
Review Article | DOI: https://doi.org/10.31579/2690-8808/133
1 Research Scholar, Department of Pharmacy Practice, ISF College of Pharmacy, Moga, Punjab, India, 142001.
2 B.Pharm, Pharm.D, Assistant professor, Department of Pharmacy Practice, ISF College of Pharmacy, Moga, Punjab, India 142001.
*Corresponding Author: Mandeep Kaur, B.Pharm, Pharm.D, Assistant professor, Department of Pharmacy Practice, ISF College of Pharmacy, Moga, Punjab, India 142001
Citation: Mayank Virmani , Mandeep Kaur.(2022). Squamous Cell Carcinoma of Left Lateral Border of Tongue followed by Therapy Induced Mucositis Grade 4; Journal of Clinical Case Reports and Studies 3(9); DOI: 10.31579/2690-8808/133
Copyright: © 2022 Mandeep Kaur, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 May 2022 | Accepted: 02 June 2022 | Published: 10 October 2022
Keywords: OSSC; EBRT; RIOM; chemotheraputic agents; gray
Carcinomas are the major serious health issue in today’s healthcare system. while its prognosis is difficult at earlier stages. OSSC oral squamous cell carcinomas are reported more than 3 lakhs new cases world-wide and it is sixth most common cancer world-wide. Squamous cell carcinoma is defined as the cancer of soft, flat, thin squamous cells mainly affect the soft cell regions like tongue diagnosed by various investigational imaging and biochemistry parameters. In this case patient was diagnosed with High Grade Squamous Cell Carcinoma. Radiation therapy along with chemotherapy is the option for better therapeutic outcomes. Hence, EBRT therapy is given and in 2 gray every cycle and a total of 59.8 gray, 20 cycle therapy depending on condition of patient. In 90% cases radiation therapy leads to RIOM (Radiation Induced Oral Mucositis) which is totally unprotectable and there in no specific treatment option available in market approved by US-FDA yet. RIOM is diagnosed by WHO grading system based on the parameters and observations. In this condition patient suffers from inflammation, mouth ulcers and progressive condition and patient can not be able to swallow anything. It’s five stage process which treated by giving antibiotic in case of RIOM and oral hygenine, mouthpaints are advised. Levofloxaccin 750mg with clotrimazole mouthpaint was given to the patient. Radiation therapy continued with curative and Supportive therapy and was successful radiation therapy also shows good response and reduction in growth of tumor was observed and therapeutic goals were achieved.
Carcinoma is the term defines cancer occurring in cell, skinline or organ with soft tissues. Various types of cancer growth have been seen in the tongue, but the most common type is squamous cell carcinoma, Squamous cells are thin, flat cells that line the mouth and other organs. Oral cancer is found to be the sixth most common cancer worldwide. Approximately 300,373 new cases of oral squamous cell carcinoma (OSCC) are annually reported around the world[1-2],It typically occurs in elderly men during the fifth-eighth decade of life[3] . In 1976 two scientists Krolls and Hoffman analyzed 14,253 cases of squamous cell carcinoma of the oral soft tissues and found that 35.2% of the intra-oral lesions were observed only on the tongue [4]. In India, Oral carcinoma has become a major health problem mainly due to the high prevalence of smokeless tobacco use. There are two types of tongue cancer:
Through Grades we can identify the severity of cancer growing in the mouth and are as follows. There are 3 grades of mouth Cancer[5]:
Patient was suffering from squamous cell carcinoma and External Beam Radiation Therapy was given to treat but unexpextedly, Radiation therapy leads to RIOM as its adverse effect .
RIOM (Radiation-Induced Oral Mucositis) is one of the major ionizing radiation toxicities defined as an injury of tissues caused by radiation/radiotherapy (RT), Eventually marked adverse effects on patient quality of life and continuity of cancer therapy [6]. In the United States, its economic cost was approximately to achieve 17,000.00 USD per patient with head and neck cancers. Varies between 7 to 98 days. . RIOM of grades 3 and 4 have been observed in 56% of head and neck cancer patients treated with radiotherapy[6-7]. While risk factors are [8]:-
WHO has designed grading system for stating severity stage of oral mucositis which is as follows:-
The WHO Grading system for Oral mucositis[9]
Mucositis uplift stage by stage and various worsten changes observed as it converted to higher stage followed by healing at last stage which are as follows:-
Developmental Stages Of Mucositis [10]
In 2004, Sonis, a Scientist suggested five stages of Oral Mucositis:-
A 54 years old male patient was admitted in cancer department having complaints of tongue bite while taking meal in afternoon. After 2 days unbearable inflammation and pain at the site of the bite. After some time a sore formation takes place at the left lateral border of the tongue and the patient started following home remedies to cure it. But there's no satisfactory improvement and it was continuously causing discomfort to the patient and condition to become more worsen than earlier. After that patient starts facing difficulty in swallowing and eating food and was not feeling well while talking and sleeping and eating. Afterward, the patient feels much pain and inflammation in the affected region of the tongue. Patient-reported to the hospital and was admitted to Hematology/Oncology department. All the physical examinations, and possible investigations were done. The sore formation that had taken place earlier was converted into a tumor on the left lateral side of the tongue downward basal and identifications were done and were found to be Squamous Cell Carcinoma of Tongue. Socioeconomically patient is non-smoker and follows a vegetarian diet. There is no history of allergy or no previous medication history. After all the investigations ( Table 1), a drug regimen was designed and a follow-up was started (Table 2). The patient was later on drugs and Radiation therapy was started. But on the 6th radiation Cycle patient complained about oral sores and difficulty in swallowing liquid and eating a semi-solid diet. Physical examination was done and on the behalf of investigations itwas confirmed that the patient was suffering from Radiation-induced oral mucositis (RIOM), Grade 4 stage. Radiation therapy cycles were continued, and along with it Supportive therapy for the same was designed and started at that time. Later, After 3 days patient observe a reduction in oral sores and was able to take some liquid diet.
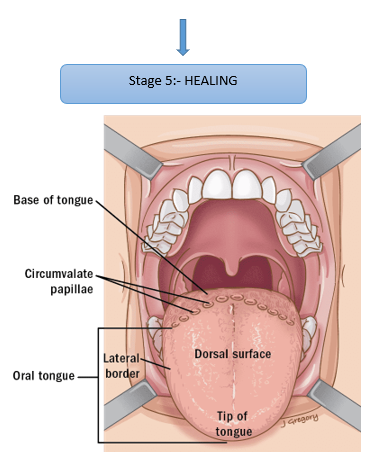
Figure 1 -Image Showing The affected area diagrammatically, Source:- Internet
Biopsy
Laboratory Investigations:-
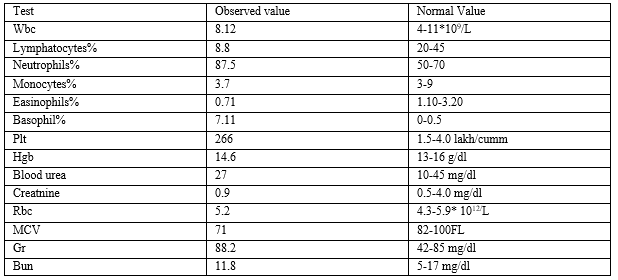
Table1: Laboratory findings of the Patient
Microcystosis and Hypochromia observed
Microcytosis is a blood disorder in which the mean blood cellular volume becomes less than 82 μm3 (82 fL) in adults.
Hypochromia means that the red blood cells have less color than normal when examined under a microscope.
Decreased level of lymphocytes stated that it is due to the known adverse effect of radiation therapy. Many researchers have also stated that(13).
Treatment and Management
Radiotherapy 20 Cycles Advised :- EBRT (External Beam Radiation
Therapy) was given To treat Tongue Cancer (Squamous Cell Carcinoma).
After 6 Cycles Adverse effect of Mucositis grade 3 following grade 4 was observed. The patient was apparently on a semisolid diet
Due to mouth ripe patient was not able to swallow .
Pt was advised to take oral care as :-
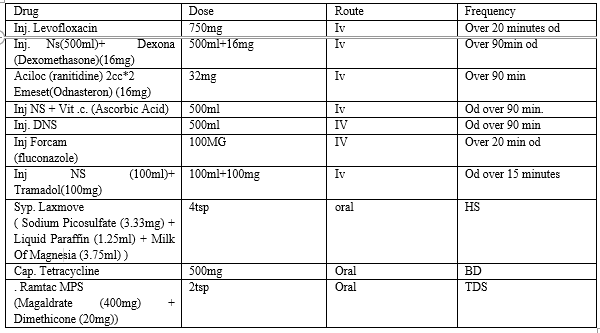
Table2: Indicating Patients Drug Regimen
Same treatment follow-up for the next 3 days was given to the patient. While the Patient was on treatment on its 6Th radiation cycle he observed some difficulties like mouth ripe Which were later confirmed as Mucositis a major adverse effect of Radiation Therapy.
According to studies Approximately 90% of confirmed malignant tumors diagnosed in the oral cavity are Oral Squamous Cell Carcinomas, especially in the tongue, and affect mostly men rather than women[1] . Same in this case a 54 years old male patient was affected and the study also shows a high risk of recurrence of Tumor[1]. Biopsy reports confirmed high-grade squamous cell carcinoma of the lateral region of the tongue. But the patient is quite responsive and in the positive recovery phase. Studies revealed that RIOM occurs in 100% of altered fractionation radiotherapy head and neck cancer patients and cant be protectable lasts between 7-98 days and causes inflammation in the tongue, mucosa, and pharynx[7]. Exactly the same was seen inpatient as the patient was complaining of sores, and was not able to swallow/intake food. Antibiotics are necessary for treatment so antibiotics were prescribed for cure Levofloxacin 750 mg was administered and clotrimazole mouth paint was advised for application to the affected region. No single therapeutic agent has been approved by the US FDA for the treatment of RIOM so random supportive therapy is prescribed for treatment. The patient shows improvement in the condition and for the next three days, the same therapy was continued with radiation therapy for cancer.
The patient is responsive and has a good recovery record with both the conditions Squamous cell carcinoma and RIOM with the treatment plan designed for both the problems. Oral hygiene was highly focused on administering Drug a designed drug regimen at accurate doses, Nutrition is also maintained as the patient was not able to swallow solid and semi-solid diet. Radiation therapy continued even after adverse effects because there is no other successful treatment option for the squamous cell carcinoma later when the patient complained of discomfort supportive treatment was designed and successful therapeutic goals were achieved. Radiation therapy shows a good response in reducing carcinoma growth.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
