
Research article | DOI: https://doi.org/10.31579/2641-0419/233
1Department of Cardiology, National University Hospital Center Aristide le Dantec of Dakar; Faculty of Medicine, Pharmacy and Odontology-DAKAR (SENEGAL).
2Cheick Anta Diop University of Dakar / Doctoral School of Life Sciences, Health and Environment (ED-SEV) / Biology, Nutrition and Human Pathology.
3Department of Cardiology, Idrissa Pouye General Hospital of Dakar; Faculty of Medicine, Pharmacy and Odontology -DAKAR (SENEGAL)
*Corresponding Author: Paul Coffi HESSOU, Departments of Cardiology, Aristide le Dantec National University Hospital Center; and Idrissa Pouye General Hospital of Dakar (SENEGAL)
Citation: Joseph S. MINGOU., Maboury DIAO, Fatou AW LEYE, Mouhamadou B. NDIAYE., Simon A. SARR., et all (2022). Stable Angina Pectoris: One-Year Outcomes of Patients with Obstructive Coronary Artery Disease: Multicenter Sutdy in Dakar (Senegal). J. Clinical Cardiology and Cardiovascular Interventions, 5(1); Doi:10.31579/2641-0419/233
Copyright: © 2022 Paul Coffi HESSOU, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 October 2021 | Accepted: 29 December 2021 | Published: 05 January 2022
Keywords: stable angina pectoris; obstructive coronary artery disease; coronary risk factors; clinical outcome; sub-Saharan Africa
Background: CAD management is important in prevention of disease progression. But we have very little study or research on the evolution of stable angina in amulatory patients without coronary antecedents and with obstructive coronary disease.
Purpose: The objective of our study was to analyze the clinical and angiographic profil of patients with stable chest pain and to assess their angina status one year outcomes.
Patients and methods: All patients who presented with symptomatic angina pectoris and/or signs of ischemia and first diagnosis of obstructive CAD in the Cardiology Departments of Idrissa Pouye General Hospital and Aristide Le Dantec National University Hospital Center of Dakar, from March 01, 2019 to December 31, 2020 were selected.
The clinical characteristics, initial angiographic findings, therapeutic strategy and outcome within the first year were analyzed.
Results: During the study period, 84 outpatients presenting with symptomatic stable chest pain and first obstructive coronary artery disease were selected. The mean age was 63.01± 9.37 years. Male preponderance was observed with 63(75%) patients; Clinical symptoms were dominated by typical pain with 46.4% (n=39) ; the risk factors were dominated by hypertension 61.9% (n=52); diabetes 41.7% (n=35) and dyslipidemia 33.3% (n=28).
During follow-up, 10 patients (11.90%) remained untraceable while 9 patients (10.71%) were not available for check-up; 3 patients (3.57%) died during follow-up. Only 62 patients (73.80) could be evaluated; among those who were alive and controlled, 26 patients (41.93%) with angina at baseline still had angina symptoms, 2 patients (3.22%) had undergone myocardial infarction; one (1.61%) had undergone urgent revascularization; one (1.61%) patient developed heart failure. Finally 32 patients (51.61%) were event-free and angina-free
Conclusion: The management of outpatients with stable chest pain and first obstructive CAD appears favourable, with good adherence to guideline-based therapies one year outcomes. Stable chest pain is not associated with an increased risk for adverse cardiovascular outcomes but there remains room for improvement in terms of risk factor control.
ACEI: Angiotensin Converting Enzyme Inhibitor
ARB: Angiotensin receptor blocker
CAD: Coronary artery disease
DAPT: Dual Antiplatelet Therapy
DVD: double-vessel disease
HDL-C : High-density lipoprotein cholesterol
LAD : Left artery descending
LBBB : Left bundle branch block
LCx: Left circumflex
LDL-C : Low-density lipoprotein cholesterol
LVEF : Left ventricular ejection fraction
LMCA: Left main coronary artery
MACE: Major adverse cardiac events
PCI: Percutaneous coronary intervention
RBBB : Right bundle branch block
RCA: Right coronary artery
STEMI: ST-Elevation Myocardial Infarction
SVD: Single-vessel disease
TVD: Three-vessel disease
Introduction
Stable angina pectoris is defined as episodes of chest pain precipitated by physiologic situations of increased oxygen demands to the heart. It occurs most commonly during or immediately after exercise. Indeed stable angina is characterized by chest discomfort or angina equivalent that is provoked with exertion and alleviated at rest or with nitroglycerin [1, 2]. This is often one of the first manifestations or warning signs of underlying coronary disease. Therefore the recognition and appropriate management of stable angina is critical in reducing the risks of future complications [3]. The most important complication of stable angina is the possibility of progression to acute coronary syndrome. Stable angina is also associated with an average annual risk of 3% to 4% for myocardial infarction or death [4].
As outlined in Societies of Cardiology guidelines, management strategies include lifestyle modification, risk factor reduction, pharmacological, and invasive management if significant obstructive CAD is present [1]. Several studies have explored the prognostic impact of stable angina in patients with CAD [5, 6, 7, 8].
Lifelong treatment and monitoring are required in patients with coronary artery disease. The clinical course of these patients may be benign over time but also fraught with cardiovascular complications that can be treated during follow-up.
This study was, therefore, aimed to evaluate the clinical and coronary angiographic profile of outpatients with symptomatic stable chest pain and first obstructive CAD, their treatment, and to assess one-year outcomes.
Patients and Method
2-1. Study design and patients
This was an observational, descriptive, and analytical study conducted from March 1, 2019 to October 31, 2021, in Cardiology Departments of General Hospital Idrissa Pouye and Aristide Le Dantec National University Hospital Center of Dakar.
We had included in our study all outpatients with symptomatic stable angina or ischemic equivalent (dyspnea, palpitations, blockpnea ...) after non-invasive test and who had significant coronary lesions at coronary angiography. All patients with known coronary artery disease (history of STEMI, PCI, and coronary artery bypass surgery) were excluded.
2-2. Baseline characteristics of study population
Information on demographic characteristics, cardiovascular risk factors, symptoms, and noninvasive test results was collected before coronary angiography was performed. Some patients had been contacted for additional information. Hypertension was defined as a systolic blood pressure ≥ 140 mmHg and/or a diastolic blood pressure ≥ 90 mmHg; diabetes was defined as chronic hyperglycemia. It is confirmed if the fasting blood glucose level is ≥ 1.26 g/l during two successive tests; Hypercholesterolemia was defined by a total cholesterol > 2 g/l, an HDL-cholesterol < 0> 1.6 g/l; Obesity was defined by a body mass index (BMI) > 30kg/m2 ; normal weight 18-24,9 kg/m2 and overweight, 25-29 kg/m2
The presence of angina was recorded at baseline and annual check-up, and was defined as chest pain during physical exertion or equivalent symptoms necessitating occasional or permanent use of antianginal drugs in the judgment of the cardiologist.
Symptoms were classified as typical angina, atypical chest pain, ischemic equivalent, or no symptoms. Typical angina was defined as [1] chest pain or substernal discomfort that is [2] caused by exertion or emotional stress and [3] relieved by rest and/or nitroglycerin. Atypical chest pain included patients with atypical angina (only two of the above criteria) and those with non-angina chest pain (one or none of the above criteria). Ischemic equivalents were considered any collection of clinical signs (dyspnea, dizziness, arrhythmias, blockpnea).
The suspicion of CAD was based on the presence and characteristics of chest pain symptoms and the presence of noninvasive test results (ECG, Exercise ECG, Echocardiography, and Stress Echocardiography).
We assessed the left ventricular ejection fraction by the Simpson biplane method. It was considered normal for values above 50%.
2-3. Assessment of angiographic CAD
All patients underwent coronary angiography according to the standard Judkin's technique. Coronary angiography was performed through the femoral or radial approach and coronary was assessed in multiple projections by two experienced operators. Angiographic findings were collected from the electronic coronary angiography report.
The severity of coronary lesions was assessed by the degree of stenosis (the percentage reduction of the arterial lumen): In our study we have considered Non-significant lesions as stenosis < 50>
To assess the consequences of angina evolution on cardiovascular outcomes, patients were categorized into 3 groups according to the evolution of angina between baseline and 1 year: persistence, complications and disappearance.
Predefined endpoints for angina progression included symptoms, results of noninvasive tests at 1 year (ECG, echocardiography, stress echocardiography) and major adverse cardiac events (all-cause mortality, nonfatal myocardial infarction, unstable angina hospitalization or revascularization, heart failure hospitalization, and cerebrovascular event) at subsequent follow-up.
2-4. Statistical analysis
All variables in study were entered in SPSS version 16 for windows statistical software and analyzed; Descriptive statistics were generated with percentages for discrete variables; means and standard deviations for continuous variables. The Chi-square test was used and considered significant for p < 0>.
2-5. Ethical aspects
The study was done in accordance with the Declaration of Helsinki. All patients who agreed to participate had given their consent freely. Furthermore, according to the protocol in our cardiology departments, patients gave always written informed consent before the different diagnostic tests.
This study was also approved by the Research Ethics Committee (REC) of the Cheikh Anta Diop University of Dakar (Protocol Number 0407/2019/CER/UCAD).
3-1. Demographic and clinical characteristics
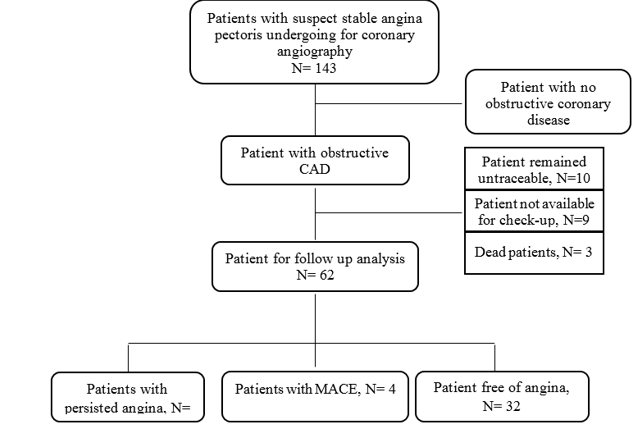
During the study period, 1137 patients were admitted in both department of Cardiology for coronary angiography. Of these, 143 were suspected for stable angina pectoris; 59 patients (41.26%) had normal coronaries while 84 patients (59.74%) had significant lesions of CAD and constituted the study group.
The baseline clinical characteristics of patients are given in table 1. There was a male preponderance with 63 patients (75%); the mean age was 63.01± 9.37 years, with extremes of 31 and 81 years. The most representative age ranges was [60-69[years with 38 patients (45.24%).

Clinical symptoms were dominated by typical pain, 46.4% (n=39); 7 patients (8.3%) had presented with dyspnoea. There were not significative difference between both symptoms following the number of disease vessels (p=0.07).
The prevalence of hypertension was 61.9% (n=52); diabetes was 41.7% (n=35); dyslipidemia was 33.3% (n=28). The table 2 shows the biological parameters of study population.

In our study, at least one noninvasive test was performed in all patients. These tests were mainly resting Electrocardiogram and resting echocardiography with 100% (n=84) and 86.9% (n=73) respectively.
On electrocardiogram, repolarization disorders were dominated by ST segment sub-shift and negative T waves with 17.92% (n=15) and 25% (n=21) respectively.
Abnormalities of the systolic function of the left ventricle with an Ejection Fraction < 50>
3-2. Angiographic characteristics
Coronary angiography revealed that 27 patients (32.14%) had single-vessel; 28 patients (33.33%) had double vessel disease; and 29 patients (34.52%) had triple vessel disease. The right radial approach was the most used with 84.52% (n=71). Coronary angiography revealed 324 coronary lesions. According to the degree of coronary artery obstruction, tight lesions were the most important with 48.14% (n=156) followed by significant lesions with 23.14% (n=75).
Amongst the vessels involvement the most common was the left anterior descending (LAD) with 39.20% (n=127), followed by the right coronary artery (RCA), 28.08% (n=91) and the Left Circumflex (LCx) 25% (n=81). All angiographic findings are summarized in table 3.

Out of the 84 patients with obstructive coronary artery disease, 37 patients (44.05%) had recommended for angioplasty, and 47 patients (55.95%) for medical management only.
The number of angioplasties performed was 43. The procedure were mostly related to LAD and RCA with 57.14% (n=25) and 30.95% (n=13) respectively. The direct stenting technique was used in 45.24% (n=19) of cases. Active stents were used in the majority of cases with 80.95% (n=35). There were no major incidents during the procedures. However, we noted one [1] patient with defective desobtruction of the right coronary and one patient [1] had the right coronary ostium dissection. There was no death during the procedure.
The table 4 summarizes the characteristics of angioplasty and medical treatment. Aspirin was the most frequently used drug (90.48% of patients); Dual antiplatelet therapy (DAPT) was used in 46.23% of patients. The use of lipid-lowering drugs was also high overall, with a significantly frequent rate (69.05%), whereas angiotensin-converting enzyme inhibitors (ACEI) or angiotensin II receptor blockers (ARB) were used more frequently (76.20%) ; Ninety-one point sixty-seven percent patients (89.5%) were taking beta blockers. Only 55.95% of patients took calcium antagonists, whereas use of other antianginal drugs (25%) and oral anticoagulants (28.57%) was lower.
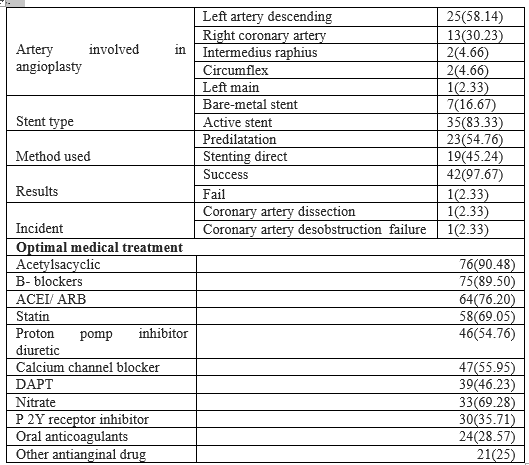
ACEI: Angiotensin Converting Enzyme Inhibitor; ARB: Angiotensin receptor blocker; DAPT: Dual Antiplatelet Therapy
3-3.One-year outcomes of patients with obstructive coronary artery disease
During follow-up, 10 (11.90%) patients remained untraceable while 9 (10.71%) were not available for check-up; 3 (3.57%) patients died during follow-up. Only 62 (73.80) patients could be evaluated; among those who were alive and controlled, 26(41.93%) with angina at baseline still had angina symptoms, 2(3.22%) had undergone myocardial infarction; one (1.61%) had undergone urgent revascularization; one (1.61%) patient developed heart failure. Only 32(51.61%) patients were event-free and angina-free. These findings are summarized in figure 1.
This study showed that patients with stable chest pain and obstructive CAD were older and predominantly male. This finding was consistent with other studies results but with and advanced age in certain study populations [9, 10]. This shows that the onset of stable angina with obstructive coronary artery disease in sub-Saharan African is early. This disparity could be explained on the one hand by the much higher life expectancy in these countries. On the other hand, the low awareness of the population on the relationship between lifestyle and cardiorespiratory diseases could be another explanatory factor of this difference.
In the current study we further tried to elucidate the risk factors. Among our patients the most prevalent risk factors associated to obstructive CAD were hypertension, diabetes, dyslipidemia and physical inactivity. Although these patients constituted a heterogeneous group, modifiable risk factors frequencies were important and suggested the need for heightened efforts for preventive strategies in our study cohort. The low proportion observed for smoking in our study could be explained by cultural and religious constraints which would influence massive consumption.
Typical angina and atypical were the most important symptom observed; however there were not significative difference between both symptoms following the number of diseased vessels.
Coronary angiography revealed that 27 patients (32.14%) had single-vessel; 28 (33.33%) patients had double vessel disease; and 29 (34.52%) patients had triple vessel disease. The literature does not provide any specific data on the coronary status of the patient with stable angina.
The right radial approach was the most used for coronary angiography with 84.52% (n=71).This approach has the advantage of reducing haemorrhagic complications as observed in the RIVAL study [11] and overall mortality according to the MATRIX study [12].
In our study 62 (73.80%) patients were recommended for angioplasty. Only 37 (59.68%) had done it. This is due to the high cost of this procedure in relation to the limited resources of the patients and also to the lack of systematic health coverage for this kind of therapeutic invasive procedure.
The majority of patients (83.33%) had received an active stent as recommended in the guidelines [13, 14]. Active stents, compared to bare-metal stents, bring a decrease in the rate of restenosis and new revascularization procedures, but without a decrease in death or myocardial infarction. The direct stenting technique performed in 45.24%. The advantage of direct stenting is to reduce the procedure time, the amount of contrast injected, the radiation time and the cost. Overs investigators further notes that direct stenting would reduce the peri-procedural mortality rate [15]. Our success rate was 97.67%, similar to the rates reported in the literature [16]. These success rates are related to both accumulated experience and technical progress.
In patients with stable coronary syndromes revascularization reduces cardiovascular death and MI compared with conservative treatment. In our study revascularization was performed in 44.27% of patients but we did not observe a significant difference in angina status between these patients and those who received optimal medical treatment.
However, controversy exists over the benefit of revascularization in patients with chronic stable CAD compared with medical management [17, 18]. Results from the COURAGE study implicated that PCI did not reduce risk of death, MI and other cardiovascular events when added to current medical treatment in patients with stable CAD [19]. In contrast, a large meta-analysis resulted in a benefit of revascularization. The positive effects of revascularization are clearly shown in patients with angina symptoms. In these cases, PCI or CABG more effectively relieve angina, reduce treatment with anti-angina drugs as well as improve physical resilience and quality of life [4, 20]. In this context, the latest ESC guidelines recommend revascularization on the basis of the presence of significant coronary artery stenosis, the severity of ischemia and the expected benefit for prognosis [1]. Indeed, the individual benefit/risk ratio must always be evaluated and revascularization considered only if its expected benefit outweighs its potential risk [1, 4].
The goals of management of stable angina due to obstructive CAD are to reduce symptoms and prevent future adverse events [1, 3]. Our study shows a low rate of MACE and mortality while disappearance of angina was observed in 51, 62%. Several studies have explored the prognostic impact of stable angina in patients with CAD [5, 6, 7, 8, 21, 22]. In the Multinational CLARIFY Study, among 7212 (22.1%) patients who reported angina at baseline, angina disappeared (without coronary revascularization) in 39.6% at 1 year [5].
Our results were different with those observed in these studies. The discrepancy in outcomes might be explained by differences in inclusion criteria, adverse outcome definitions, different methodology and length of follow-up time.
Conclusion
In our study population the management of outpatients with symptomatic chest pain and first obstructive CAD appears favourable, with good adherence to guideline-based therapies one year outcomes. Stable chest pain is not associated with an increased risk for adverse cardiovascular outcomes but there remains room for improvement in terms of risk factor control.
Limitations of the Study
The study cohort was relatively small, especially the patient population with angina symptoms and obstructive coronary artery disease; 22.62% of patients were lost to follow-up. Thus, for a better understanding of the management and outcome of stable CAD in Sub-Saharan population, studies with larger numbers of patients are needed.
In addition we did not repeat the analysis of cardiovascular risk factors after the follow-up period. This would have made it possible to assess the effect of treatment on modifiable risk factors.
Declaration of interest: the authors declare that they have no interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
