
Research Article | DOI: https://doi.org/10.31579/2690-8816/135
Adventist Health Services, Blantyre, Malawi.
*Corresponding Author: Fyson Kasenga, Adventist Health Services, Blantyre, Malawi
Citation: Fyson Kasenga, (2024), Staff Motivation: A Case of Adventist Health Services in Rural Malawi, J Clinical Research Notes, 5(4); DOI:10.31579/2690-8816/135
Copyright: © 2024, Fyson Kasenga. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 July 2024 | Accepted: 15 August 2024 | Published: 30 August 2024
Keywords: health services; staff motivation; nurses; health care provider
Human resource is a backbone of any given organization regardless of where it is located, originality and economic base among others. Essentially an organization has a life span equated to that of a human being with various body parts as structures let alone with a culture. Just as an automobile engine cannot move without gasoline, so is the same with an organization which cannot function without human beings. According to Shearer, 2012, a motivation theory such as Herzberg and Maslow enhance employees' motivation, morale, and satisfaction. A manager has ability to motivate, empower, and influence staff to improve satisfaction and retention levels among the team. Therefore, educational development and organizational culture influence leaders in managing an organization. Organizational culture has an impact on a manager's style, which is forwarded to their followers and this impact can be positive or negative.
Human resource is a backbone of any given organization regardless of where it is located, originality and economic base among others. Essentially an organization has a life span equated to that of a human being with various body parts as structures let alone with a culture. Just as an automobile engine cannot move without gasoline, so is the same with an organization which cannot function without human beings. According to Shearer, 2012, a motivation theory such as Herzberg and Maslow enhance employees' motivation, morale, and satisfaction. A manager has ability to motivate, empower, and influence staff to improve satisfaction and retention levels among the team. Therefore, educational development and organizational culture influence leaders in managing an organization. Organizational culture has an impact on a manager's style, which is forwarded to their followers and this impact can be positive or negative.
Why motivation? Very important to relate the fact that the urge or a triggering factor to do something be investigated and established so as to reward it so long it brings up a desired outcome. In the event that unpleasant outcome comes up, reinforcement of some kind should be explored and used to determine the desired goal. There are times that much is done in the form of various rewards to determine the nature of results, only to realize that nothing happens but same results are yielded despite change of the reinforcement methods, then more needs to be done. Motivation represents the degree in which a persistent effort is focused to achieve a certain goal. Managers, including health managers, are especially interested about motivation, due to the direct relation with productivity (Duma, 2003). Therefore, staff motivation is vital as reported before (Kasenga and Hurtig, 2014).
There are various means of motivating people to achieve set goals. More often than not, money is regarded as the primary reason why people work so hard in an organization but this cannot be regarded as such. To some people by just getting an employment regardless of how much they earn, in itself constitutes motivation. A study done before (Ilies et al, 2017) revealed that employees' daily work engagement experiences related positively, within individuals, to work-family interpersonal capitalization, which in turn, related positively related to daily family satisfaction and to daily work-family balance. This entails that doing something on daily basis has multiple health benefits regardless of official employment or not and these benefits can be manifested during and after work life. The income one gets during work, relationship with people at work and respect that one is working among others are some of the benefits. Consequently, when people retire from work, they enjoy retirement benefits, look back and see the contribution made during their working life though this can be argued if they earned a successful retirement. In a study done by Britt et al, (2001), it was established that structural equation modeling revealed that personality hardiness was associated with being engaged in meaningful work during the deployment, which was strongly associated with deriving benefits from the deployment months after it was over. Enriching experiences were also associated with deriving benefits from the deployment.
This paper aims at establishing what works well and what does not in the 16 clinics of Adventist Health Services across Malawi in order to optimize the performance of the service delivery, bridge the gaps and improve patients care and satisfaction.
Methods
This was operational research which utilized qualitative and quantitative methods. The researcher is the Chief Executive Officer (CEO) of Adventist Health Services (AHS) which is owned by the Seventh Day Adventist Church in Malawi and is based at the Secretariat, Blantyre, Malawi. He has a responsibility of ensuring that the clinics under AHS are well managed and the general population within the clinics is well looked after. The Seventh Day Adventist (SDA) Church in Malawi offers various services in the country ranging from education, humanitarian services, publishing, health as well as spiritual nourishment as a primary goal.
Study area
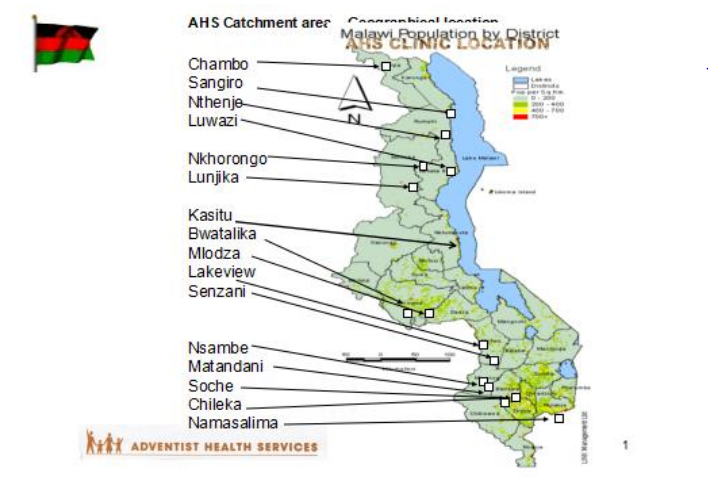
Adventist Health Services (AHS) is an organization of the Malawi Union Conference of the Seventh-day Adventist Church that currently operates a network of 16 clinics doing preventive, curative and supportive work in the health sector. These clinics are located in all the three regions of Malawi. In the northern region AHS has 6 clinics as follows; Nkhorongo in Mzuzu and Lunjika in Mzimba district, Luwazi in Nkhatabay district, Nthenje in Rumphi district, Sangilo in Karonga district and Chambo in Chitipa district. In the central region AHS has 5 clinics as follows; Kasitu in Nkhotakota district, M’bwatalika and Mlodza in Lilongwe district, Lakeview and Senzani in Ntcheu district. AHS in the southern region has 5 clinics as follows; Soche and Chileka in Blantyre district, Namasalima in Mulanje district, Matandani and Nsambe in Neno district.
3. Map showing Adventist Health Services clinics’ locations
4.Adventist Health Services purpose for existence
4.1 Purpose
Adventist Health Services exist to attain and sustain healthy, spiritual and productive communities in areas where it is serving.
4.2 Vision
To be the Health Care Provider of choice in the communities served by Adventist Health Services.
4.3 Mission statement
To promote and provide wholistic, quality, integrated preventive, curative and supportive health services to communities served in line with the principles of the Seventh-day Adventist Church.
4.4 Core values
God fearing,Team spirit, Integrity, Transparency, Accountability, Unity and Empathy
5. Goals:
5.1 To promote good health seeking behaviors amongst men and women.
5.2 To provide quality curative services in Adventist Health Services facilities.
5.3 To promote spiritual and supportive services.
5.4 To establish financial sustainability.
5.5 To retain qualified, competitive and dedicated staff at all levels.
5.6 Target Audience
Adventist Health Services serves both rural and urban communities. However, most of the facilities are situated in the rural communities to meet health needs of the huge population in remote and hard to reach communities. AHS takes into account all demographic factors in its health service delivery. It considers the socioeconomic characteristics of the population it serves regardless of age, sex, education level, income level, marital status, occupation, religion, birth rate, death rate, average size of a family and ethnic backgrounds among others.
5.7 Workforce:
AHS has a total workforce of 226 employees comprised of skilled and non-skilled employees. A total catchment population of 426,719 is served by AHS through its 16 clinics. The qualifications of employees range from degrees to Primary Leaving Certificates.
5.8 AHS facility location, catchment population, services being offered and a list of partners working with the organization
| CLINIC NAME AND LOCATION | DATE ESTABLISHED | NO. OF BEDS | STAFFING | SERVICES OFFERED | 2022 STATISTICS | PARTNERSHIP |
|---|---|---|---|---|---|---|
Chambo Clinic in Chisenga, Chitipa District
Population of 16,563 | 1954 | 27 | Clinician: 1
Medical Asst: 1
Nurse/midwife: 2 Support staff: 8
|
| 19,377 | Ministry of Health (MoH) at District Health Office (DHO) level. Note: Adventist Health Services (AHS) is providing free healthcare services to the general population under the Service Level Agreement (SLA) signed between AHS and the MoH through the DHO. Of the 16 AHS health centres, it is 10 of them that serve the communities through the service level agreement (SLA). |
Sangilo Clinic, South of Karonga District
Population of 12,745 | 1964 | 18 | Medical Asst: 1
Nurse/ Midwife: 3
Support staff: 8 |
| 5,038 | Onse Project through Karonga DHO-
Ministry of Health at District Health Office level. |
Nthenje Clinic, Rumphi District
Population of 6,471 | 1960 | 8 | Clinician: 1
Nurse/ Midwife: 1
Support staff: 5
|
| 3,471 | Ministry of Health at District Health Office level.
|
Luwazi Clinic, Nkhatabay District
Population of 10,807 | 1982 |
6 | Clinician: 0 Medical Asst: 1
Nurse/ 1 Midwife: 2
Support staff: 7 |
| 4,496 | Ministry of Health at District Health Office level. Note: Adventist Health Services is providing free healthcare services to Under-five population and Maternal mothers under the Service Level Agreement (SLA) signed between AHS and the Ministry of Health through the District Health Office. |
Nkhorongo Clinic, Mzuzu
Population of 20, 603 | 1979 | 6 | Clinician: 1
Medical Asst: 1 Nurse/ Midwife: 4 Lab Asst: 1 Support staff: 10 |
| 15,355
| Ministry of Health @ District Health Office level. Note: Adventist Health Services is providing free healthcare services to Under-five population and Maternal mothers under the Service Level Agreement (SLA) signed between AHS and the Ministry of Health through the District Health Office. |
Lunjika Clinic, Eswazini in Mzimba District.
Population of 15,300 | 1962 | 20 | Clinician: 1
Medical Asst: 2
Nurse/ Midwife: 3 Support staff: 8 |
| 11,582 | NCA through CHAM. Ministry of Health at District Health Office level. Note: Adventist Health Services is providing free healthcare services to Under-five population and Maternal mothers under the Service Level Agreement (SLA) signed between AHS and the Ministry of Health through the District Health Office. |
Kasitu Clinic in Nkhotakota District
Population of 14,778 | 1993 | 16
| Clinician: 1
Nurse/ Midwife: 2 Support staff: 5
|
| 5,339 | Ministry of Health at District Health Office level.
|
Mbwatalika Clinic, Mpingu area Lilongwe District
Population of 25,187 | 1985 | 20 | Clinician: 1
Medical Asst: 2
Nurse/ Midwife: 5
Support staff: 8 |
| 13,685 | Norwegian Church Aid (NCA) through Christian Health Association of Malawi (CHAM)
Ministry of Health at District Health Office level. |
| Mlodza Clinic, Lilongwe urban Population of 50,748 | 1994 | 2 | Clinician: 1 Nurse/ Midwife: 2
Lab Asst: 1
Support staff: 6 |
| 3,234 | Ministry of Health @ District Health Office level. |
Lakeview Clinic, Ntcheu District
Population of 9,541 | 1937 | 15 | Clinician: 1
Medical Asst: 1
Nurse/ Midwife: 4 Lab Tech: 1 Support staff: 8 |
| 8,893 | Egpaf – Provide support in HIV & ART – Training & mentorship. Ministry of Health at District Health Office level. Note: Adventist Health Services is providing free healthcare services to Under-five population and Maternal mothers under the Service Level Agreement (SLA) signed between AHS and the Ministry of Health through the District Health Office. |
Senzani Clinic, Ntcheu District
Population of 20,159 | 1980 | 9 | Medical Asst: 1
Nurse/ Midwife: 3
Support staff: 8 |
| 4,662
| Ministry of Health at District Health Office level. Note: Adventist Health Services is providing free healthcare services to Under-five population and Maternal mothers under the Service Level Agreement (SLA) signed between AHS and the Ministry of Health through the District Health Office. |
Soche clinic, Soche township, Blantyre District.
Population of 145,820 | 1962 | 7 | Clinician: 2 Nurse/ Midwife: 5
Lab Tech: 1
Lab Asst: 1 Support staff: 8 |
| 7,647 | Egpaf - Provide support in HIV & ART. Ministry of Health at District Health Office level. |
Chileka Clinic, Blantyre rural District.
Population of 26,725 | 1973 | 8 | Medical Asst: 1
Nurse/ Midwife: 3
Lab Asst: 1
Support staff: 9 |
| 4,361 | Egpaf - Provide support in HIV & ART.
Ministry of Health at District Health Office level.
|
Namasalima Clinic, Mlodza area in Mulanje District
Population of 24,472 | 1987 January | 10 | Clinician: 1 Medical Asst: 1 Nurse/ Midwife: 5 Lab Tech 1 Support staff: 11 Pharmacy Asst: 1 |
| 18,790 | Baylor – Support HIV services. One community – support in HIV clients follow-up Ministry of Health at District Health Office level. Note: Adventist Health Services is providing free healthcare services to Under-five population and Maternal mothers under the Service Level Agreement (SLA) signed between AHS and the Ministry of Health through the District Health Office. |
Matandani Clinic, Neno District
Population of 10,443 | 1940
| 7 | Medical Asst: 1
Nurse/ Midwife: 3
Support staff: 8
|
| 21,991 | Partners in Health (PIH) & The (Neno) District Health Office. Note: Adventist Health Services is providing free healthcare services to the general population. |
Nsambe Clinic, Neno District.
Population of 16,357 | 1982 | 6 | Clinician: 1 Nurse/ Midwife: 3 Support staff: 8
|
| 21,279 | Partners in Health (PIH) & The (Neno) District Health Office. Note: Adventist Health Services is providing free healthcare services to the general population. |
5.9 Sampling informants
Based on the theoretical assumption that there were variations and range of understanding on different areas, informants were therefore purposely selected. The participants were selected based on their roles, years of service, experiences, sex and age-groups. The clinic managers facilitated the selection and each participant was given a choice to participate or not.
5.9.1 Data collection
A total of 42 participants were interviewed using a structured questionnaire based on years of work, age, sex and occupation. At least one member from each section of the clinic participated in the interviews.
Distribution of Various Socio-Demographic Variables
| Males | Females | Total | |||
| No | % | No | % | No | % |
| 23 | 54.8 | 19 | 45.2 | 42 | 100 |
Table 1: Gender (N = 42)
Majority 23 (54.8%) of respondents were males
(a) Age group (in years) | Respondents | |
| No | % | |
| 15 - 24 | 2 | 4.8 |
| 25 - 34 | 10 | 23.8 |
| 35 - 44 | 11 | 26.2 |
| 45 - 54 | 15 | 35.7 |
| 55 -64 | 3 | 7.1 |
| 65 and above | 1 | 2.4 |
| Total | 42 | 100 |
| (b) Marital status | ||
| Married | 32 | 76.2 |
| Single | 6 | 14.2 |
| Divorced | 2 | 4.8 |
| Widowed | 2 | 4.8 |
| Total | 42 | 100 |
| (c) Educational levels | ||
| Primary (Classes 1 - 8) | 8 | 19.1 |
| Secondary | 20 | 47.6 |
| Post-Secondary | 14 | 33.3 |
| Total | 42 | 100 |
Table 2: Sex and age distribution (N=42)
A total of 15 (35.7%) respondents were in the age group of 45 - 54 followed by those 11 (26.2%) in the age group of 35 - 44.
| Worked before | Not worked before | Total | |||
| No | % | No | % | No | % |
| 18 | 42.9 | 24 | 57.1 | 42 | 100 |
Table 3: The staff members who worked before joining AHS or not (N = 42)
A total of 18 (42.9%) of employees worked elsewhere before joining AHS
Work experience in years | Respondents | |
| No | % | |
| 1 - 5 | 8 | 19.1 |
| 5 - 9 | 19 | 45.2 |
| 10 - 14 | 5 | 11.9 |
| 15 - 19 | 3 | 7.1 |
| 20 - 24 | 3 | 7.1 |
| 25 - 29 | 2 | 4.8 |
| 30 - 34 and above | 2 | 4.8 |
| Total | 42 | 100 |
Table 4: Years of work experience (N = 42)
At least 19 (45.2%) of the respondents had work experience of 5 - 9 years
What is liked most by AHS staff | Respondents | |
| No | % | |
| Mopping the floor | 4 | 9.5 |
| Dispensing drugs and supplies | 3 | 7.1 |
| Having friendly workmates | 11 | 26.2 |
| Delivery of good services | 9 | 21.4 |
| Time to worship God | 8 | 19.1 |
| Profession | 7 | 16.7 |
| Total | 42 | 100 |
Table 5: What the staff liked most at the work place
Majority of respondents 11 (26.2%) liked friendship at workplace followed by those 11 (21.4%) who liked the delivery of good services
What the staff do not like | Respondents | |
| No | % | |
| Shortage of staff | 16 | 38.1 |
| Absent from duties | 6 | 14.3 |
| Poor working environment | 5 | 11.9 |
| Delayed salaries | 10 | 23.8 |
| Poor communication | 3 | 7.1 |
| Stealing clinic supplies | 2 | 4.8 |
| Total | 42 | 100 |
Table 6: What the staff do not like
Shortage of staff 16 (38.1%) and delayed salaries were observed as major challenges faced by staff working in the AHS clinics.
How did you know AHS? | Respondents | |
| No | % | |
| Through Church affiliations | 14 | 33.3 |
| CHAM | 9 | 21.4 |
| Voluntary work | 3 | 7.1 |
| Advertisement | 7 | 16.7 |
| Relief duties | 3 | 7.1 |
| Access to treatment | 4 | 9.5 |
| Job searching | 2 | 4.8 |
| Total | 42 | 100 |
Table 7: How did you know Adventist Health Services (N = 42)
A total of 14 (33%) of respondents knew AHS through church affiliations, 9 (21%) through CHAM and 7 (16.7%) through advertisement
Challenges | Respondents | |
| No | % | |
| Inadequate staffing | 12 | 28.6 |
| Late payment of salaries | 7 | 16.7 |
| Inadequate resources | 13 | 30.9 |
| Lack of education assistance | 4 | 9.5 |
| Delayed communication | 6 | 14.3 |
| Total | 42 | 100 |
Table 8: Challenges faced while working for Adventist Health Services (N = 42)
To a greater extent 13 (30.9%) inadequate resources and 12 (28.6%) inadequate staffing were viewed as major challenges faced by staff working in the AHS clinics
How to overcome challenges | Respondents | |
| No | % | |
| Timely supply of drugs and supplies | 13 | 31.0 |
| Recruit additional staff | 8 | 19.0 |
| Renovate staff houses and health centre buildings | 5 | 11.9 |
| Employ medical personnel to be responsible for all the health centres | 6 | 14.3 |
| Rotation of staff every five years | 4 | 9.5 |
| Improve communication | 4 | 9.5 |
| Decentralization of leadership | 2 | 4.8 |
| Total | 42 | 100 |
Table 9: How to overcome the challenges (N = 42)
The supply of drugs 13 (31%) and 8 (19%) recruitment of additional staff were largely viewed by respondents as part of addressing challenges faced by staff working in the AHS clinics.
Where to go when problems arise | Respondents | |
| No | % | |
| The In-charge | 20 | 47.6 |
| AHS Secretariat | 5 | 11.9 |
| HR | 6 | 14.3 |
| Immediate Supervisor | 4 | 9.5 |
| Team work | 3 | 7.1 |
| Church Pastor | 4 | 9.5 |
| Total | 42 | 100 |
Table 10: If problems faced where to go for help (N = 42)
The In-Charge was trusted by majority 20 (47.6%) of the respondents to address their problems and this was followed by the Human Resources Officer (HR) 6 (14.3%)
Why the staff decided to work for AHS? | Respondents | |
| No | % | |
| Sharing same beliefs | 11 | 26.2 |
| No option, job was available | 6 | 14.3 |
| To work in rural areas | 7 | 16.7 |
| Chosen for me by my sponsor | 3 | 7.1 |
| Used to access treatment at the AHS | 6 | 14.3 |
| Good at assisting staff with problems | 5 | 11.9 |
| It is very close to where I come from | 4 | 9.5 |
| Total | 42 | 100 |
Table 11: Why did you choose to work for AHS? (N = 42)
At least 11 (26.2%) of respondents decided to work for AHS because of sharing beliefs whereas 7 (16.7%) because they wanted to work in rural areas.
The study aimed at looking at what works well and what does not in the 16 clinics of Adventist Health Services has yielded the following implications;
Majority of participants in this study were males (54.8%) and these were clinic managers. This may suggest that leadership positions in the clinics are dominated by male health workers and may imply less participation in decision making processes by female health workers or female health workers decline to take up leadership positions or these female health workers are not given the opportunities to take up these leadership positions. The study done before (Costantino Errani et al, 2021), has shown that the idea that men and women are different and have different working styles and skills and the belief that males are more dominant and more status-worthy than females leads to gender barriers and stereotypes that restrict women from entering male-dominated specialties. Further, a leadership gender gap also exists; although women consist of 70% of the health care workforce, they occupy only 25% of leadership positions. This entails that it is high time now that women not in only health care setting but in all sectors, should be given rightful positions so that gender-based inequalities should be history of the past.
The study has showed that majority of participants working in Adventist Health services were in age groups of 45 -54 (35.7%), 35 - 44 (26.2%) and 25 - 34 (23.8%). This indicates that Adventist Health Services has a mixture of both young and middle-aged population which need nurturing to maintain them in employment in a relatively long-term duration. This finding may further suggest that these health care providers are in their prime age to focus on their career paths, organization can invest in them and those in their middle ages may have trust in the organization indicating that they are secured in their work, or simply due to unemployment challenges, they may get stuck in the Adventist Health Services because they may not get employment anywhere else, or these employees are comfortable with their families perhaps due to conducive working environment as established by studies done before (Remus et al., 2017; Britt et al., 2001). In these studies, it was indicated that both the relationship between daily work environment engagement and work-family interpersonal capitalization and the indirect effects of daily work engagement on the family outcomes were stronger for employees with higher intrinsic motivation than for those with lower intrinsic motivation. Consequently, enriching experiences were also associated with deriving benefits from the deployment. In other words, good working environment may foster reduction of stress to the employee and to the families which may contribute to peace of mind and possibly productivity both at work and at family levels.
The importance of employees’ work experience has not been left behind; the study has revealed. This is simply because 45% and 19.1% of the employees have had work experience of 5 - 9 years and 1 - 5 years respectively. This may have several implications; workers might be new in the service coming straight from various colleges and see Adventist Health Services as the starting point of their career path, or there may be a lot of turn over creating environment which is not allowing them to grow and stay long, might be workers who have been moving from one place to the other looking for green pastures or as a result of frustrations or being bullied. Several studies in the past (Janet, 2016; Zenobia et al., 2013; Chan et al., 2009; Yamaguchi et al., 2016) have shown reasons why workers leave their places of work and get employment elsewhere. The reasons that trigger nurses' intention to leave are complex and are influenced by organizational and individual factors such as, lack of job satisfaction. Given the complexity of issues outlined in this analysis, nurse managers should assist their nursing staff to deal with those
influences, make efforts to address the nursing shortage that will require additional communications and recognize the needs and values of their staff and empower them to create a better work environment. As a consequence, their commitment to the organization can be fostered. Interventions aiming to increase nurse retention should distinguish between care settings.
Health workers’ work-family conflict will decrease retention. Regarding home healthcare, allowing nurses to fulfill family responsibilities will increase nurse retention. Furthermore, nursing home nurses, increasing nurses' job control will increase nurse retention. Current literature reports that 20-25% of nursing staff experience bullying behaviour. The main perpetrators are nurses in a senior position to those being bullied and colleagues who are established staff members. Those likely to be bullied are students and new staff members. Bullying can cause distress and depression, with up to 25% of those bullied leaving their jobs or the profession, and have an impact on patient care. Factors contributing to bullying are hierarchical management and employees not feeling empowered. Silence and inaction by managers and colleagues allow this behaviour to continue. A zero-tolerance policy and the addressing of this behaviour clearly and promptly by managers should be investigated. Staff being bullied should be supported by colleagues as cited by previous studies (Judith, et.al., 2010; McIntosh et al.,2010).
Getting employment and staying long in the employment are totally two different things. Having conducive environment at work and interest to work play a great role in retaining staff. In this study, members of staff liked most having friendly workmates (26.2%) at work followed by having morning prayers (19.1%) and some were influenced by their profession. This finding is congruent with what previous studies have established that money is not only means of motivation (Morris et al., 2022; Karayanni and Nelken, 2022). In these studies, it was found that distinctions between intrinsic and extrinsic motivation are discussed in many studies, including divergence in the types of associated rewards or outcomes that drive behavioral action and choice. Intrinsically motivated behaviors are computationally similar to extrinsically motivated behaviors, in that they strive to maximize reward value and minimize punishment. In this case punishment may be undesired outcome of different facets. However, actions that do not lead to reward are ubiquitous in many species and in many experimental paradigms. Outcomes that are apparently non-optimal can be interpreted as the consequence of optimal decisions whose goal is to optimize a combination of intrinsic and extrinsic rewards.
Shortage of staff (38.1%), delayed salaries (23.8%), absent from duties (14.3%) and poor working environment were issues haunting the Adventist Health Services employees, the study has revealed. These findings have the following implications; employees’ productivity may be negatively affected which may equally affect the quality of care offered to patients or staff members themselves may be demotivated which may affect their working situation. Coincidentally, a study done before (Efendi et., al 2019). In this study, four key attributes of nurse retention were identified in the analysis, specifically motivation, intention, and individual decision; strategy and intervention; geographic context; and attachment to work. Antecedents of nurse retention included the healthcare system at the macro level, the health care facility, health personnel, and living conditions. Retention has consequences for individual nurses, the healthcare organization, and the overall health system. Our concept analysis provides clarification to better understand nurse retention along with its implications for the healthcare workforce. It is therefore important to improve the working environment of all workers and health care workers is not an exceptional. This initiative improves productivity and the relationship of workers with their families, colleagues and employers.
Much as Adventist Health Services clinics are spread across Malawi, in this study, it has been established that majority of staff knew more about the clinics through the church (33.1%) and Christian Health Association of Malawi (CHAM) (21.4%). Media play a great deal in advertising any type of business let alone health care institutions. However, the most important channel of communication is good customer care coupled with quality services leading to user satisfaction. The finding in this study has several implications; it could be that working conditions in CHAM facilities are good and acceptable to employees, remunerations may also be acceptable, influence from religious beliefs must be playing a vital role, or people might just need to explore other avenues or sides of the coin they have not experienced before. These findings are consistent with studies done before (Robbins & Davidhizar, 2020; Glenn, 2007). In these studies, Employees are interested in managers who can lead in a positive and encouraging manner. Nurses who are content in their positions correlate to a reduction in staff turnover and improve retention. When the nursing staff are satisfied with their employment, patient satisfaction rises. Health care organizations can see this trickle-down effect through increases in patient satisfaction scores over time. The promotion of effective communication and positive attitudes enhances a healthy environment for all employees and staff. Health care organizations should evaluate individual nurse managers on units to promote transformation of leadership qualities; this will directly result in staff satisfaction, staff retention, and patient satisfaction. Essentially, leadership skills have an influence to workers so it is important to have managers who have desirable and acceptable skills in management.
Inadequate resources including staffing (33.3%) has been shown as the main challenge facing Adventist Health Services clinics as revealed by this study. This may imply that patient care is compromised, members of staff are overworking, motivation to work as members of staff may be negatively affected so this will lead to patients being unsatisfied with care, they receive from the health worker and therefore staff burn out may be enviable. Consequently, this may affect the quality of care offered to the patients. According to Wafa et.al., (2021) and McVey, (2023) medical errors are common in health care settings when there is shortage of staff and this compromises the quality of care. Nursing staffing shortages contribute to extended nurse-to-patient ratios and increased workload for staff. Increased workload contributes to missed nursing care and correlates with increased patient length of stay, readmission rates, patient safety errors, and hospital-acquired infections. As a result of staff shortages, law suits are very common which hitches on the finances of an organization. This calls for proper planning to avoid anomalies in health care settings in as much as there are staff shortages as reported in the study before (Schwatz et al., 2024, Alghamdi 2016). In these studies, it was found that acute care settings, which manage the care of very complex patients, need innovations that lessen nurses' workload burden while ensuring safe patient care and outcomes. Further, nurse managers need to address the workload issues with regard to the real nature of nursing work; this could increase nurses' productivity, nurses' satisfaction, turnover, work stress and provide sufficient staffing to patient care needs.
The study did not only show challenges faced by the staff but it also provided the possibilities of addressing these challenges. Therefore, the study has established that recruitment of staff (19%) and timely supply of drugs and consumables may improve the quality of care given to patients. A study done before (Wei et al., 2019) has shown that nurse resilience is crucial in the service delivery especially in the presence of shortage of staff coupled with drastic shortages of consumables. Fostering nurse resilience is an ongoing effort. Nurse leaders are instrumental in building a resilient nursing workforce. The strategies identified to foster nurse resilience will not only impact the nursing staff but also improve patient outcomes. Seven strategies are identified to cultivate nurse resilience: facilitating social connections, promoting positivism, capitalizing on nurses' strengths, nurturing nurses' growth, encouraging nurses' self-care, fostering mindfulness practice and conveying altruism. A stable nursing team has a positive impact on improving patient outcomes. To mitigate the impact of a nursing shortage, nurse leaders can enhance their own resilience and then recruit, hire and retain resilient staff nurses in an effort to improve nurses' intent to remain (ITR).
The study has showed that Clinic managers (47%) and Human Resources Officers were viewed as responsible persons handling staff problems. This may suggest that these officers are able to handle staff by virtue of their positions, may have necessary skills that attract members of staff to go to them when they experience problems or members of staff have no option but simply to go to them. These findings are not consistent with the study findings done before (Hill et al., 2018). In that study, it was established that facility managers can be successful if they work closely with the human resources officers. In other ways, there is need for team work in any work settings. When discussing the availability and gaps in supports available when managing poor performance, managers were aware of the majority of the supports available to them in the workplace but there was a disconnect between managers and the HR department. Nurse managers' and clinical nurses' understanding of the concept of quality improvement and how it applies to the practice of nursing differed. Each group identified that quality improvement can be beneficial to nursing practice, but blamed each other for potential benefits not being realized. Both nurse managers and clinical nurses offered similar solutions with varied emphasis on how quality improvement could improve nursing practice and patient outcomes.
Employees in the adventist Health Services clinics were quick to express how they took a decision to get employment in the Adventist Health services. In this study, 26% of the employees joined the workforce because of beliefs and some desired to work in rural area 16% while others had no option but to take what was available at the time of looking for the job (14.3%). Usually, people look for supportive environment at work places which enhances productivity and peace of mind. It is evident that from the time in memorial until the turn of the century, workers in general spend more time at work than they do the same at home. Therefore, it is important that these workers should be in the conducive environment at work place which must be carefully chosen. A study that was done in Norway (Westlie et al., 2022), established that health workers were more likely to work in areas where they grew up. There was a higher probability of working in a rural area if the doctor had grown up in a rural community and of working in general medicine if this had been their preference as a student.
Adventist Health Services (AHS) with a network of 16 clinics across Malawi, has created demand for services of varied in nature. This demand has also been extended to job creation and the reason why it has a large workforce. It is evident that AHS is better placed to serve communities at all levels because of its natural setting in rural areas to a large extent and in urban areas at a smaller scale level where the services are largely focused. On the other hand, the challenges faced by AHS are multiple as revealed by this study ranging from inadequate finances, staffing, resources and consumables in general. However, members of staff have expressed interest in the institution but were quick to request leadership to address the challenges to be able to provide quality services to the beneficiaries. Based on this, the study recommended workable strategies to beef up income creation to make the institution sustainable, improve the welfare of staff and ultimately provide quality health care to the beneficiaries. Therefore, a follow up study is needed to look into the organizational culture that will transform AHS to suit the changes in the 21st century.
Considering the fact that Adventist Health Services has clinics all over Malawi, reaching all of them to access information required traveling and expenses which were not adequate. In certain situation participants were comfortable to express themselves in a language that was not familiar to the investigator and needed interpreters so this was never easy.
It takes more than person to come up with the piece of work of this nature. I would like therefore to express my profound gratitude and immense appreciation to the following individuals whose contributions to this work has been commendable. Adventist Health Services management and staff for approving and taking part in this study, my family for the tireless support during the entire period of doing this work, Prof. Anna-Karin for the guidance, clinic managers for the support, Dr. Happy Fyson Kasenga for the support, Mrs. Mtisunge Nkolokosa for helping out in setting up some pages of this paper and others too numerous to mention.
The author has no conflict of interest while undertaking this piece of work
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
