
Case Report | DOI: https://doi.org/10.31579/2690-1897/145
1 Department of Maxillofacial Surgery Hospital of Specialities Rabat, Morocco.
2 Faculty of Medicine and Pharmacy of Rabat. Mohammed V University in Rabat, Rabat, Morocco
*Corresponding Author: ajaa El azzouzi. Department of Maxillofacial Surgery Hospital of Specialities; CHU Ibn Sina, Av. Abderrahim Bouabid, Rabat-Morocco.
Citation: Rajaa El Azzouzi, Othmane Bouanani, Sarra Benwadih, and Malik Boulaadas. (2023), Spontaneous Cervical Hematoma Revealing a Parathyroid Adenoma: A Case Report, J, Surgical Case Reports and Images 6(2); DOI:10.31579/2690-1897/145
Copyright: © 2023 Rajaa El azzouzi, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 February 2023 | Accepted: 06 February 2023 | Published: 08 February 2023
Keywords: adenoma; hematom; hypercalcemia; parathyroid; case report
Introduction:
Neck hematoma is a rare but potentially lifethreatening medical condition.
Although spontaneous rupture of a parathyroid adenoma with extracapsular hemorrhage is rare, it may cause cervical and mediastinal hematoma, leading to potentially fatal consequences, it should be considered when a non-traumatic sudden neck swelling coexists with hypercalcemia.
Case’s presentation:
This report describes an atypical spontaneous rupture of an asymptomatic parathyroid adenoma in a 42-year-old woman who presented to the emergency room after the acute installation of an unpainful voluminous swelling in the right side of her neck, after eliminating a vascular emergency. Hemodynamically stable, the patient was treated conservatively with a period of observation in hospital, 1 month follow-up imaging with CT confirmed a regression of the half volume of the hemorrhagic lesion and the likely source of hemorrhage as a parathyroid nodule with significant vascularity. The diagnosis was confirmed on histopathological analysis after elective surgical exploration of the neck 3 months of a benign parathyroid adenoma. The patient made a full recovery with immediate normalization of her biochemistry post-operatively.
Discussion:
Spontaneous rupture of a cervical parathyroid adenoma with extracapsular hemorrhage should be considered when a non-traumatic sudden neck swelling coexists with hypercalcemia. The most appropriate treatment, in the absence of dyspnea or dysphagia, we believe that it is preferable to intervene surgically in a delayed manner.
Conclusion:
A high suspicion index is needed, particularly in post-menopausal women, to reach a diagnosis and allow optimal management. Since bleeding may recur, we suggest an independent indication for definitive parathyroidectomy surgery.
Parathyroid adenoma can cause very rarely extracapsular bleeding. The clinical presentation can vary more widely depending upon the extent of hemorrhage. In 1934, Capps first reported a case of massive hemorrhage secondary to rupture of a parathyroid adenoma [1]. This report describes an atypical spontaneous rupture of an asymptomatic parathyroid adenoma in a 42-year-old woman who presented to the emergency room after the acute installation of an unpainful voluminous swelling in the right side of her neck with no others accompanied signs.
We report a case of 42-year-old woman, operated for a thyroid nodule 16 years ago presented to the emergency department with a sudden onset of unpainful voluminous swelling of the right side of her neck.

Figure 1: Front view showing the swelling of the right cervical region
No triggering factors such as trauma was mentioned. The patient did not report any compressive symptoms such as dyspnea or dysphagia, hoarseness nor any systemic symptoms of inflammation or infection. Clinical examination revealed in an afebrile patient with stable vital signs, the presence of a painless right basi-cervical mass of soft consistency, not beating, not expanding, without inflammatory signs or ecchymosis apparent beneath the skin, measuring 6.5 cm in long axis, the rest of the examination noted the absence of epistaxis, otorrhagia or gingivorrhagia.
As she was hemodynamically and respiratory stable, An initial computed tomography (CT) scan with injection was performed and showed the presence of a voluminous hemorrhagic lesion of the right carotid space, well limited spontaneously hyperdense, accentuated after injection of contrast product measuring 35*33*65 mm, pushing back the sterno-cleido mastoid muscle outside and arriving inside in contact with the hyoid bone, respecting the aero-digestive channel, which evokes a false aneurysm or a spontaneous cervical hematoma given the anamnestic data.
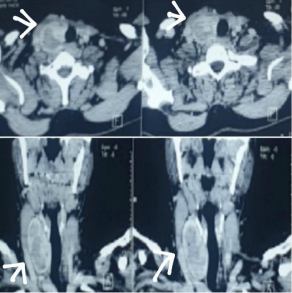
Figure 2: Axial and coronal CT scan showing the cervical hematoma
A vascular surgery opinion was requested, eliminating a vascular emergency. As she was hemodynamically stable, she was treated conservatively with a period of observation in hospital to monitor for signs of neck organ compression. 1 month follow-up imaging with CT and cervical ultrasound confirmed a regression of the half volume of the hemorrhagic lesion and the likely source of hemorrhage as a parathyroid nodule with significant vascularity.
The blood tests showed a corrected calcium of 2.70 (normal range 2.20–2.60) parathyroidhormone (PTH) 16.3 (normal range 1.60–6.90).
The diagnosis was confirmed on histopathological analysis after elective surgical exploration of the neck 3 months after her presentation. This revealed a benign parathyroid adenoma with evidence of acute and chronic bleeding. The patient made a full recovery with immediate normalization of her biochemistry post-operatively.
The first observation of an extracapsular hemorrhage of parathyroid origin was made by Capps in 1934 [1]. It concerned a 50-year-old woman who died suddenly in a context of dyspnea associated with a hematoma of the cervicothoracic region. The autopsy revealed that death was due to a suffocating hematoma secondary to a parathyroid hemorrhage. The development of respiratory complications from mediastinal extension or compressive symptoms is only described in a few cases, with the latter requiring emergency surgery [2,3].
A review of the literature shows that the majority of cases are seen in middle-aged females, as we reported in our case. Thus, spontaneous neck hematomas in post-menopausal women should prompt a PHPT workup.
In all described cases, hematoma is the first sign of hyperparathyroidism. Clinically, it manifests itself either as spontaneous neck pain or as dysphagia [4,5]. Dyspnea and dysphonia, which are rarer, are symptoms that should motivate an emergency surgical intervention according to Massard and Roma [6,7]. This atypical clinic often leads to diagnostic errors: in the pure cervical form, a thyroid hemorrhage is more often suspected. In the cervicomediastinal form, a ruptured thoracic aortic aneurysm is more likely to be suspected [7]. The patient's first priority is to be put in condition, followed by a radiological examination, mainly a CT scan and a cervical ultrasound, as well as biological tests, blood calcium and parathyroid hormone levels, to rule out differential diagnoses and to determine the etiology.
Simicic has defined a diagnostic triad suggestive of cervical hemorrhage of parathyroid origin which consists of cervical pain on swallowing, cervical and/or thoracic ecchymosis associated with hypercalcemia [8]. Studies have suggested that the rapid growth which eventually leads to an acute hemorrhage when demand outstrips the vascular supply.
As for the most appropriate treatment, in the absence of dyspnea or dysphagia, we believe that it is preferable to intervene surgically in a delayed manner.
This attitude, shared by most authors, has allowed us, in our experience, to carry out preoperative localizing examinations of the pathological gland, which then simplified the operative procedure. Moreover, the deferred emergency removal of the parathyroid gland makes it possible to intervene when the hematoma is in the process of resorption. Our experience shows that it is then easier to identify the parathyroid gland and the other anatomical structures including the recurrent laryngeal nerve [9].
Based on this case report and a few similar cases reported in the medical literature, a diagnosis of extracapsular parathyroid hemorrhage should be considered when a non-traumatic sudden neck swelling coexists with hypercalcemia. Conservative management is a suitable option for patients who remain hemodynamically stable but all should undergo a period of observation in hospital, and a definitive surgical exploration should be considered within at least a month of presentation to avoid the risks of recurrent bleeding.
Free and informed consent has been given by the patient.
The authors declare no conflicts of interest
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
