
Case Report | DOI: https://doi.org/10.31579/2692-9406/033
*Corresponding Author: Tibor Hajto MD, PhD, Meggyes u 26, H-2045 Törökbálint, Medical University Pecs, Sziget u. 12, H-7624 Pécs, Hungary.
Citation: T Hajto. (2020) Standardized Plant Immunomodulator Increases the Effect of MEK and BRAF Inhibitors with Clinical Benefit. Case Report of a Patient with Carcinoma in Biliary Duct. Biomedical Research and Clinical Reviews. 1(5); DOI:10.31579/2692-9406/033
Copyright: © 2020 Tibor Hajto, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 November 2020 | Accepted: 28 November 2020 | Published: 04 December 2020
Keywords: mek-inhibitor; dabrafenib; braf-inhibitor; trametinib; immunomodulatory treatment; tumor disease; rice bran arabinoxylan
Background: Targeting hyperactive mitogen-activated protein kinase (MAPK) signaling cascade has proven to be an effective treatment for a variety of different cancers. Using an important member of this cascade, namely MEK (mitogen-activated extracellular signal regulation kinase) inhibitors, the clinical responses are often transient and complete remission is rarely observed. It was shown that growth factor receptor signaling pathway inhibitors can increase the immune sensitivity of tumor cells but they can’t activate the down regulated immune effectors. Consequently, the combination of MAPK cascade signaling pathway inhibitors and the immune effectors activating immunomodulators may be a promising new strategy.
Material and Methods: In a now 59 years old patient with inoperable (BRAF-mutant) low differentiated adenocarcinoma of biliary ducts after 30GY radiotherapy and two cycles (Gemcitabin+ Cisplatin) chemotherapy a rapid progression of lung, liver and brain metastases were by CT and MR established. A treatment was tarted with BRAF+MEK inhibitors (2x150 mg dabrafenib and 1 x 2 mg trametinib). These inhibitors were combined with daily 45 mg/kg rice bran arabinoxylan concentrate (using Biobran/MGN-3) which was shown to be a pathogenic associated molecular pattern (PAMP)-like molecule and can stimulate the type-1 innate immune cells against tumor cells.
Results: After the chemotherapy and before the start of second-line treatment, the patient had a nearly terminal state of her rapidly progressive disease. Eight months after the combination of MEK / BRAF inhibitor and immunomodulator therapy nearly complete remissions of all metastases were established in CT and MR.
Conclusion: This case report may support a hypothesis that MEK/BRAF inhibitors and type-1 immune cells activating immunomodulators together may synergistically inhibit the tumor growth. Further clinical investigations are necessary to clarify this question.
Abbreviations:
MEK = Mitogen Activated Extracellular Signal; MAPK = Mitogen Activated Protein Kinase; MHC = Major Histocompability Complex; M1 and M2 = type-1 and 2 macrophages; D1 and D2 =type-1 and 2 Dentritic cells; KAR (NKG2D) = Killing Activator Receptor; CEA = Carcinoembryonic antigen; WBRT = whole body radiotherapy; MICA and MICB = MHC-Class-I Cain-related protein-A and B; ULBP = UL-16 binding proteons,
MEK (Mitogen-activated Extracellular signal regulation Kinase) – inhibitors can down- regulate the receptor tyrosine kinase-mediated signaling pathway by inhibition of mitogen activated protein kinase /MAPK/ cascade (RAS/RAF/MEK/ERK) which regulates cell proliferation, cell cycle progression and cell migration. Dysregulation of the MAPK cascade occurs in more than one-third of all malignancies, a process that has fostered the development of targeted MAPK pathway inhibitors [1]. Owing to the widespread activation of this pathway in numerous neoplasms, MEK inhibitors are being studied in combination with other targeted and cytotoxic drugs in a variety of clinical situations [2-4]. MEK inhibitory compounds demonstrated markedly enhanced potency against BRAF (V600E) cancer cells compared to cell lines lacking this oncogenic pathway mutation. In addition, MEK and BRAF inhibitors exhibit a synergistic effect [5].
Despite the improved outcomes with monoclonal antibodies targeting various members of the MAPK cascade, durable clinical responses are uncommon. An outgrowth of resistant clones within progressed tumors appears inevitable [6]. Recent immunological and clinical observations suggest that in the background of this resistance at least in part the tumor-.induced disturbance of immunoregulation may play also a role. In spite of an enhanced sensitivity of tumor cells for immunological killing induced by targeted MAPK pathway inhibitors [7-˙8] the most important immune effector cells against tumors are parallel not activated.
As it is well known, tumor cells are definitively able to escape from the T cell lyse since they exhibit genetic dysregulation related to irreversible quantitative and qualitative alterations of their MHC-I antigens [9]. Consequently, growing attention is focusing on the mechanisms of the innate immune system which are able to kill tumor cells in a non-MHC-restricted manner and appear to exhibit more reversible escape mechanisms if it is compared with the adoptive system. As known, the effector cells of innate immune system are committed in two directions. Type-1 macrophages (M1) and from the monocytes originating type-1 dentritic cells (D1) generate (in a rigorously regulated cascade system only for short time) proinflammatory cytokines, IL-12 and activate cytotoxic effector (such as NK and NKT) cells which are potent inhibitors of tumor growth. However, these type-1 cells are defective in tumor patients. Available information suggests that tumor-associated macrophages belong to the prototypic M2 population [10-11]. M2 macrophages and from the plasmocytoid precursors originating D2 dentritic cells generate IL-4 and IL-10 which facilitate the generation of Th2 cells and inhibit Th1 cells and the type-1 natural system [10]. M2 macrophages and D2 dentritic cells affect chronic inflammation, promote cell proliferation by producing growth factors and stimulate angiogenesis. Tumor patients can have up to 40% M2 peripheral monocytes and healthy individuals have only 10% M2 monocytes [10-11].
As it was mentioned, the dominance of M2 and D2 cells in tumor patients can lead to an enhanced production of growth factors which are also contribute to the down regulation of the type-1 natural immune cells. It was shown that growth factors can inhibit the NK cytotoxicity against cancer cells by down regulating the expression of the so called stress- related receptors on the surface of tumor cells, namely the Killing Activator Receptor (KAR) binding NKG2D ligands such as UL-16 binding proteins (ULBP1 and ULBP2) or MICA and MICB [7-8]. Taken together these observations we can conclude that targeted MAPK pathway inhibitors can enhance the sensitivity of tumor cells against immune effectors but they are not able to activate them. Therefore the hypothesis is arisen as to whether immunomodulators, which are able to activate the (type-1) immune effectors against tumor cells, may improve the effects of the targeted MAPK pathway inhibitors. In this paper a case report is presented which may support this hypothesis. A patient with inoperable (BRAF-mutant) low differentiated adenocarcinoma of biliary ducts with lung, liver and brain metastases was treated with a combination of MEK and BRAF inhibitors together with evidence based and standardized plant immunomodulator (BioBran/MGN-3) which was shown to stimulate the type-1 natural immune cells. After four months all metastases showed a nearly complete remission which after 8 months were also established.
MEK and BRAF inhibitors
As MEK inhibitor 1 x 2 mg trametinib and as BRAF inhibitor 2x150 mg dabrafenib were given from July 4th 2016 regularly until March 2017 (observation period). The patient was regularly controlled by CT and MR investigations by the Oncological Department of Medical University Debrecen (Hungary).
Standardized Rice Bran Extract (BioBran/MGN-3)
The immunomodulatory drug used in the combinative treatment of the presented patient is BioBran/MGN-3 which is manufactured and supplied by Daiwa Pharmaceutical Co, Ltd, Tokyo, Japan. BioBran/MGN-3 is composed of denaturated hemicellulose, which is obtained from rice bran hemicellulose reacting with multiple carbohydrate-hydrolyzing enzymes from shiitake mushrooms. BioBran/MGN-3 is standardized for its main chemical component: arabinoxylan with a xylose (in its main chain) and with an arabinose polymer (in its side chain). To the presented patient BioBran/MGN-3 was given orally in doses of 45mg/kg at first daily and four months later three times a week.
Ethics committee
Ethics committee proposed to observe and publish case reports of own patients treated with standardized plant immunomodulators. The patient has given an informed consent to process and publish her dates. This case report may stimulate an interest for other research groups according to the opinion of the ethics committee.
Results
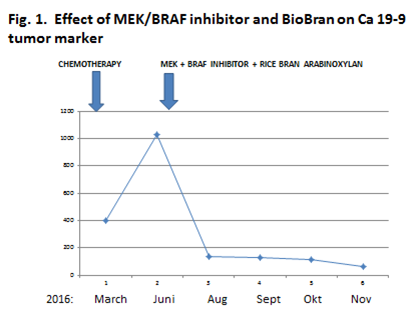
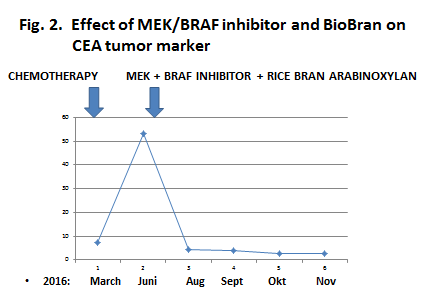
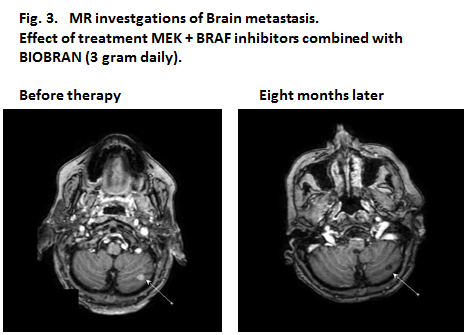
A now 59-year-old patient with inoperable low differentiated adenocarcinoma of biliary ducts had in April 2016 a terminal stage of her disease. By PET/CT investigations multiplex metastases were established in the following organs: lung (S3), bilateral mediastinal, paraaortal, paratracheal, subcarinal, subclavicular lymph nodes, pancreas, hilus of liver and mesenterium. In addition, four brain metastases (three in cerebellum and one in temporal region) were detected by MR investigation. After an irradiation (30 GY WBRT), in Mai/June 2016 two of Cisplatin and Gemcitabin were given. At end of June 2016 progressions of all metastases were established and therefore the chemotherapy was stopped. Since by the genetic investigation 15% BRAF (V600E) clinical relevant driver mutation and 22% TP53 (Q16fs*28) clinical relevant driver mutation were found, at begin of July 2016 1 x 2 mg trametinib MEK inhibitor and 2x150 mg dabrafenib BRAF inhibitor were given. At the same time an immunomodulatory treatment was started with a standardized bran rice arabinoxylan concentrate (BioBran/MGN-3) in doses of 3 g daily for four months and thereafter three times 3 g a week. During this combinative therapy a very rapid remission of all metastases was observed. Figure 1 and 2 show the rapid decreases in tumor markers (CEA and CA19-9) in peripheral blood. After four and eight months nearly complete remissions (CR) of all metastases were also established by CT and MR investigations. Figure 3 represents a CR of a brain metastasis prior the treatment and eight months later.
The effect of the immune system on the inhibitory targeting therapy of the tyrosin kinase-mediated signaling pathway is poorly understood since very few research results are now available. Although signaling pathways are usually depicted as linear cascades, nearly all signaling pathways are highly interconnected and form networks that allow dynamic regulation of the timing, strength and duration. In addition, both feed forward and feed-backward loops provide the means to self-regulation signals. As a consequence, the same signal may induce different outcomes depending on the particular cell state. Consequently, they can inhibit or stimulate in different cells [6]. Interestingly, it appears to be a similarity between the regulation of MAPK cascade and the regulation of natural immunity. As it was mentioned above, the effector cells of the innate immune system are also committed in two directions [10-11] which also in the cascade system can play an important role in the activation and inhibition of cell proliferation. Both protein kinase signaling pathway and innate immunity exist in a basal state and they are activated only if it is necessary by divergent regulation stimuli [12-13]. The mechanisms for switching between dormant and activate state in both systems can be intricate, but it is probable that both signaling pathways are highly interconnected and form networks. Therefore, it is not surprising that growth factors stimulate the cell proliferation on the one hand and protect the cells (downregulating their ligands) against immune effectors on the other hand inducing a decrease in tumor defense.
Consequently, a combination of protein kinase signaling pathway inhibitors and natural effector cells activating immunomodulators may open new perspectives in the tumor therapy. This case report may support this hypothesis. However, in the future we must better learn to manipulate the regulatory networks, and the timing, strength and duration of responses must be taken with more attention into consideration. For example, the stronger a response, the less possible to give a drug daily, since therapy free intervals can be necessary [13-14].
Pathogenic Associated Molecular Pattern (PAMP) molecules are the best candidates for this combination of targeting therapy with immunomodulation. However, PAMP molecules exist only in the nature (bacteria or plants). The chemistry is not able to produce these configurations. Bacteria have toxic side effects but plants have not. Unfortunately, the best evidence-based and standardized immunomodulators without any side effects are plant extracts and they are all over the world registered only as food supplements. There is growing evidence that plant PAMP-like molecules (such as standardized rice bran arabinoxylan concentrate) exhibit a lot of immunological [15-26] and clinical benefit [27-29]. Therefore further clinical trials are necessary to investigate this beneficial interaction.
Conclusion
This case report may support a hypothesis that MEK / BRAF inhibitors and type 1immune cells activating immunomodulators together may synergistically inhibit the tumor growth. Further clinical investigations are necessary to clarify this question.
Conflict of interest
The authors declare that there is no competing or other conflicting interest in relation to this paper.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
