
Case report | DOI: https://doi.org/10.31579/2578-8868/317
1Tyumen State Medical University, Ministry of Health of the Russian Federation, 625023, Odesskaya st., 54, Tyumen, Russia.
2Polenov Neurosurgical Institute – Branch of Almazov National Medical Research Centre, 191014, Mayakovskogo st., 12, Saint-Petersburg, Russia.
3Department of Pathology with a course of forensic medicine named after D.D. Lochov, St. Petersburg State Pediatric Medical University, 194100, Litovskaya st., 2, Saint-Petersburg, Russia.
4The North-Western State Medical University named after I.I. Mechnikov, 191015, Kirochnaia st., 41, Saint-Petersburg, Russia.
*Corresponding Author: Darya Sitovskaya, MD, pathologist, Department of pathology Polenov Neurosurgical Institute – Branch of Almazov National Medical Research Centre, 191014, Mayakovskogo st., 12, Saint-Petersburg, Russia.
Citation: Dzhamilya Murzaeva, Darya Sitovskaya, Yulia Zabrodskaya, (2024), Sporadic Hybrid Nerve Sheath Tumour Arising from a Vestibulocochlear Nerve: A rare Case Report, J. Neuroscience and Neurological Surgery, 15(4); DOI:10.31579/2578-8868/317
Copyright: © 2024, Darya Sitovskaya. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 30 April 2024 | Accepted: 17 May 2024 | Published: 29 May 2024
Keywords: hybrid tumors; vestibulocochlear nerve; neurofibroma; schwannoma; hpnst
Hybrid peripheral nerve sheath tumors (HPNST) were first included in the 4th edition of the World Health Organization (WHO) Classification of Central Nervous System in 2016. These tumors are a combination of schwannoma and neurofibroma, and are typically found in the limbs, trunk, and soft tissues. In this case report, we present a rare intracranial localization of neurofibroma/schwannoma with histological examination. Our patient was a 36-year-old man without any tumor genetic syndromes. The tumor measured 1.6 × 1.1 cm and was completely excised. The pathology report showed no significant nuclear atypia, mitotic activity, or necrosis. At the time of writing, the patient is alive and well with no recurrence. It is important to note that HPNSTs are usually benign tumors, but can occur in various locations, including the intracranial region. Further studies with a larger number of cases are needed to determine the exact pathogenetic basis of these tumors.
Hybrid peripheral nerve sheath tumor (HPNST, ICD-O code 9563/0) is a newly recognized entity of peripheral nerve sheath tumors. It is characterized by multiple, discrete areas of different benign tumor components, including schwannoma, neurofibroma, and perineurioma. These tumors mainly occur in the subcutaneous soft tissue and can present a diagnostic challenge. They may also be associated with tumor syndromes, such as neurofibromatosis type 1 (NF1), also known as von Recklinghaus disease, and neurofibromatosis type 2 (NF2). Additionally, there is a condition that was once considered a variation of NF2 but is now known as schwannomatosis. Cranial HPNST is extremely rare [1-5]. This article presents a sporadic case of HPNST in the vestibulocochlear nerve.
The study utilized a resected tumor from the VIIIth pair of cranial nerves of a 36-year-old male. Histological and immunohistochemical (IHC) methods were employed, using standard techniques. Antibodies from Dako (California, USA) were utilized, specifically S100 and CD34. The EnVision polymer detection system was also utilized. To ensure the accuracy of the observed staining, reactions were also performed without primary antibodies. Histological analysis and microphotography were conducted using a Leica Aperio AT2 scanning microscope and AperioImage Scope image manager (Leica Microsystems, USA). The study was conducted in accordance with the Helsinki Declaration of Human Rights. Preoperative examinations and surgical treatments were performed in accordance with the 2015 Clinical Guidelines of the Association of Neurosurgeons of Russia.
A 36-year-old man with a 6-month history of headaches was admitted to the neurosurgery department. The patient did not exhibit any criteria for inherited tumor syndromes, including NF1, NF2, and schwannomatosis. Magnetic resonance imaging (MRI) of the head revealed a 1.6 cm × 1.1 cm lesion on the vestibular nerve, with no associated mass effect on the surrounding brain tissue. The lesion also showed enhancement after intravenous administration of gadolinium-diethylenetriaminepentaacetic acid. A neurological examination showed normal visual fields and acuity, intact cranial nerves II through XII, and normal hearing on both sides. Motor-sensory skills were also normal. The patient underwent successful surgery, with complete removal of the tumor mass and preservation of hearing and facial functions.
Neuropathologic Findings
At gross examination, the lesion was a nodular white-yellow, firm, well circumscribed mass measuring 1.6 × 1.1 cm (Fig. 1).
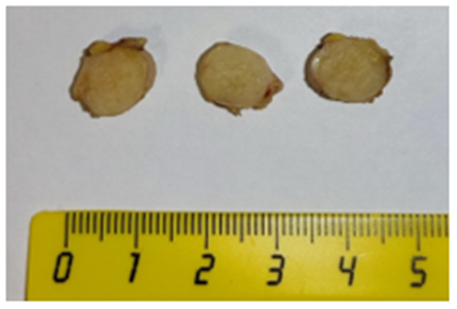
Figure 1: Gross examination of the tumor. The tumor appears white-yellow in color and is encased in a capsule, with a lobular appearance when sectioned.
Tumor diagnosis is primarily based on hematoxylin and eosin-stained sections and immunohistochemistry (IHC). Histologic examination demonstrated a well-demarcated solid neoplasm with two distinctive morphologic and immunophenotypic features. The tumor cells in the predominant schwannomatous areas were composed of spindle cells with bland, tapered, and at times "wavy" nuclei. These cells were arranged in a fascicular growth pattern with focal Verocay body formation (nuclear palisading around nuclear-free areas). Immunohistochemically, these
cells were diffusely positive for S100 protein and negative for CD34. In the second component – neurofibroma areas, the tumor showed low cellularity. The Schwann cells were loosely arranged with fibroblasts with elongated to oval nuclei, delicate chromatin, conspicuous nucleoli, and collagen bundles. Immunohistochemical studies revealed that the tumor cells in this area were particularly immunopositive for S100 protein and focally positive for the anti-CD34 antibody. Focal degenerative atypia with nuclear hyperchromasia was observed. Mitoses and necrosis were not recognized in either component (Figure. 2).

Figure 2: A, B. Histological examination of the tumor, H&E stain, ×400.
A – Tumor structures resembling schwannoma are represented by spindle-shaped cells with Verocay body formations (Antoni A).
B – Tumor structures resembling neurofibroma.
C-E. Results of immunohistochemical reactions, ×400.
C – Diffuse cytoplasmic staining anti-S100 antibody in schwannoma component.
D – Patchy cytoplasmic staining anti-S100 antibody in neurofibroma component.
E – Patchy cytoplasmic staining anti-CD34 antibody in neurofibroma component.
Diagnosis: Hybrid Peripheral Nerve Sheath Tumor with Neurofibroma/Schwannoma Components. We present a case of a benign peripheral nerve sheath tumor with histological and immunohistochemical features consistent with a biphasic pattern of differentiation of schwannoma and neurofibroma in the VIIIth cranial nerve. The patient reported pain after surgery, but at the 7-month follow-up, there was no neurological deficiency. Additionally, there was no recurrence on MRI at the 7-month postoperative mark. This is the first reported case of a hybrid neurofibroma/schwannoma in a vestibulocochlear nerve, to our knowledge.
Since the first report of a hybrid peripheral nerve sheath tumor in 1998, only a few cases have been described. While the majority of these tumors arise in peripheral nerves of the trunk and extremities, there have been rare occurrences in uncommon locations such as the colon, nasal cavity, orbit, and lymph nodes [2-3]. One case of an HPNST tumor affecting the trigeminal nerve has been documented in the literature [6]. In this case, we present an unusual occurrence of a neurofibroma-schwannoma in the VIIIth cranial nerve. The hybrid nature of this tumor is confirmed and highlighted by its histological biphasic pattern and immunohistochemical staining profiles. The schwannoma component shows S100 positivity, while the neurofibroma component stains positive for CD34. The histological differential diagnosis includes spindle cell lesions such as schwannomas, perineuriomas, neurofibromas, and low‐grade malignant peripheral nerve sheath tumors. Conventional schwannomas are composed of a single cell type and are characterized by Antoni A with Verocay body formations and Antoni B patterns. These features are seen in the absence of any other anaplastic features such as mitosis, necrosis, or increased cellularity. It is important to note that degenerative nuclear atypia should not be confused with malignant transformation [2-3]. On the other hand, conventional neurofibromas are composed of two cell types (schwann cells and fibroblasts) and often have collagen bundles. In atypical neurofibromas, there may be mitosis and increased cellularity. The pathogenetic basis of the dual differentiation seen in hybrid lesions is still not well understood.
Hybrid peripheral nerve sheath tumors are typically considered benign and can include neurofibroma/schwannoma, neurofibroma/perineurioma, schwannoma/perineurioma, and schwannoma/neurofibroma/perineurioma. However, there have been rare case reports of local recurrence and malignant transformation in these tumors, similar to conventional benign schwannomas and neurofibromas [1-8]. In our case, we did not observe any recurrence of the tumor during the postoperative follow-up. Further studies are needed to determine the risk factors for local recurrence and malignancy in intracranial neurofibroma-schwannoma.
Hybrid neurofibroma/schwannoma has been reported to be frequently associated with NF1, NF2 or schwannomatosis and rarely occur sporadically [1-3,8]. It has been demonstrated that the majority of hybrid schwannoma/perineurioma cases exhibit VGLL3 rearrangements fused 5' to either CHD7 or CHD9 [9]. However, no recurrent genetic changes have been observed in schwannoma/neurofibroma hybrids. In the case of our hybrid neurofibroma/schwannoma of the vestibulocochlear nerve, no connection with neurofibromatosis was found. This highlights the importance for clinicians to be aware of the potential risk of intracranial hybrid neurofibroma/schwannoma, even in patients without evidence of NF1, NF2, or schwannomatosis.
The authors declare that there are no relevant conflicts of interest.
Informed consent was obtained from this patient in this study.
The study was conducted without sponsorship.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
