
Case Report | DOI: https://doi.org/10.31579/2578-8965/146
1 Anatomo patólogo, Academia Mexicana de Cirugía, Laboratorio Grupo Diagnóstico.
2 Anatomo patóloga Laboratorio Grupo Diagnóstico.
3 Gynecoobstetra Hospital Ángeles-México.
*Corresponding Author: José de Jesús Curiel-Valdés, Anatomo patólogo, Academia Mexicana de Cirugía, Laboratorio Grupo Diagnóstico, Mexico.
Citation: Jose Curiel Valdes, Rubí A. Patiño, Gabriel R. Escalante, (2023), Squamous Cell Carcinoma of the Uterine Cervix not Associated with HPV Case Report with 4-year Follow-Up. Case Report. J. Obstetrics Gynecology and Reproductive Sciences, 7(1) DOI: 10.31579/2578-8965/146
Copyright: © 2023 José de Jesús Curiel-Valdés. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 December 2022 | Accepted: 19 December 2022 | Published: 06 January 2023
Keywords: squamous cell carcinoma of the cervix; human papilloma virus; carcinoma not associated with papilloma virus
It is known that the vast majority of squamous cell carcinomas of the cervix are secondary to HPV infection and the recent WHO classification already includes a section on cancer not associated with HPV. Many lesions not associated with HPV that were initially negative were reportedly confirmed to be related to HPV when they were reanalyzed using a different methodology.
It is known that the vast majority of squamous cell carcinomas of the cervix are secondary to HPV infection and the recent WHO classification already includes a section on cancer not associated with HPV [1,2]. Many lesions not associated with HPV that were initially negative were reportedly confirmed to be related to HPV when they were reanalyzed using a different methodology [3]. Statistics show varied figures, especially in large series [4-9]. In a recent meta-analysis, [10] the figures range between 100% including only adenocarcinomas and 5% in squamous cell carcinomas have been found. There are very few reports of individual cases or small series [11]. Sigrid (2022) [5] recently reported in Austria 9 cases with 3 pre-invasive lesion and 6 infiltrating lesions that were negative for HPV, in biopsies. The purpose of this paper is to report a rare case of invasive squamous cell carcinoma with 4 years follow-up.
Case Report:
In 2914, a 72-year-old woman with a high-grade intraepithelial lesion (HSIL) went for a cytology test to obtain a second opinion. She is of low socio-economic status and education, and lives in a rural area. She was not bleeding or having any discomfort at the time she went for the test. Colposcopy was performed (Figure 1, A-C) with an open cervical os that allowed the squamo-columnar junction to be seen at the edge. The test was satisfactory. The outside had thin light red epithelium alternating with whitish areas; no abnormal vessels were seen. With acetic acid (AA) there was no reactivity. The light red areas of varying thicknesses became more evident alternating with whiter linear areas. There were no mosaic or dense thick areas. With iodine, the central area was negative while the periphery area was positive. Cytology was also done with a brush ensuring that sample from the endocervical canal, showed atrophic epithelium with no evidence of displasia. Epithelial maturation was performed with local estrogens, estriol (0.5mg) for 21 days. On the 26 day, a new colposcopy was performed (Figure 2, A-C). It was also adequate, cervix with an open orifice with epithelium which has a glandular appearance around the orifice. It bled easily in radius 12 to 3. The rest with smooth surface had no visible vessels or aceto reactive areas. With iodine, all the periphery of the glandular area was intensely positive. A new liquid-based sample for rtPCR and cytology showed mature epithelial cells; it had normal endocervical cells, without any evidence of atypia. The result of rtPCR (Seegene South Korea) for 28 types of viruses, 19 high risks: 16,18, 26, 31,33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, 69, 73, 82 and 9 low risks: 6, 11, 40, 42, 43, 44, 54, 61, 70 was negative. The review of the previous cytology reported as HSIL only showed atrophic basal cells that were confused with dysplastic cells and occasional cells which have larger nuclei that were classified as ASC US. (Figure 1E).
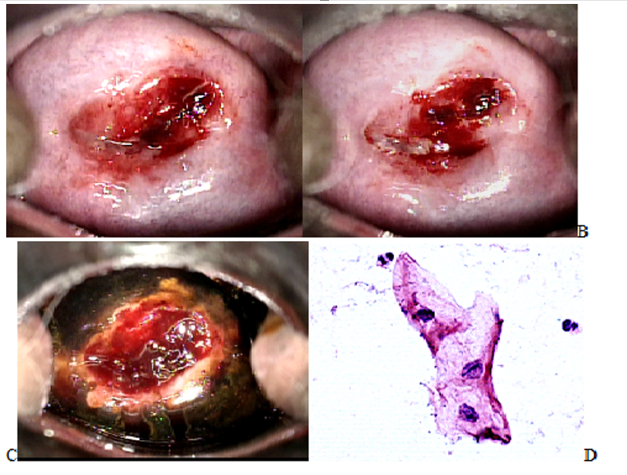
Figure 1: Colposcopy October 2016. A Squamo-columnar junction (SCJ) was visible at the edge of the hole in radius 6 to 9 (arrows) and outside in radius 10 to 3 and 4 to 5 (arrows); TZ had thin epithelium, visible vessels and without any alteration. B With AA, there was mild irregular smooth non-persistent reactivity, with mucus that was not completely removed to prevent bleeding. In radius 12 to 3 at the edge of the orifice, there was slight bleeding with the application of AA by spraying. In this area, the tissue is of the glandular type. The ZT is more clearly defined, which is the entire acetoreactive area. C With lugol the ZT is iodine negative, and the SCJ is more clearly defined. D Original conventional cytology 40X slide review was originally interpreted as HSIL, cells whose nuclei slightly increased in size, there was no atypia (arrows), altered chromatin or enhancement of the nuclear membrane and in our laboratory diagnosed as ASC US. E Liquid-based cytology done simultaneously with colposcopy, atrophy without atypia. (E).
The patient was advised that she required continuous annual surveillance. However, she came back 4 years later (2018) because she had intermittent and scarce bleeding of 2 years of evolution that increased in the last two previous weeks. Colposcopy showed neoplastic exophytic bleeding lesion of the cervix in the posterior lip. The biopsy showed moderately differentiated keratinizing invasive squamous cell carcinoma, which was negative for p16 (BioSB California USA clones RBTp16). A new trPCR study was also carried out for the 28 viruses mentioned in the tissue; it was negative. It was sent to an external laboratory to perform PCR (MY09/11 – sequencing) for the 86 types of viruses, which was negative. An external laboratory study of p16 with a different Ab (Masters Diagnostica España clones MX007, p16-INK4) was also carried out. It was negative. The patient was referred to oncologist consultation. But there was no further contact with her, nor was her evolution known.
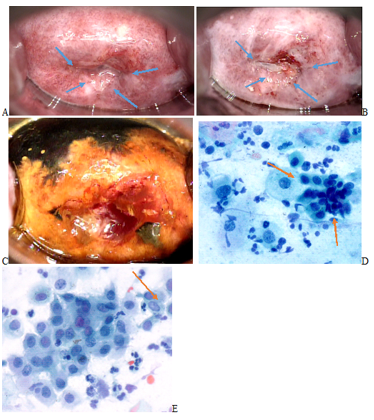
Figure 2: Colposcopy November 2016, with three weeks of estrogen. A, without any substance, elongated orifice, with thin glandular-looking tissue, light red, without abnormal vessels. The SCJ was visible at the edge of the glandular tissue and the rest of the cervical surface was smooth without abnormal vessels. B, With AA, the faint smooth irregular reactivity of the previous colposcopy is not appreciated, because of maturation and glycogen acquired. The area that bleeds easily with the introduction of the vaginal speculum and AA spray application remains similar as in the first colposcopy. C, With Lugol, the ZT is iodine positive, and it is broader than that in the previous colposcopy. D, LBC in the simultaneous with the second colposcopy had mature squamous cells with no atypia.

Figure 3: Colposcopy 2019 (4 years later). A, evident exophytic bleeding lesion B and C, Invasive epidermoid carcinoma (HE 10 and 40X) evident atypia with mitoses. D, E, in panoramic and detail (10X and 40X) p16 positivity only in lymphocytes among the neoplasm; the neoplastic cells are negative or occasionally faintly cytoplasmic positive.
When CC is related to HPV, it is known that the evolution from low-grade lesion to invasive cancer is from 5 to 10 years and in cases of immunodeficient patients, it takes 2 years. The evolution in cases not related to HPV is not documented. For the reported case, no lesion could be detected by cytology and colposcopy the previous 4 years including invasive cancer. However, the bleeding occurred 2 years before the last examination. Unfortunately, the patient lives in a rural environment, with low economical resources; she hid the bleeding from her relatives. The histological study shows the same type of cells and architecture similar to those related to HPV. p16 staining in the uterine cervix is recognized as a very reliable indirect marker associated with HPV, with some exceptions of false positives. However [12,13], p16 negativity means that there is no evidence of cellular damage by HPV. Non-specific p16 positivity has been reported not to be related to HPV, but it is not in this case since the staining was negative. The absence of HPV was corroborated by two methodologies, the negativity of PCR and by two antibodies for the p16 of different brands.
a case of a 72-year-old woman with invasive cancer of the cervix is documented. Over a period of 4 years, she developed invasive squamous cell carcinoma without previous dysplasia or lesion, which was confirmed by colposcopy and cytology. She was negative for HPV by rtPCR, which was confirmed in biopsy. She had p16 negativity in the third examination at the 4th year. The invasive lesion perhaps started prior to the first bleeding for two years when the invasion began.
No source of financial support
No publishable conflict of interest
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
