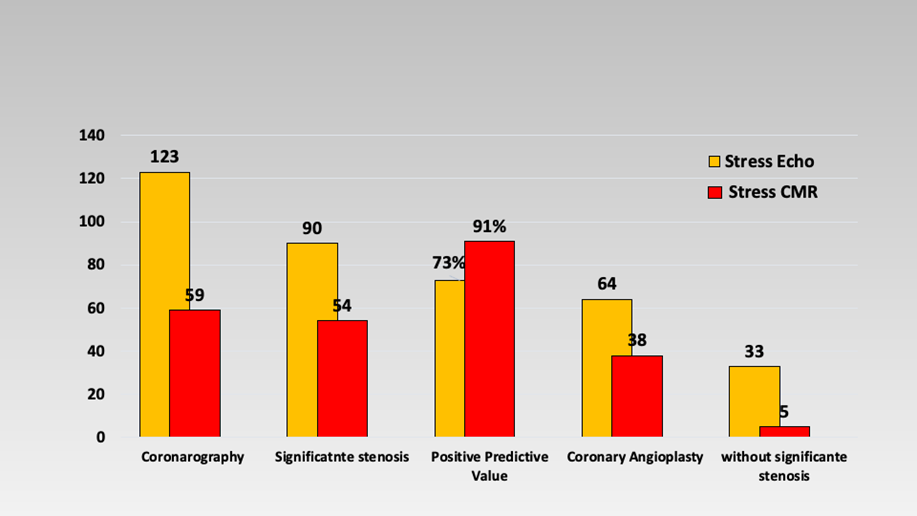
Figure 2: Presentation of the main results. comparison between Stress CMR and Stress Echo. The results are presented by the number of patients.
In patients with at least one significant coronary lesion (≥70% or FFR ≤ 0.80) coronary angioplasty was performed in 38 patients (64% of true positives) in the Stress CMR group versus 64 patients in the Stress Echo group (71 % of true positives). (Figure 3)
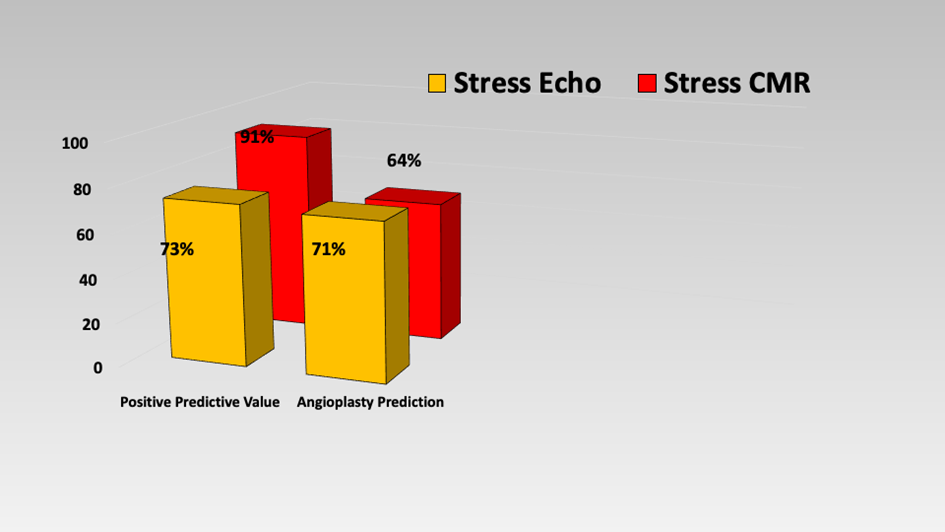
Figure 3: Comparison of the Positive Predictive Value of Stress CMR and Stress Echo and of the prediction of coronary angioplasty according to the two techniques.
The stratification of cardiovascular risk by Stress CMR plays a very important role (6).
Figure 4 presents the distribution by 4 groups of patients according to the presence or absence of myocardial ischemia and/or LGE and their
distribution within each group according to the completion of revascularization by coronary angioplasty or not.
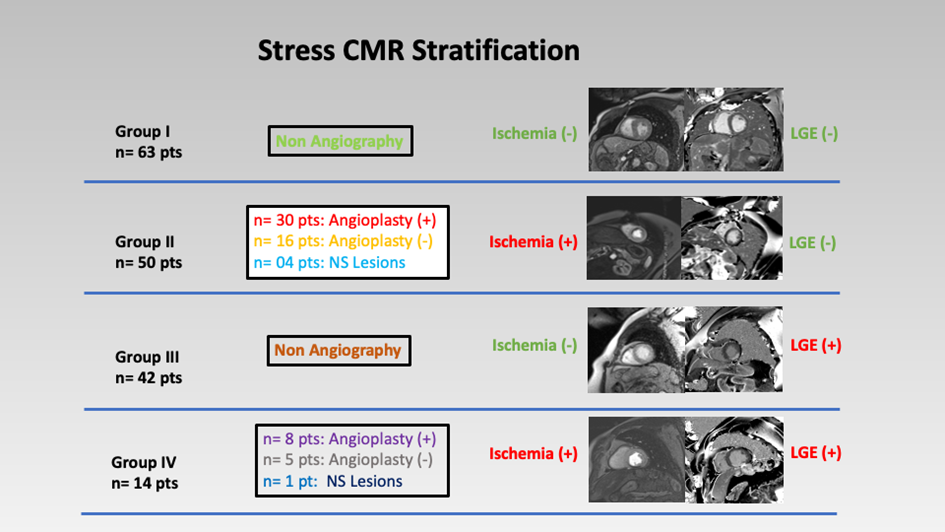
Figure 4: Stratification by stress CMR according to the presence of ischemia and/or LGE and at the same time according to the follow-up by coronary revascularization or not. Group I: absence of ischemia and absence of LGE. Group II: presence of ischemia and absence of LGE. Group III: absence of ischemia and presence of LGE. Group IV: presence of ischemia and presence of LGE. Figure 5 shows a case of patients with extensive septal and anterior wall myocardial ischemia with extensive coronary lesions on coronary angiography.
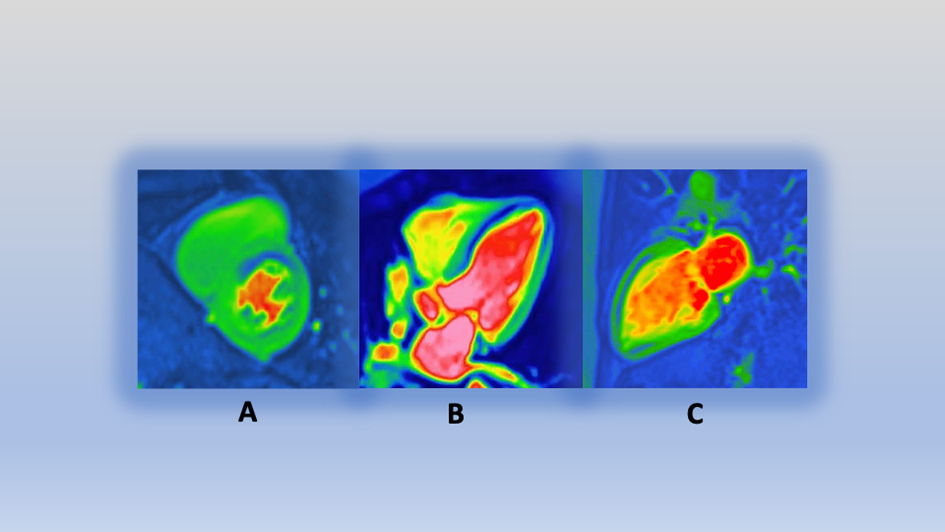
Figure 5: Stress CMR images showing in a patient A, B, C: Antero-Septal wall perfusion defect.
Figure 6 shows the case of a patient with a very demonstrative Stress Echo. the patient presented apical dyskinesia under dobutamine which corresponded on coronary angiography to distal thrombosis of the distal Left Anterior Descending (LAD) Coronary.
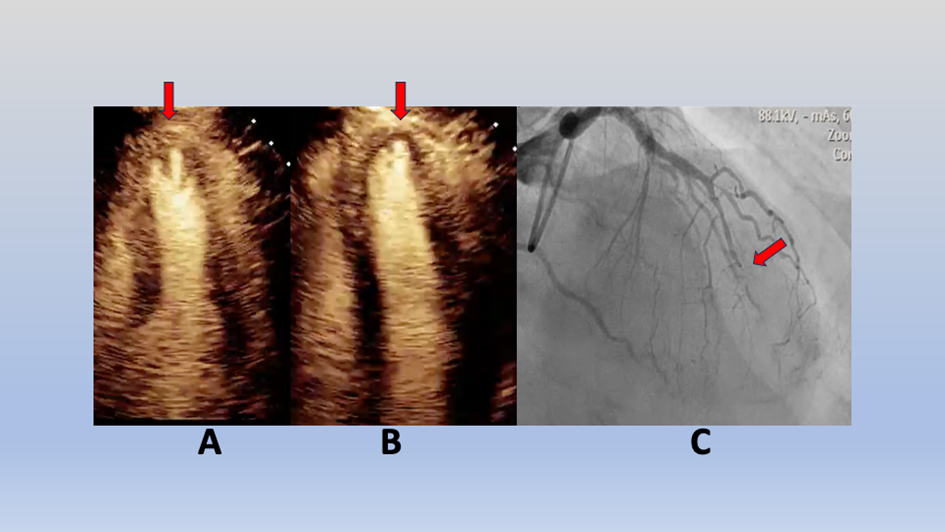
Figure 6: Stress Echo images showing in the case of a patient A: at Rest, B: Apical dyskinesia with Stress Dobutamine, C: Distal Left Anterior Descending Coronary Thrombosis (Coronary Angiography).
We present the first results of phase 1 of the “Nancy Ischemia Registry”. The goal at this early stage is to compare two functional imaging methods and to see their specificity in detecting myocardial ischemia and the consequences on myocardial revascularization. These results reflect a real image of the patients we examine in our practice outside of clinical trials where patients are selected according to precise criteria and excluding a part, often with severe lesions, to respect a strategy fixed in advance.
Stress Echo plays an important role in the detection and management of myocardial ischemia (12-13). The stratification of cardiovascular risk by Stress CMR becomes a gold standard, screening for ischemia and late enhancement (6-8).
We usually use these two functional imaging techniques with some hindsight. Our results show that the two techniques have a good specificity in the detection of myocardial ischemia after verification by Coronary Angiography. We cannot comment on their sensitivities because we did not perform Coronary Angiography on patients without suspicion of myocardial ischemia. We are within the framework of a real register of daily practice. However, these results show, a priori, that Stress CMR can detect even small ischemic lesions (very good detector of myocardial ischemia). This ischemia probably corresponds to small coronary artery lesions or very distal lesions for which a revascularization procedure is not necessarily indicated.
In The ISCHEMIA trial (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) included over 5,000 patients with stable coronary artery disease and moderate to severe myocardial ischemia, no differences were found in relevant clinical outcomes, including all-cause mortality, cardiovascular death, myocardial infarction (MI), heart failure and stroke, over a follow-up of 3.2 years (9).
The interim report of the ISCHEMIA-EXTEND study shows that there was no difference in all-cause mortality in 7 years, but there was a lower risk of 7-year cardiovascular (CV) mortality and a higher risk of non-CV mortality with the initial invasive strategy when compared with the initial conservative strategy (10). The higher rate of non-CV death in the invasive group was unexpected and remains unexplained, deserving further investigation. Overall, the trial’s extended follow-up provides much more robust evidence for the neutral effect on survival of the two strategies. When the ISCHEMIA trial was first designed, the goal of the trial was to determine whether a catheter-based strategy could ultimately reduce CV events like CV mortality and MI, and this seems to be the case: spontaneous MI at the earlier and CV death at the later time point being reduced by this strategy (10).
Our results show that Stress Echo can detect, when the test is positive, more severe coronary lesions, probably more proximal, which are more amenable to a revascularization procedure. In practice, Stress Echo is a “good detector” of myocardial ischemia while Stress CMR is a “very good detector” of myocardial ischemia. Stratification by stress CMR in our study according to the presence of ischemia and/or LGE and at the same time according to the follow-up by coronary revascularization or not (Figure 5) could have interesting consequences to know on the occurrence of MACE in the future.
The EVAREST study provides UK-wide data to evaluate “real-world” performance and accuracy of stress echocardiography (13). Stress echocardiography has high accuracy across UK-based hospitals and thus indicates stress echocardiography is being delivered effectively in real-world practice, reinforcing its role as a first-line investigation in the assessment of patients with stable chest pain. Stress echocardiography is widely used to identify obstructive coronary artery disease (13).
In the management of coronary patients, the choice between the two techniques is linked, in our practice, to the availability of the technique and to the patient's coronary history. For Stress Echo, in our registry, many patients were at high cardiovascular risk with little coronary history. While the population of patients who had a stress CMR was mainly with a coronary history. This heterogeneity of the two populations, Stress Echo and Stress CMR, reflects a real image of the patients encountered in practice without exclusion criteria. In a future analysis of the follow-up of these patients, it will be interesting to see the evolution of the MACE in each group according to the choice of screening test.
for the PROMISE Investigators (14), in symptomatic patients with suspected coronary artery disease (CAD) who required noninvasive testing, a strategy of initial Coronary Computed Tomography Angiography, as compared with functional testing (exercise electrocardiography, nuclear stress testing, or stress echocardiography), did not improve clinical outcomes over a median follow-up of 2 years.
Generally, many specific criteria for inclusion and/or exclusion of randomized patients in many studies could modify their impact on the reality experienced by most patients. In the PROMISE study (14), additional inclusion criteria were an age of more than 54 years (in men) or more than 64 years (in women) or an age of 45 to 54 years (in men) or 50 to 64 years (in women), exclusion criteria were an unstable hemodynamic status or arrhythmias that required urgent evaluation for suspected acute coronary syndrome, a history of CAD or evaluation for CAD within the previous 12 months, or clinically significant congenital, valvular, or cardiomyopathic heart disease, or any reason that the patient could not be randomly assigned to either group safely.
we hope by “Nancy ischemia register” to be simpler and cover many patients.
For the management of coronary artery disease, when we receive a patient, it is imperative to make the most precise decision that brings us as close as possible to the diagnosis, and as quickly as possible. In all randomized studies, patient care is based on several inclusion and exclusion criteria to optimize the decision as much as possible. We are far from the real situation where the decision must be simpler and more practical. Our register tries to be more real and closer to current practice. However, in trying to be real, our patient data is less comprehensive and accurate. The groups of patients with different screening techniques for myocardial ischemia are heterogeneous (age, sex, coronary ATCD, medication, ...).
“Nancy Ischemia Register” is an ambitious work that brings together different screening techniques for myocardial ischemia. this registry attempts to cover most patients likely to present with myocardial ischemia in a real context and outside of randomized studies with numerous inclusion and/or exclusion criteria.
In its first phase of the register, the Stress CMR seems in real conditions more sensitive than the Stress Echo in detecting myocardial ischemia. However, Stress Echo appears to be more sensitive in detecting larger coronary lesions that further require myocardial revascularization.
In the next phases of “Nancy Ischemia Register”, we will see the impact of other anatomical imaging techniques (CTCA, CACS). We performed 2116 CT coronary angiogram and 1581 coronary artery calcium score in patients at “high” cardiovascular risk. The actual comparison between the different techniques could be very interesting.
In the last phase, we record MACE occurring in all 4553 patients during the years 2022-2023-2024. we compare groups and MACE according to:
1- the presence of myocardial ischemia or not, 2- Revascularization or not, 3- technique used for screening for myocardial ischemia. The comparison of MACE according to the initial examination (positive or negative) could have consequences on the choice of a particular technique as a means of detecting myocardial ischemia at the start of our investigations.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
