
Review article | DOI: https://doi.org/10.31579/2641-0419/221
1High Specialty Resident in Advanced Hand Procedures at Hospital Ángeles Pedregal. Mexican School of Medicine La Salle University. Mexico City, Mexico.
2Hand Surgeon at Hospital Ángeles Pedregal. Mexico City, Mexico.
3Plastic and Reconstructive Surgery Resident. Hospital Central Sur de Alta Especialidad Petróleos Mexicanos. Mexico City, Mexico.
4General Surgery Resident at Hospital Ángeles Pedregal. Mexican School of Medicine La Salle University. Mexico City, Mexico.
*Corresponding Author: Jorge Eduardo Molina Ortega. Brigadeiro Faria Lima, 5416, Vila São Pedro, CEP: 15.090-000, São José do Rio Preto, SP, Brasil.
Citation: Molina Ortega JE., Carlos G. Orvañanos., Campos Serna EI., Concha Tiznado MDL. (2021) Stenosing flexor tenosynovitis of the hand
(trigger finger). J. Clinical Cardiology and Cardiovascular Interventions, 4(17); Doi:10.31579/2641-0419/221
Copyright: © 2021 Jorge Eduardo Molina Ortega, This is an open-access article distributed under the terms of the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 September 2021 | Accepted: 14 September 2021 | Published: 20 September 2021
Keywords: trigger finger; algorithm; treatment
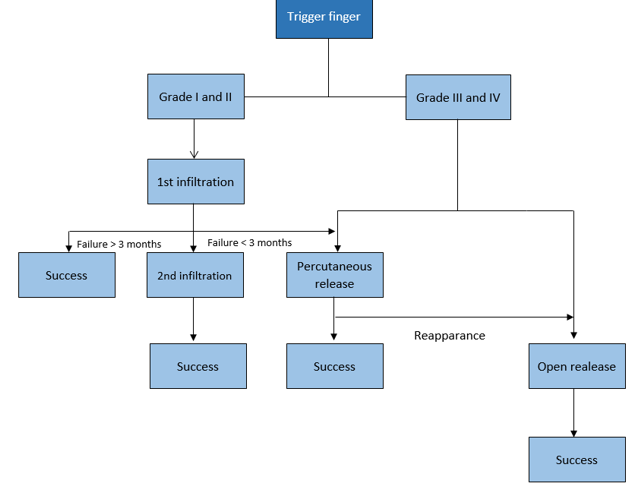
Trigger finger is the second cause of consultation with the hand surgeon. In 2009, Kerrigan published a strategy for the treatment of this pathology, which consists of two infiltrations with corticosteroids in the sheath of the flexor tendons at the level of the A1 pulley, followed by percutaneous or open surgical release, following the algorithm described by the author. 140 files that met the inclusion criteria were analyzed. It was found that the female gender is the most frequently affected during the sixth decade of life in 46%. The most frequently affected finger is the third, affects the right hand in 44% and both hands in 29%. 91% of the patients received a first infiltration and only 31% of these received a second infiltration. The surgical procedure was decided in 33% of the patients. The longest follow-up was 180 months and the shortest was 3 months with 100% of asymptomatic patients. The algorithm proposed by Kerrigan in the treatment of this pathology is a good strategy that has a high success rate without having to perform a surgical procedure as the first treatment option.
Stenosing flexor tenosynovitis of the hand, better known as trigger finger, is one of the main causes which leads to pain and the inability to use one’s hand. The tendon entrapment phenomenon is due to the mechanical pinching of the finger flexor tendons when they pass through a narrow retinaculum pulley located at the head of the metacarpal. [1-3]
The most common trigger finger shape is primary shape, which is found in middle-aged females, usually healthy, and with a frequency of two to six times greater than in males. [1,2,4,5] Thumbs are the most frequently affected finger, followed by the ring, middle, little, and index fingers. Secondary type stenosing tenosynovitis can be observed in patients with Mellitus diabetes, gout, renal diseases, rheumatoid arthritis and other rheumatic diseases. [6-8]
In fingers, each flexor tendon passes through a series of narrow fibro-osseous tunnels which serve to optimize balance between movement and the production of power to maintain the tendon in close apposition to the articulations which it controls. [1-3] The tendon entrapment phenomenon is due to the mechanical pinching of the finger flexor tendons when they pass through a narrow retinaculum pulley located at the head of the metacarpal. [1-3]
The most outstanding pathological changes in the pulleys show macroscopic hypertrophy.
The microscopic examination of such reveal degeneration, the formation of cysts, fiber division and lymphocyte and plasma cell infiltration. [9] There is also the presence of chondrocytes in the innermost or friction layer of the pulleys. Normal A1 and the proliferation of chondrocytes and the presence of type III collagen in thickened pulleys. That is, fibrocartilaginous metaplasia under the influence of repetitive compressive loads. [3]
Thumbs are the most frequently affected finger, followed by the ring, middle, little, and index fingers. 5
Secondary type stenosing tenosynovitis can be observed in patients with Mellitus diabetes, gout, renal diseases, rheumatoid arthritis and other rheumatic diseases, and it is associated with a worse prognosis after surgical or conservative treatment. [7-9]
The incidence of trigger finger throughout life in non-diabetic adults over 30 years of age is 2.2% and can reach up to 10% among insulin dependent adults with Mellitus diabetes. [9-11]
surgical treatment has negative results in 7 to 9% of cases, resulting the nerve injury, infection, incision pain, flexion deformity, bowstring deformity in the flexor tendon and recurrence. [1,8,12-14]
The injection of corticosteroids is quite successful, especially among non-diabetic patients with only one affected finger, one nodule, one defined palpable nodule and recent symptoms. [15,16]
Although a relationship cannot be made between a corticosteroid and pulley rupture, all authors recommend not performing the injection of intratendinous corticosteroids upon knowing the wear effect they have on collagen fibers.
Due to the inhibition in wound healing theory, it is advisable to wait at least six weeks after the injection of corticosteroids before considering open surgical release. [8]
Throughout the past 10 years, and with the use of the algorithm proposed by Kerrigan and Stanwix, we have treated 140 patients, 46 of which required surgery (Tables 1 and 2).



The use of the protocol has resulted in an adequate treatment for stenosing flexor tenosynovitis of the hand, which has the advantage of being a clear and easy strategy to follow (Annex 1).
Furthermore, it reduces costs while increasing benefits for patients. Moreover, it contributes toward lowering the complication rates which arise when following other treatment strategies mentioned by other authors.
Most primary trigger finger cases can be treated successfully without surgery, which has also been our experience. Some authors have documented that
Disclosure: The authors declare no benefits in any form have been received or will be received related directly or indirectly to the subject of this article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
