
Review Article | DOI: https://doi.org/10.31579/2692-9759/109
1 Medicine student of Federal University of Mato Grosso, Brazil.
2 Interventionist cardiologist from Medicine University of São José do Rio Preto, Brazil.
*Corresponding Author: Alan Vinicius Gamero Osti, Interventionist cardiologist from Medicine University of São José do Rio Preto, Brazil.
Citation: De Oliveira CC, De Mattos Silva FLV, Gamero Osti AV, (2023), Spontaneous Coronary Artery Dissection (SCAD): A Review Article, Cardiology Research and Reports. 5(5); DOI:10.31579/2692-9759/109
Copyright: © 2023, Alan Vinicius Gamero Osti. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 September 2023 | Accepted: 19 October 2023 | Published: 30 October 2023
Keywords: arterial dissection; acute coronary syndrome; angiography
A rare and sporadic disease, Spontaneous Coronary Artery Dissection (SCAD) consists of obstruction of the coronary artery by intramural hematoma, with or without rupture of the intimal layer, without association with atherosclerosis, trauma or iatrogenesis. It is an important cause of acute coronary syndrome (ACS) and sudden death in individuals without typical cardiovascular risk factors. It predominates in women between the 4th and 5th decades of life, being the most common cause of ACS associated with pregnancy, in patients with underlying arteriopathies, especially fibromuscular dysplasia; in individuals with systemic inflammatory diseases such as systemic lupus erythematosus, sarcoidosis, or inflammatory bowel disease; or with hereditary arteriopathies, such as Ehlers-Danlos vascular syndrome and Marfan syndrome. Surviving patients present as clinical manifestations of ACS, ventricular arrhythmias, cardiogenic shock or sudden cardiac arrest, with chest pain consistent with atherosclerotic ACS and elevated cardiac enzymes. The accurate diagnosis of SCAD is important, as its management differs from that of atherosclerotic ACS. If suspicion, coronary angiography should be performed, classifying the lesion according to the Saw Angiographic Classification: if multiple radiolucent lumens or contrast coloration of the arterial wall, type 1; if diffuse stenosis >20 mm, type 2, being the most common; if focal or tubular stenosis <20 mm that mimics atherosclerotic lesion, type 3. American College of Cardiology (ACC)/ American Heart Association (AHA) and European Society of Cardiology (ESC) guidelines suggests conservative treatment in clinically stable patients, and an early invasive strategy by angioplasty coronary artery in patients with severe lesions. Coronary artery bypass surgery is considered in high-risk injuries.
SCAD stands for the obstruction of the coronary artery, mainly the anterior descending artery, by an intramural hematoma within the middle layer of the coronary vessel wall. This hematoma compresses the arterial lumen, leading to the development of a false lumen and causing ischemia. It is not associated with atherosclerosis, trauma, or iatrogenic factors. DEAC is an important cause of acute coronary syndrome (ACS) and sudden death in individuals without cardiovascular risk factors. It is more common in women in their fourth and fifth decades of life and is a common cause of ACS associated with pregnancy or the postpartum period, possibly linked to fibromuscular dysplasia. Physical and emotional stress are precipitating factors, as they can lead to the shearing of the coronary artery. Clinical manifestations in patients include ACS, particularly ST-segment elevation myocardial infarction (STEMI), ventricular arrhythmias, cardiogenic shock, or cardiac arrest. The clinical presentation may resemble atherosclerotic ACS in over 90% of cases, with elevated cardiac enzymes. If there is suspicion, coronary angiography should be performed, especially in cases of STEMI, where routine thrombolysis should not be administered. In cases of diagnostic uncertainty, intravascular imaging can and should be utilized. An accurate diagnosis is crucial because the management of SCAD differs from the treatment of atherosclerotic ACS. Despite current diagnostic advances, SCAD remains underdiagnosed in many cases and is treated as atherosclerotic ACS, which can negatively impact the prognosis, as these conditions require different approaches. Guidelines recommend a conservative approach in clinically stable patients, involving beta-blockers and aspirin, as more than 70% of cases can achieve angiographic healing. Intervention and revascularization, either percutaneous or surgical, are reserved for cases of instability or high-risk lesions. According to the available literature, there are no significant differences in long-term mortality risk, recurrent DEAC, or the need for revascularization between conservative and invasive therapies.
I. Epidemiology and Risk Factors:
A rare cause of acute coronary syndrome (ACS), it accounts for less than 1% of all acute myocardial infarctions [14]. Its prevalence ranges from 0.1% to 1.1% in patients undergoing coronary angiography, but its incidence is often underestimated. It predominantly affects young patients, with a higher incidence between the 4th and 5th decades of life, and it typically occurs in individuals with no traditional cardiovascular risk factors. Women are affected in 90% of cases [10, 14], particularly during pregnancy or the postpartum period, making it the leading cause of acute coronary syndrome in pregnancy [20]. There is a lack of information about its occurrence in men, but the literature indicates that it occurs earlier in this population, between the 3th and 4th decades of life [4, 8, 20]. It can affect any coronary artery but primarily occurs in the left anterior descending coronary arteries, which branches into diagonal and septal branches, supplying the anterior wall, anterior septum, apical, and apical cap of the heart [8, 10, 11, 14].
II. Physiopathology:
The cross-section of coronary arteries reveals three concentric histological layers: intima, media, and adventitia. SCAD occurs when there is blood accumulation within the medial layer, and two theories exist to elucidate its causative event. The first proposes that spontaneous rupture in the intimal layer of the coronary arterial wall allows blood to enter through this lesion, forming a false lumen and consequently predisposing to the formation of an intramural hematoma. The second theory postulates that the primary event is spontaneous bleeding from the vasa vasorum, small blood vessels that penetrate the arterial wall, originated by a primary rupture or a thrombosis on that vessel, resulting in the formation of an intramural hematoma. Both the dissected vessel wall flap and the hematoma compress the arterial lumen, obstructing blood flow through the artery, leading to coronary insufficiency and ischemia of the cardiac tissue [2, 8, 10, 11, 14].
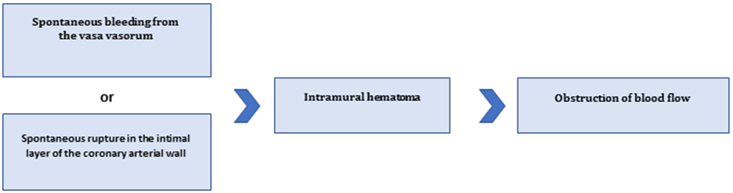
Image 1: Physiopathology of SCAD (Fonte: Camila Costa de Oliveira).
III. Etiology:
Spontaneous Coronary Artery Dissection (SCAD) has an uncertain but multifactorial etiology, influenced by underlying arteriopathies, hormonal factors, genetic factors, or ischemic inflammatory diseases. The most common precipitating external factors are extreme emotional or physical stress, such as intense Valsalva maneuver, coughing, vomiting, intense isometric exercise, and weightlifting. The increase in circulating catecholamines potentiates the shear stress on the vascular wall, contributing to the occurrence of SCAD [3, 4, 7, 8, 10, 11, 14, 15, 17].
Fibromuscular dysplasia, characterized by alternating areas of stenosis and dilation, leading to vascular abnormalities, is the most commonly associated arteriopathy with SCAD, especially its multifocal form affecting extra coronary arteries. Patients who do not have imaging findings consistent with multifocal fibromuscular dysplasia often exhibit other arterial abnormalities such as dissections, aneurysms, or tortuosities in the coronary artery[8, 10, 14].
More common in the female population, particularly in women using oral contraceptives, undergoing post-menopausal hormone replacement therapy, receiving infertility treatment, pregnant, or postpartum, SCAD is linked to the female hormone’s estrogen and progesterone, although the exact mechanism remains unclear. Hypotheses suggest that estrogen and progesterone receptors present in the coronary arteries, when stimulated, weaken the vessel wall, resulting in arterial wall rupture, intramural hematoma formation, and the onset of clinical symptoms. SCAD associated with pregnancy affects younger individuals, especially in the third decade of life, and carries a worse prognosis, with larger infarctions, multi-arterial involvement, and reduced left ventricular ejection fraction [3, 7, 8, 11, 14].
Patients with severe inflammatory disorders, such as systemic lupus erythematosus (SLE), inflammatory bowel diseases (IBD), polyarteritis nodosa, sarcoidosis, and celiac disease, may have a higher predisposition to developing SCAD, albeit in smaller proportions[8, 11].
Some genetic conditions are known to cause vascular fragility and arterial dissection, increasing the likelihood of SCAD, including Ehlers-Danlos vascular syndrome, Marfan syndrome, and Loeys-Dietz syndrome. It has been observed in relatives with first and second-degree relationships with patients, but despite this, SCAD is not strongly associated with familial factors, showing a higher occurrence as a sporadic condition[8, 11].
IV. Clinical Manifestations:
Despite the wide range of possible signs and symptoms, SCAD commonly presents as Acute Coronary Syndrome (ACS), with angina-like chest pain radiating to the arm, neck, or back and cardiac enzyme alterations in the majority of cases. About 70% of patients experience acute myocardial infarction (AMI), with more than 50% having non-ST-segment elevation ACS (NESTEACS) and the minority having ST-segment elevation myocardial infarction (STEMI) [10, 11, 14]. Patients may also experience ventricular arrhythmias, congestive heart failure, cardiogenic shock, pericardial tamponade or sudden cardiac death [3, 8, 10, 11, 13, 14, 17].
SCAD associated with pregnancy may have more severe symptoms and a higher risk of recurrence, with serious complications such as ventricular arrhythmias, cardiogenic shock, or sudden death. On cardiovascular physical examination, sinus tachycardia and a B3 gallop rhythm can be noticed if the right coronary artery is involved[8, 11, 14].
The main site of injury is the left anterior descending coronary artery, occurring less often in the right coronary artery, the left circumflex artery and the left main artery, decreasing in incidence rate. On cardiovascular physical examination, sinus tachycardia and a B3 gallop rhythm can be noticed if the right coronary artery is involved[8, 10, 11, 14].
V Diagnosis:
The diagnosis of SCAD is made through the combination of a physical examination, EKG, laboratory tests and angiography, the first-line diagnostic modality in SCAD. Early diagnosis is crucial because, despite the initial symptoms being similar to those of atherosclerotic ACS, the treatment for these two conditions is different. Therefore, early diagnosis of SCAD enables the selection of the appropriate therapy and favorable outcomes [1, 8, 10, 11, 14].
The electrocardiographic pattern may consist of ST-segment elevation in ischemia or transmural infarction and T-wave inversion or ST-segment depression in subendocardial ischemia. An echocardiogram can reveal abnormalities in regional contractility within the involved coronary territory[8, 10, 11, 14].
Coronary angiography by catheter is the gold standard for diagnosing SCAD, with the angiographic appearance of the coronary artery being serrated due to the presence of multiple lumens or intramural hematoma. Left ventriculography can reveal abnormalities in wall motion [1, 2, 3, 14]. The finding of coronary artery tortuosity is highly prevalent in patients who have experienced SCAD and is associated with a higher likelihood of recurrence, being considered a possible marker or potential mechanism for SCAD[6].
The Saw classification was adopted for standardizing the angiographic assessment of SCAD. Type 1 representing the classic appearance of SCAD, characterized by multiple radiolucent lumens or contrast in the arterial wall; type 2 is marked by a change in arterial caliber with clear demarcation from normal diameter to diffuse narrowing, further subdivided into variants 2A (diffuse arterial narrowing delimited by normal segments proximal and distal to the intramural hematoma) and 2B (diffuse narrowing extending to the distal tip of the artery); type 3 refers to focal or tubular stenosis, usually less than 20 millimeters in length, mimicking atherosclerotic lesions. [1, 2, 4, 8].
Other diagnostic possibilities include intravascular ultrasound (IVUS) or optical coherence tomography (OCT), which allow for the visualization of dissection flaps, delamination of coronary layers, intramural hematoma, and the presence of lumens. Despite being considered an effective tool in identifying arterial dissection, the OCT and IVUS are expensive, little available and presents risks of spreading dissection if the guidewire enters the false lumen. The use of intracoronary imaging is reserved for rare cases in which angiography fails to establish the diagnosis[10, 13].
VI. Treatment:
The treatment of SCAD includes the use of medications and revascularization, with the choice between these modalities being individualized and dependent on clinical presentation, the extent of dissection, and the amount of compromised myocardium[2, 3, 5, 12, 15].
Conservative treatment is the initial modality of choice for stable SCAD patients and is carried out through anticoagulation and dual antiplatelet therapy. Experts recommend long-term aspirin use, but there are no studies supporting the benefit of dual antiplatelet therapy in SCAD[2, 3, 4, 8, 10, 11, 14, 15, 16]. Beta-blocker therapy should be prescribed based on studies that have demonstrated that this class reduces the recurrence of SCAD. The use of ACE inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) is reserved for acute myocardial infarction complicated with left ventricular systolic dysfunction [14]. Reviews of studies have shown angiographic healing in over 90% of stable patients managed conservatively within a one-month period. However, studies have demonstrated an approximately 18% recurrence rate. Stable patients are monitored with coronary angiography, with invasive coronary angiography reserved for high-risk patients with recurrent symptoms[6, 10, 14, 16].
Guidelines do not recommend thrombolytic therapy in SCAD in ST elevation Myocardial Infarction, due to the possibility of coronary artery rupture and cardiac tamponade, making the diagnostic mandatory to avoid clinical deterioration[2, 3, 14].
Because of the potential development of early myocardial infarction complications in conservatively managed SCAD patients and the need for emergency revascularization, prolonged inpatient monitoring is necessary as part of a conservative strategy for SCAD management[8, 14].
In high-risk patients with refractory ongoing ischemia, left main artery dissection, or hemodynamic instability, the treatment of choice should be revascularization through percutaneous coronary intervention (PCI) or coronary artery bypass grafting surgery (CABG). The choice between these management options should be individualized, and there is no consensus between the American Heart Association (AHA) and the European Society of Cardiology (ESC) regarding which is preferable[2, 8, 12]. Studies have shown that PCI for SCAD can increase the risk of complications because the guidewire can enter the false lumen, and balloon dilation or stent placement can cause new dissection or propagate an existing one. Furthermore, most SCAD lesions are distally located, making PCI challenging[12, 14, 15, 16]. The European Society of Cardiology advocates the use of second-generation drug-eluting stents in the invasive treatment of SCAD; however, the literature has not demonstrated a difference in prognosis in relation to the nature of the stent chosen. Current guidelines recommend maintaining dual antiplatelet therapy for at least one year in patients undergoing PCI [10, 14].
CABG is reserved for SCAD patients after a failed attempt at PCI or patients with dissection of the left main or proximal coronary artery or refractory ischemia despite conservative management. Studies have demonstrated a high graft occlusion rate due to competitive flow in the healed native vessels [14].
Immediate complications of SCAD include ventricular tachyarrhythmias, ventricular free wall or septal rupture, congestive heart failure, and cardiogenic shock [3, 8, 10, 13, 14, 15, 19]. As a common symptom following spontaneous coronary artery dissection is chest pain, which can occur as a sequela of the dissection or due to non-cardiac causes such as stress, anxiety, or depression the patients should be evaluated for possible psychiatric disorders, such as post-traumatic stress disorder, depression, and anxiety, to improve their quality of life[9, 10, 14, 18].
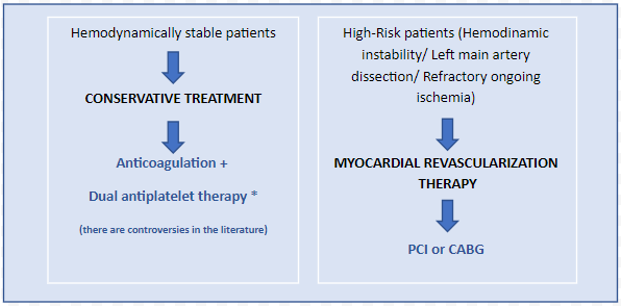
Image 2: Treatment of SCAD (Fonte: Camila Costa de Oliveira).
Despite diagnostic advances, SCAD remains underdiagnosed and treated as atherosclerotic ACS, the most common cause of ACS in the general population, damaging the patient's prognosis, as these are conditions that require different management. Rapid clinical suspicion and diagnosis through coronary angiography are decisive for successful treatment and prognosis. Unstable patients or injuries with high complication potential can be treated invasively, but there are no comparative studies in the literature.
We declare that there is no conflict of interests.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
