
Case Report | DOI: https://doi.org/10.31579/2690-1897/146
1 I Degree Specialist in MGI. Assistant teacher. Faculty of Medical Sciences Sagua la Grande. Villa Clara. Cuba.
2 3rd year resident in Rheumatology, Arnaldo Miliàn Castro Provincial Teaching Hospital. Villa Clara. Cuba.
3 I and II Degree Specialist in MGI. Assistant Professor. Faculty of Medical Sciences Sagua la Grande. Villa Clara. Cuba.
4 I Degree Specialist in MGI. Instructor teacher. Faculty of Medical Sciences Sagua la Grande. Villa Clara. Cuba.
*Corresponding Author: Claribel Plain Pazos. I and II Degree Specialist in MGI. Assistant Professor. Faculty of Medical Sciences Sagua la Grande. Villa Clara. Cuba.
Citation: Melba González Lastre, Amalia Viera González, Elsa Rodríguez Herrera, Isis Esther Martin Alonso, Claribel Plain Pazos, et all (2023), The Role of Second Messengers in the Functioning of the Cell, J, Surgical Case Reports and Images 6(3); DOI:10.31579/2690-1897/146
Copyright: © 2023 Claribel Plain Pazos, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 January 2023 | Accepted: 10 March 2023 | Published: 25 April 2023
Keywords: adenoma; hematom; hypercalcemia; parathyroid; case report
Introduction:
Neck hematoma is a rare but potentially lifethreatening medical condition.Although spontaneous rupture of a parathyroid adenoma with extracapsular hemorrhage is rare, it may cause cervical and mediastinal hematoma, leading to potentially fatal consequences, it should be considered when a non-traumatic sudden neck swelling coexists with hypercalcemia.
Case’s presentation:
This report describes an atypical spontaneous rupture of an asymptomatic parathyroid adenoma in a 42-year-old woman who presented to the emergency room after the acute installation of an unpainful voluminous swelling in the right side of her neck, after eliminating a vascular emergency. Hemodynamically stable, the patient was treated conservatively with a period of observation in hospital, 1 month follow-up imaging with CT confirmed a regression of the half volume of the hemorrhagic lesion and the likely source of hemorrhage as a parathyroid nodule with significant vascularity. The diagnosis was confirmed on histopathological analysis after elective surgical exploration of the neck 3 months of a benign parathyroid adenoma. The patient made a full recovery with immediate normalization of her biochemistry post-operatively.
Discussion:
Spontaneous rupture of a cervical parathyroid adenoma with extracapsular hemorrhage should be considered when a non-traumatic sudden neck swelling coexists with hypercalcemia. The most appropriate treatment, in the absence of dyspnea or dysphagia, we believe that it is preferable to intervene surgically in a delayed manner.
Conclusion:
A high suspicion index is needed, particularly in post-menopausal women, to reach a diagnosis and allow optimal management. Since bleeding may recur, we suggest an independent indication for definitive parathyroidectomy surgery.
Spondylodiscitis is a rare infectious disease that is difficult to diagnose and can affect the intervertebral bodies, spaces, and adjacent intervertebral discs. The incidence of this pathology is increasing [1,2].
Its annual incidence oscillates between 0.5 and 2.5 cases per 100,000 inhabitants and appears to be increasing as a result of the aging of the population, addiction to intravenous drugs, the increase in spinal surgical procedures, and bacteraemia of primary origin. urinary or catheter [3, 4].
It represents 2 to 7% of all osteomyelitis cases and tends to affect the adult population above all (mean age 50 to 60 years) with a clear male predominance [2].
Spondylodiscitis is generally a monobacterial infection and in more than 50% of cases it is due to Staphylococcus Aureus followed by highly negative bacteria such as Escherichia Colliding from 11 to 25%. Coagulase-negative staphylococci, essentially Staphylococcus epidermidis, are usually only involved in spondylodiscitis secondary to surgical interventions or vertebral punctures [5]
There are no specific symptoms or signs of the disease and the diagnosis can take from 2 to 6 months, this darkens the prognosis and increases mortality.
Although it is an infrequent disease, difficult to diagnose, it is interesting for the primary care physician to know its existence and its main clinical manifestations in order to make a proper diagnosis. We present a case seen in our health area and referred to the Arnaldo Miliàn Castro Provincial Teaching Hospital, Rheumatology service where the disease was treated and diagnosed.
Presentation of the Case
A 62-year-old female patient with a personal pathological history of arterial hypertension for which she has been treated with amlodipine (10mg) 1 tablet daily, hypothyroidism with endocrinology follow-up, and repeated urinary tract sepsis in the last two years. She has been diagnosed with Polymyositis for 5 years and associated Sjogren's syndrome, for which she receives treatment with prednisolone (20mg) 1 daily tablet and Cyclophosphamide in monthly pulses. On this occasion, he went to the consultation for presenting pain in the right lumbar region, after physical exertion, irradiating to the upper third of the thigh, making it difficult for him to extend the hip and walk, for approximately 15 days, fever of up to 38.5°C in the first three days that gave way easily with antipyretics. On physical examination, he presented mucosal skin pallor, painful palpable submaxillary adenopathies, in the SOMA, pain at the lumbar level that limits flexion and extension movements and radiates to the upper 1/3 of the right thigh, positive Fabere maneuver on the right side, with the sacroiliac point on the same positive side, limitation and pain in extension movements of the right hip and decreased muscle strength of the shoulder and pelvic girdle. For these reasons, it was decided to refer her to secondary care, indicating her admission to the Arnaldo Miliàn Castro Provincial Teaching Hospital, Rheumatology Service.
Complementary exams of interest:
Hb: 10.6 g/l, leukocytes: 18 x 109/l
Erythrocyte sedimentation rate: 90 mm
Blood glucose: 4.7 mmol/l
Creatinine: 91 mmol/l
Urate:290 mmol/l
TGP: 302 units
GGT: 28 units
FAL: 132
LDH: 327
positive PCR
positive lupus anticoagulant
urine culture positive for Escherichia coli
Mantoux intradermal reaction
Blood culture, Rose Bengal and Brucella serology were negative.
Abdominal ultrasound: reports liver with increased echogenicity without focal lesion, right kidney with irregular contours, with calcifications at the level of the renal parenchyma, right psoas was thickened with respect to its counterpart, with an echogenic image that detaches it with an approximate length of 6.6 cm and with an anteroposterior diameter of 2.3 cm, this muscle being involved with an evolving hematoma.
Abdominal ultrasound: reports liver with increased echogenicity without focal lesion, right kidney with irregular contours, with calcifications at the level of the renal parenchyma, right psoas was thickened with respect to its counterpart, with an echogenic image that detaches it with an approximate length of 6.6 cm and with an anteroposterior diameter of 2.3 cm, this muscle being involved with an evolving hematoma.
A clinical and radiological diagnosis of spondylodiscitis with abscess of the right psoas is made, antibiotic therapy with Cefotaxime 1g + intravenous Metronidazole for 21 days is started, the patient evolved favorably without the need to apply invasive procedures.
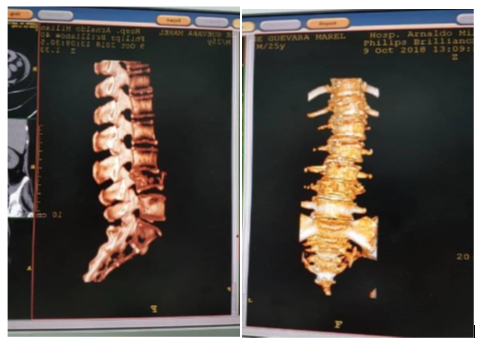
Figure1 & 2: CT scan of the lumbosacral spine
Spondylodiscitis is a rare infection of the spine that is increasing due to greater longevity, improved diagnostic methods, and suspicion of the pathology. It tends to affect the adult population above all (mean age 50 to 60 years) with a clear predominance of the male sex [5,6,7]. The case presented is not the most common since it involved a 62-year-old woman .
The risk factors associated with spondylodiscitis are previous bacteremia, chronic renal failure, diabetes mellitus, hemodialysis, a history of vertebral surgery, arterial hypertension, states of immunosuppression and neoplasms, etc. [2,3] In this case, the patient had a history of polymyositis, which is a rare autoimmune inflammatory myopathy that presents with muscular manifestations, mainly affecting the shoulder and pelvic girdle and requiring the use of immunosuppressive drugs,8 as occurred in this case.
Spondylodiscitis can be associated with epiduritis or a paravertebral abscess. The association of spondylodiscitis and psoas abscess is very infrequent [5,9]. The usual mechanism is hematogenous spread from a respiratory, surgical, and urinary septic focus, as occurred in this case, which presented urinary sepsis with a positive urine culture for Escherichia coli.
There are no specific symptoms or signs of the disease and the diagnosis can take from 2 to 6 months, this darkens the prognosis and increases mortality. The time elapsed between the manifestation of the first symptoms and the diagnosis increases with age, from 30 to 70% of patients do not show any sign of infection [9] In the aforementioned case, the patient presented clinical manifestations that led to the diagnosis.
The blood culture is not specific. Tissue culture helps to differentiate the pathogen. In addition, a study of a probable parasitic or fungal origin should be carried out if there is suspicion. However, taking it by CT-guided percutaneous biopsy is controversial. Conventional radiography is the first imaging method to be used in patients with unclear spinal symptoms, with a sensitivity of 82% and a specificity of 57%. Erosion can be seen in the upper or lower part of the vertebral endplate or kyphosis depending on the virulence of the pathogen involved, the immunological status of the patient and the clinical course of the disease, however, an x-ray without showing signs of spondylodiscitis does not exclude the diagnosis.
Tomography is used in cases where the use of magnetic resonance is contraindicated. Paravertebral abscesses can be better diagnosed with contrast-enhanced CT. In addition, tomography can be used to perform guided biopsies and drainage of smaller abscesses [10]. In this case, the result was very helpful in confirming the diagnosis.
Magnetic resonance is the method of choice in the imaging study to detect spondylodiscitis, in addition, contrasted magnetic resonance helps in the differentiation of degenerative and neoplastic lesions. The specificity is 96% and the sensitivity is 92%, the use of gadolinium can increase the sensitivity to 95.4% [2,3].
The goals of treatment are to eliminate the source of infection, restore the functionality of the spine, and reduce pain. Antibiotic treatment is the therapy of choice and the combination of prolonged antibiotic treatment is essential when surgical intervention is indicated. The patient described resolved with antibiotic treatment, not requiring another intervention.
Surgical management depends on the site and if there are complications such as abscesses in surrounding tissues and the patient's clinical condition, fusion is recommended when there is involvement of the end plates of the vertebral body, while in intraspinal empyema dorsal decompression and evacuation is usually sufficient [5].
The non-specific symptoms and the frequency with which back pain is observed in the general population make it difficult to diagnose spondylodiscitis in primary care. Suspicion should be made in the presence of low back pain with elevated acute phase reactants in patients with autoimmune diseases that represent a situation of immunosuppression, both due to the disease itself and the medication used in its treatment. A correct and early diagnosis is essential, since with adequate treatment the prognosis of patients is good and complications and sequelae are avoided.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
