
Case Report | DOI: https://doi.org/10.31579/2578-8965/059
*Corresponding Author: Vicente Spinoso, Servicio de Obstetricia y Ginecología, Hospital Obispo Polanco de Teruel, Av. Ruiz Jarabo, s/n, 44002 Teruel, Spain.
Citation: Vicente S. Cruz, Marta C. Morales, Ligia G. Melgosa, Aida R. Lopez (2021) Spontaneous pregnancy following treatment of symptomatic uterine myomatosis with Ulipristal Acetate without surgery J. Obstetrics Gynecology and Reproductive Sciences 5(3); DOI:10.31579/2578-8965/059
Copyright: © 2021 Vicente Spinoso Cruz, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 January 2021 | Accepted: 15 February 2021 | Published: 09 April 2021
Keywords: cases report; pregnancy; uterine fibroids; ulipristal acetate
Uterine fibroids are the most frequent gynaecological benign tumors in women of reproductive age and can cause infertility. Their treatment may be medical, surgical or a combination of both, but they may compromise future fertility in patients in which their wish to conceive has not yet been fulfilled. In this report we present two patients with symptomatic uterine myomas and who wanted to preserve their fertility. Treatment with one or two 12-week courses of 5 mg of ulipristal acetate was prescribed. A decrease in the size of the fibroids was observed, along with adequate control of the symptoms. Spontaneous pregnancies led to two live births without significant complications. Treatment with Ulipristal Acetate may be an effective option to take into account in the management of patients with symptomatic uterine fibroids who refuse surgery or in those in which it is contraindicated and who wish to preserve their fertility.
CRL: Crown-rump length
FHR: Fetal Heart Rate
Hct: Haematocrit
SPRM: Selective Progesterone Receptor Modulator
UPA: Ulipristal Acetate
Uterine leiomyomas are the most common benign tumors in women of reproductive age [1-3]. Although many of them are asymptomatic and frequently undiagnosed, a significant percentage cause important symptoms such as heavy menstrual bleeding, pelvic pain and pressure, anaemia and decreased quality of life [3]. Depending on the anatomical location, they can also cause infertility and an increased risk of abortion [4]. Specifically, those fibroids distorting the uterine cavity can cause alterations in sperm migration, interfere with embryo transport due to affected uterine contractility, and also involve eventual implantation failures as a consequence of impaired endometrial vascularization [5].
The therapeutic approach to treat symptomatic uterine fibroids can be medical, surgical or a combination of both options. However, the optimal treatment would be the one that produces relief or disappearance of symptoms, reduction of fibroids’ volume or their eventual total shrinkage and improvement of fertility rates [6].
Ulipristal Acetate (UPA) is a selective progesterone receptor modulator (SPRM) that has been approved as medical treatment of uterine fibroids in Europe [7]. Its effectiveness in doses of 5 to 10 mg daily during 13-week cycles has been demonstrated, controlling excessive bleeding and reducing fibroids’ size [8]. It’s been also shown as effective as Leuprolide Acetate for the control of bleeding and the decrease in fibroid volume, but with a statistically significant reduction in the reporting of hot flashes when compared to the latter [9]. Endometrial changes related to UPA treatment - have been described, which are benign and reversible a few weeks after stopping treatment. No development of endometrial hyperplasia or adenocarcinoma have been reported [10-11].
There is little evidence reporting the utility of UPA for the treatment of uterine fibroids with a view to improving fertility rates [12]. However, cases reported in Poland [12] and Spain [13] and also the follow-up of 21 patients who came from a pivotal phase III study with UPA in Europe offer good expectations [14]. Khulood et al [6] described in 2016 the first term pregnancy in a patient with symptomatic uterine myomatosis previously treated with UPA without surgery. In our series, we describe two cases with the same characteristics that demonstrate the utility of this drug in improving spontaneous fertility rates without additional treatments.
42-year-old patient, G0, came to the medical consultation presenting a 6-month course of pressure at the hypogastric level and menstrual disorders (hypermenorrhea) for 3 months. As a relevant antecedent, the patient referred myomectomy 12 years ago through laparotomy. On physical examination, it was confirmed the presence of a firm mass at the hypogastric level, approximately 5 cm above the pubic symphysis, not painful on palpation and introduced into the pelvic cavity. A transvaginal ultrasound was performed, showing a heterogeneous uterus of 112.6 x 100.4 x 63.2 mm, where at least 4 fibroids were counted (Figure 1):
A) Anterior myoma measuring 24 x 30 mm, type V FIGO classification
B) Posterior myoma measuring 29 x 24 mm, type V FIGO classification
C) Fundic myoma measuring 35 x 25 mm, type VI FIGO classification
D) Left transmural myoma measuring 51 x 40 mm, type III-V, FIGO classification.
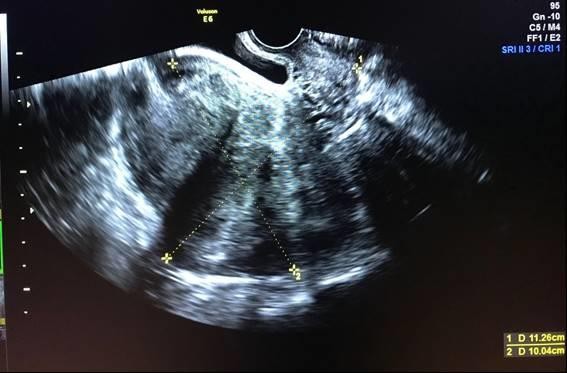
Figure 1. Anterior (A) and posterior (B) fibroid (before pregnancy)
Lab tests showed Haemoglobin (Hb) levels of 10.4 g/dL and Haematocrit (Hct) of 31. 1 %, with a normal biochemistry. The patient had still a wish to conceive, so it was decided to start treatment with UPA 5 mg / day in two courses of 12 weeks each and re-evaluation.
During the treatment, the patient reported pain relief in the hypogastrium and improvement in hypermenorrhea. The haematological profile showed values of Hb: 13.4 g/dL and Hct: 40.1 %; transaminases were within normal limits. As a side effect, few and irregular spotting was reported during treatment.
After completing the two courses of UPA, the patient came to the medical consultation for control visit, reporting an 8-week course secondary amenorrhea . A pregnancy test was performed, being positive. A transvaginal ultrasound showing a gestational sac in situ with an embryo inside with a crown-rump length (CRL) of 4.2 mm corresponding to 6W + 1D and positive Fetal Heart Rate (FHR) quantified at 107x´(Figure 2). It was concluded that the patient presented spontaneous ovulation approximately 2 weeks after finishing the treatment
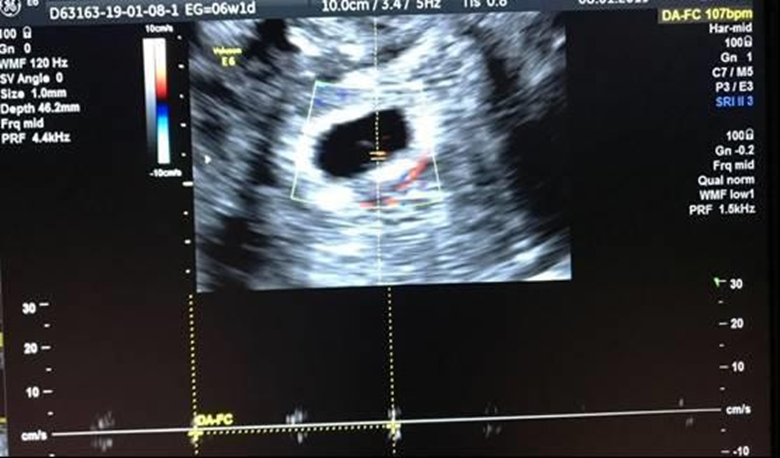
Figure 2. Positive Fetal Heart Rate
During pregnancy follow-up an increase of the volume of the fibroids until 12 weeks was confirmed, without presenting relevant complications. At 20 weeks the size of fibroids were:
A) Anterior myoma, lower third, close to the cervix measuring 31 x 44 mm,
B) Posterior myoma, lower third, close to the cervix measuring 45 x 38 mm
C) Fundic myoma measuring 49 x 35 mm
D) Left myoma measuring 70 x 60 mm, type IV-V FIGO classification
The patient developed gestational diabetes which was controlled with
diet. At 39 weeks, caesarean was performed, obtaining a healthy female newborn with a birth weight of 2,930 Kg, Apgar score of 9 and 10 points and a cord pH of 7.31. Mother and daughter are discharged on the third day of surgery without complications. Mother Breastfed for 9 months and at 3 months post-cesarean section, a transvaginal ultrasound was performed, showing a notable reduction in the size of the fibroids (no myoma observed in anterior uterus surface):
A) Posterior myoma measuring 24 x 20 mm, type V FIGO classification
B) Fundic fibroid measuring 28 x 21 mm, type VI FIGO classification
C) Left transmural myoma measuring 35 x 25 mm, type IV FIGO classification (Figure 3).

Figure 3. Left transmural myoma in pregnancy diagnosis moment.
A 35-year-old patient, G2 / P1 / A1, consulted for presenting menstruation with a tendency to be hypermenorrheal for 7 months, treated with combined oral contraceptives without significant improvement. Then, transvaginal ultrasound was performed, showing:
A) Subserous myoma in fundus measuring 19 x 21 mm, type VI FIGO classification
B) Posterior submucous myoma measuring 23 x 23 mm, type II FIGO classification
C) Posterior submucous myoma measuring 17 x 15 mm, type II FIGO classification
D) Anterior submucous myoma measuring 15 x 14 mm, type II FIGO classification
Laboratory analysis revealed values of Hb of 10.9 g/dL and Hct: 32.1 %, with a normal biochemistry. Based on the symptomatology and the lab tests results it was decided to prescribe treatment with UPA 5 mg / day for 12 weeks (one course). The patient was also appointed to incorporate to the hospital’s surgical waiting list, proposing resection of submucous fibroids by hysteroscopy.
8 weeks after completing UPA treatment, the patient went to the gynecology clinic, reporting secondary amenorrhea just after UPA cessation, concomitantly nausea, vomiting and occasional dizziness for approximately 2 weeks. Transvaginal ultrasound was repeated, showing (Figure 4)
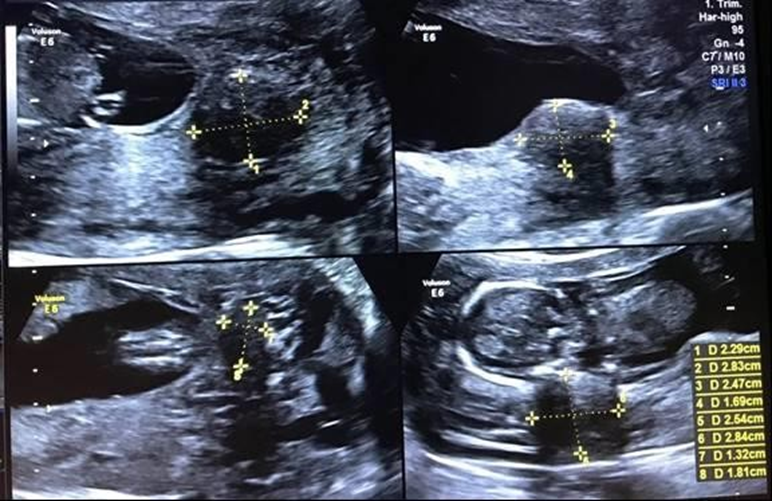
Figure 4. Intramural myoma(A); posterior myoma(B); posterior myoma(C); posterior myoma (D)
A) Intramural myoma measuring 15 x 17 mm, type II FIGO classification
B) Posterior myoma measuring 19 x 18 mm, type II FIGO classification
C) Posterior myoma measuring 15 x 13 mm, type II FIGO classification
D) Posterior myoma measuring 11 x 10 mm, type II FIGO classification
E) Presence of a gestational sac in uterus with an embryo inside with a CRL of 3.25 mm. corresponding to 5.5 weeks and a positive FHR quantified at 116x´.
During pregnancy follow-up an increase in the volume of the fibroids until 12 weeks of gestation was confirmed, without significant complications.
A) Intramural myoma measuring 22.9 x 28.3 mm, type II FIGO classification
B) Posterior myoma measuring 24.7 x 16.9 mm, type II FIGO classification
C) Posterior myoma measuring 28.4 x 25.4 mm, type II FIGO classification
D) Posterior myoma measuring 18 x 13 mm, type II FIGO classification
The patient underwent gestational diabetes during pregnancy, requiring insulin and diet treatment. At 39 weeks gestation was completed by labor induction, obtaining a male newborn with a birth weight of 3,710 Kg, an Apgar score of 9 and 10 points and a cord pH of 7.22, eutocic delivery without complications. Mother and son were then discharged on the second day of the puerperium without incidents. The mother breastfed for 6 months and at 3 months postpartum a transvaginal ultrasound was performed, showing a notable reduction in the size of the fibroids:
A) Intramural fibroid measuring 13 x 13 mm, type III FIGO classification
B) Posterior myoma measuring 12 x 11 mm, type III FIGO classification
C) Posterior myoma measuring 9 x 10 mm type III FIGO classification
D) Visualization of the smallest posterior myoma was not achieved
All fibroids had a low submucosal component (type III FIGO classification), so it was decided to insert an intrauterine device that releases levonorgestrel. She remains asymptomatic to date.
Uterine fibroids have a high impact on the quality of life of patients due to their high morbidity and, despite of their benignity, they can produce heavy menstrual bleeding, pelvic pain, pressure symptoms, infertility, and obstetric complications [3].
Multiple treatments (medical, surgical or a combination of both), have been described for uterine fibroids with a high variable response [16, 17]. However, when choosing a treatment it is essential to take into consideration the patient's age and her desire to preserve fertility. Women with uterine leiomyomas who still wish to conceive may face a dilemma since there are not many therapeutic options available to warrant that goal.
UPA, a member of the selective progesterone receptor modulator (SPRM) family, was approved for the treatment of uterine leiomyomas in Canada, Europe, and numerous countries worldwide [14]. Many studies have demonstrated the efficacy of UPA in controlling menorrhagia and reducing the volume of uterine fibroids in symptomatic patients [8, 9, and 10].
In the two clinical cases described, AUP 5 mg / day for 12 weeks in one or two cycles successfully reduced the volume of the fibroids and allowed the recovery of the normal anatomy of the uterine cavity. This improvement was at least enough to enable an embryo implantation. Although the possible changes in endometrial histology after the end of treatment were not examined, the final outcome was that both patients became pregnant and they had pregnancies with few complications.
This work is added to other existing publications [12, 13, 18-22] that showed the use of UPA in the management of patients with uterine myomatosis who still wish to conceive, and who reject a surgical option since, this option compromised their fertility. In addition to successfully reduce fibroid volume and improve symptoms, the use of UPA avoid the inherent risks of surgery on reproductive capacity, and appear to have no deleterious effects on pregnancy. That is why we think that UPA may be considered a therapeutic alternative in an immediate attempt to achieve conception at the end of treatment [13]. However, in order to be able to make a recommendation based on scientific evidence, the authors advocate conducting prospective studies in the future to establish the safety of this drug as a treatment option for symptomatic uterine fibroids before pregnancy.
Treatment with Ulipristal Acetate may be an effective option in women with symptomatic uterine fibroids unable to conceive and who refuse surgery or surgery is contraindicated. Clinical studies should be carried out to confirm this finding.
The data used to support the findings of this study are available from the corresponding author upon request.
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
This study was sponsored by Gedeon Richter Ibérica SA
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
