
Research Article | DOI: https://doi.org/10.31579/2690-1919/148
1 Division of Infectious Diseases
2 Department of Medicine
3 cahn School of Medicine at Mount Sinai, New York NY 10003 United States.
*Corresponding Author: Veenu Gill, Infectious Disease Physician Banner Thunderbird Medical Center 5555 W. Thunderbird Road Glendale, Arizona 85306 United States
Citation: Veenu Gill, Jorg Ruhe, David C. Perlman, (2021) Specific Magnetic Resonance Imaging Findings as Predictors of Osteomyelitis in Routine Clinical Practice. Journal of Clinical Research and Reports, 7(2); DOI:10.31579/2690-1919/148
Copyright: © 2021 Veenu Gill, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 March 2021 | Accepted: 12 March 2021 | Published: 22 March 2021
Keywords: osteomyelitis; bone biopsy; histology; MRI
Background: The gold standard for the diagnosis of osteomyelitis is histopathology combined with positive bone cultures. Magnetic Resonance Imaging (MRI) is often used to aide diagnosis and guide treatment decisions. The purpose of the study was to examine the association of MRI findings with, and their sensitivity and specificity in identifying osteomyelitis as proven by bone histopathology and bone culture in routine clinical practice.
Materials and Methods: A retrospective analysis of patients with bone specimens obtained by biopsy or at resection for suspected osteomyelitis during 2010-2014 at an academic medical center in New York City. We used bivariate analysis to compare findings of patients who did or did not have osteomyelitis confirmed on histopathology (Analysis 1) and those who had either bone histopathology demonstrating osteomyelitis, positive bone cultures or both or who had neither (Analysis 2).
Results: We identified 103 patients with an MRI in the week prior to bone biopsy or bone resection. In Analysis 1, 52 (50.5%) of 103 patients had osteomyelitis confirmed on histopathology. In Analysis 2, 72 (70%) patients had proven osteomyelitis. These groups with and without osteomyelitis did not differ significantly with respect to the frequency of marrow edema, cortical erosions, decreased T1 signal or increased T2 signal in either analysis and the sensitivity and specificity of MRI findings for detecting osteomyelitis was lower than reported in prior studies.
Conclusions: Based on the above results, clinicians should be aware that the sensitivity and specificity of MRI findings for histologic and microbiologic osteomyelitis may be less in real world practice than is reported in formal studies.
Osteomyelitis is a major public health issue. Osteomyelitis contributes to one in 675 United States (US) hospital admissions each year or about 50,000 cases annually [1]. The direct medical charge per episode of osteomyelitis is estimated to be $35,000 US [2]. The gold standard for the diagnosis of osteomyelitis is evidence of bone infection on pathologic specimens obtained through biopsy, debridement or resection) plus the presence of positive bone cultures [2, 3]. A variety of radiologic studies can be useful both in guiding biopsy or surgical intervention and in the presumptive diagnosis of osteomyelitis, including plain radiography, nuclear medicine studies, computed tomography (CT) or particularly Magnetic Resonance Imaging (MRI) [4].
MRI is a key imaging modality for the detection of osteomyelitis because it has superior overall sensitivity approaching 90%, but it has a lower specificity ranging from 70-80% in different clinical studies depending upon the diagnostic criteria used and specific MRI findings considered [4,5,6]. In prospective studies with double blind reading of both MRIs and of bone pathology, MRI can identify certain findings which are highly sensitive e.g., bone marrow edema and can reveal findings which can be highly specific e.g., cortical destruction [5,6,7]. However, MRI cannot always distinguish between infection and non-infectious etiologies such as Charcot arthropathy, particularly when the relatively non-specific finding of bone marrow edema is identified [8, 9]. Further, in routine clinical settings, it is not uncommon to encounter situations in which the sole MRI finding e.g. bone marrow edema is sensitive but nonspecific and in which MRI findings may then interpreted as ‘consistent with’ or ‘not able to exclude’ osteomyelitis; treatments decisions may then be made based on these nondefinitive imaging findings and the clinical context [6,7,9].
MRI and other imaging studies may inform the clinical decision to do a bone biopsy or to proceed to resection, yet there are many situations in which bone specimens are not, or cannot, be obtained. These radiographic (including MRI) findings themselves, often in the presence of overlying or adjacent skin and soft tissues infections, may lead to the institution of empiric antibiotic therapy prior to, or instead of, bone specimens being obtained for pathologic or microbiological analysis. Hence, another issue that arises in routine clinical practice is that patients may have received antibiotics prior to either bone biopsy or surgical resection, thus potentially reducing the sensitivity of subsequently obtained bone cultures [10,11,12].
To our knowledge, there are few data specifically correlating specific MR findings with bone biopsy and intraoperative bone cultures in routine “real-world” clinical practice. We sought to examine the correlation between specific MRI findings and pathologic evidence of osteomyelitis on bone specimens and on intraoperative bone cultures in routine practice at an academic medical center. The aim of the study was to identify specific MRI findings of osteomyelitis as confirmed by bone histopathology and cultures.
Study design:
We conducted a retrospective review of electronic pathology records at our institution for the years 2010-2014 using search terms "bone inflammation", " bone biopsy" and "osteomyelitis". All adult aged >18 years) patients seen at our institution from 2010-2014 who had a bone biopsy or bone resection as part of management of possible or suspected osteomyelitis and had an MRI performed within one week prior to the bone specimen being obtained, were identified. Among this group who had bone pathologic specimens, we subsequently identified those patients who had an MRI of the affected area within one week prior to the date the bone specimen was obtained, to identify patients with bone pathologic specimens, MRIs and a clinical a priori consideration of osteomyelitis.
The patients’ medical records were reviewed to identify baseline characteristics including the presence of comorbidities, descriptions of the involved area, the presence or absence of erythema, purulence, ulcers, ulcer size, exposed bone, and whether ulcers probed to bone. Laboratory values such as sedimentation rate, C-reactive protein, white blood cell count, and the route and duration of antibiotics before the specimens were recorded. MRI reports were reviewed to identify specific findings noted and final interpretations; pathology reports were reviewed to identify specific findings noted and final interpretations, and included pathologic findings such as the presence or absence of bone necrosis, acute or chronic inflammation and gram stain results. We also identified whether cultures of intraoperatively obtained bone specimens were performed and the results of these cultures.
All data gathered was entered into an Excel spread sheet. Two separate analyses were conducted. In the first analysis (Analysis 1), clinical characteristics and MRI findings of patients who had osteomyelitis confirmed on histopathology and those who did not were compared. In the second analysis (Analysis 2), clinical characteristics and MRI findings of patients who had either bone histopathology demonstrating osteomyelitis, positive bone cultures or both (=proven osteomyelitis) were compared with those who had neither (=no proven osteomyelitis)
Statistical analysis:
Bivariate analyses using the Pearson's 2 test, the Fisher's exact test, and the Mann-Whitney U test were performed to compare categorical and continuous variables, respectively.
The sensitivity, specificity, positive and negative predictive values of specific individual MRI findings for the identification of osteomyelitis (as defined in Analysis 1 and 2) were calculated. We also calculated the sensitivity, specificity of the combined MRI findings of a) marrow edema plus cortical erosions, and b) decreased T1 signal intensity plus increased T2 signal intensity.
A total of 520 distinct patients were identified in the study time period 2010-2014 as having possibly relevant bone specimens. Of those, 417 were excluded for the following reasons: resection for anatomic (noninfectious) bone deformity (82), pathologic diagnosis of malignancy (146), wrong specimen (42), incomplete records where relevant data were contained in outpatient records which were not available (120), no MRI done (20) and duplicate records (7). This resulted in 103 patients who were included in the study and who had both MRI and pathology records available (Table 1).
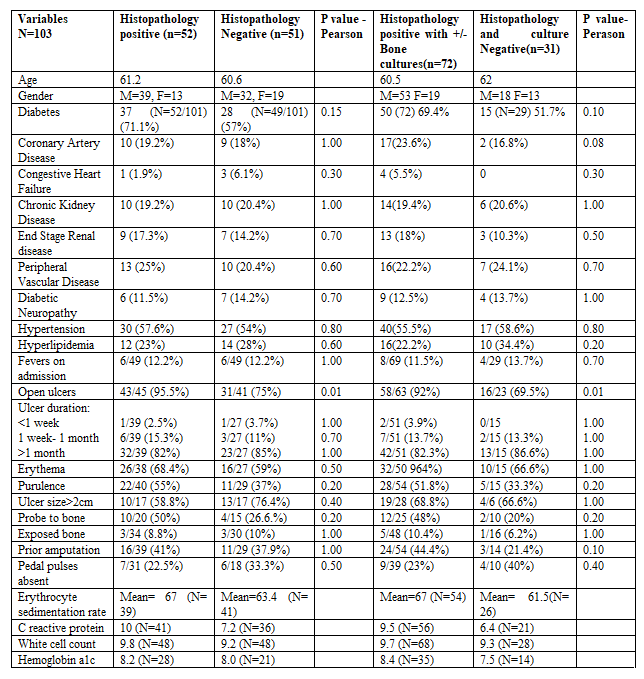
Among the 103, the mean age of patients in the total cohort was 60 years. 64% had diabetes mellitus, 23% had peripheral vascular disease and 12% had diabetic peripheral neuropathy.
Analysis 1
Of the 103 patients, 52 (50.5%) patients did have osteomyelitis confirmed on histopathology and 51 (49.5%) patients had negative histopathologic results. The only finding on physical examination significantly associated with osteomyelitis was presence of an open ulcer (p=0.01; Table 1). Probing to bone, ulcer size, exposed bone and signs of peripheral vascular disease were not significantly associated with the presence of underlying osteomyelitis. The mean ESR value was 65mm/hour and the mean CRP value was 8.7mg/L. Eighty-three (80.5%) of the 103 studied had baseline X-rays performed (Table 2).
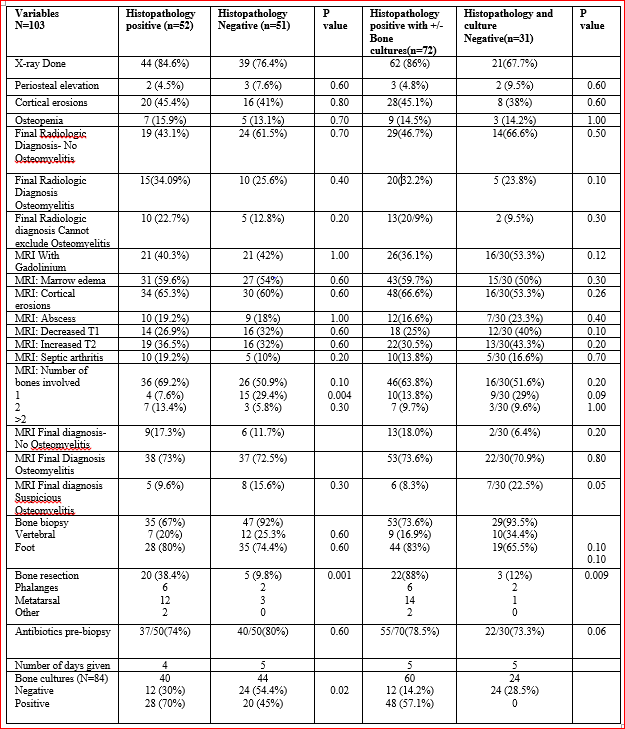
Only 6% of the patients had periosteal elevation on x-ray whereas 43% had cortical erosions. Only 25 out of 103 patients (30.1%) had findings identified on plain x-ray interpreted as compatible with osteomyelitis (Table 2). There was no significant difference with regard to the presence of cortical erosions among those with or without osteomyelitis on histopathology (Table 2).
42(41%) of the 103 of the had MRIs performed with gadolinium. The two groups did not differ significantly in the findings of marrow edema [27(54%) vs. 31(59.6%), p=0.60], cortical erosions
[30(60%) vs 34( 65%), p=0.60], decreased T1 signal [16(32%) vs. 14(26.9%), p=0.60] or increased T2 signal [16(32%) vs. 19(36.5%), p=0.60]. The majority of the patients (79.6%) underwent bone biopsy. Sixty-three biopsies were of bones of the foot and 19 were vertebral bone specimens. Twenty-five (24.2%) of 103 underwent resection of the affected bone, 20 (38.4%) of whom had confirmed osteomyelitis on histology. Of the 19 patients who had a vertebral biopsy performed for suspected vertebral osteomyelitis, 7 (20%) had osteomyelitis confirmed on histopathology.
Data on antibiotic use prior to obtaining bone specimens were available for 100 of the 103 patients. Seventy-seven (77%) patients received one or more systemic antibiotics for a mean of five days prior to bone biopsy or resection.
We calculated the sensitivity and specificity of either marrow edema, cortical erosions or the combination of both to predict the presence of osteomyelitis on histopathology. Marrow edema alone had a sensitivity of 59.6%, a specificity of 46%, a positive predictive value of 53.4% and a negative predictive value of 52.2% (Table 3).
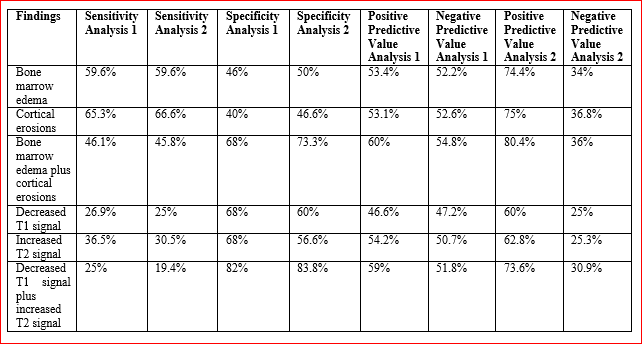
Analysis 1: compared those with histopathologic confirmed osteomyelitis (n=51) to those without histopathologic confirmed osteomyelitis (n=52); Analysis 2 compared those with histopathologic osteomyelitis, positive bone cultures or both (n=72) to those with neither (n=31).
The presence of cortical erosions had a sensitivity of 65.3% with a specificity of 40%. The positive predictive and negative predictive values of cortical erosions were 53.1% and 52.6% respectively (Table 3).
The presence of both marrow edema and cortical erosions had a specificity of 68% with a sensitivity of 46.1%. The positive predictive value of the combination of both bone marrow edema and cortical erosions was 60% and the negative predictive value was 54.8%. Changes in the T1 and T2 signal intensities by themselves had sensitivities of 26.9% and 36.5% respectively; the specificity of each was 68%. The combination of a decreased T1 signal and an increased T2 signal intensity had a specificity of 82% with a sensitivity of 25%; the positive predictive value of the combination was 59% with a negative predictive value of 51.8% (Table 3).
Analysis 2
Data on bone cultures was available for 84 patients; 48 (57%) of these were positive. Of the 48 patients with positive bone cultures, all had osteomyelitis confirmed on histology. 36 patients had negative bone cultures; 24 of which were negative on histopathologic diagnosis and 12 were positive on histology.
A total of 72 (69%) of the 103 patients had either osteomyelitis on histopathology, positive bone cultures or both (=proven osteomyelitis); 31 (31%) had neither (=no proven osteomyelitis; Table 1). Ulcer size, the duration of the ulcerative lesions and positive results on the probe to bone maneuver were not significantly different between the two groups; neither ESR nor CRP differed between the two groups (Table 1).
The presence on X-ray of periosteal elevation, cortical erosions and osteopenia did not statistically differ between the two groups (Table 2). There was also no difference with regard to frequency of MRI findings such as cortical erosions, T1 and T2 signal intensity changes and marrow edema. Of 103 patients, 82 (79.6%) patients had bone biopsy and 25 (24.2%) of 103 had bone resected. Twenty-two (88%) of the 25 resected bones had histopathologic findings of osteomyelitis. Seventy-seven (77%) of the 100 patients for whom data were available, had received one or more systemic antibiotics for a mean of 5 days prior to bone biopsy. The most commonly prescribed antibiotics were vancomycin, penicillin derivatives and cephalosporins. Bone cultures were performed for 84 people, 48 (57.1%) of whom had positive cultures. All 48 patients with positive bone cultures also had histological evidence of confirmed osteomyelitis on pathology.
The organisms most commonly isolated from bone cultures were: methicillin sensitive Staphylococcus aureus (MSSA), methicillin resistant Staphylococcus aureus (MRSA), coagulase negative Staphylococci, Streptococcus species, Corynebacterium, Enterococcus species; among gram negative bacteria, Pseudomonas species were common. Forty one of 103 patients had deep (non-bone) wound cultures obtained; 31 (87%) were positive and the most common organisms were MSSA, MRSA and Streptococcus species.
We calculated the sensitivity and specificity of marrow edema, cortical erosions and a combination of edema plus erosions to predict the presence of proven osteomyelitis as identified by either histopathology, bone cultures or both, compared to no proven osteomyelitis. Marrow edema alone had a sensitivity of 59.6% and a specificity of 50% with a positive predictive value of 74.4% and a negative predictive value of 34% (Table 3). The presence of cortical erosions had a sensitivity of 66.6% and specificity of 46.6%. The positive predictive and negative predictive value of cortical erosions were 75% and 36.8% respectively.
The presence of marrow edema and cortical erosions had a specificity of 73.3% with a sensitivity of 45.8%. The positive predictive value of the combination was 80% with a negative predictive value of 36%. Changes of the T1 or T2 signal intensity alone had sensitivities of 25% and 30.5%, respectively. The specificity of each was 60% and 62.8%, respectively. The combination of a decreased T1 signal and an increased T2 signal intensity had a specificity of 83.8%, with a sensitivity of 19.4%. The positive predictive value of the combination was 73.6%; the negative predictive value was 30.9%.
Osteomyelitis continues to cause significant morbidity and health care costs (1). Despite the availability of diagnostic procedures including biopsy and a range of imaging tests such as MRI osteomyelitis continues to pose diagnostic challenges. Biopsies are not always feasible, and consequently clinicians are often required to rely on imaging tests to support or exclude the diagnosis. However, despite data in which double blind readings of MRIs often have high sensitivity and specificity for the diagnosis of osteomyelitis confirmed by double blind histopathologic analysis in study settings (5,6,7,10,11), our data suggests that MRIs may have a lower sensitivity and specificity for the diagnosis of osteomyelitis in routine clinical practice.
The presence of single findings compatible with osteomyelitis e.g. bone marrow edema, cortical erosions, T1 signal or T2 signal changes were associated with sensitivities in the 25-65% range, with specificities of 40-68%. The presence of combinations of both bone marrow edema and cortical erosions yielded roughly comparable sensitivity, specificity and negative predictive values, but did yield somewhat superior positive predictive values in the 60-80% range. Similarly, a combination of T1 and T2 signal changes had a lower sensitivity (approximately 19-25%), but a higher specificity of approximately 82-84%. This is in contrast to a prior study that reported a sensitivity close to 80% and a specificity of 72% (11).
More patients had open ulcers on physical exam in the groups without osteomyelitis in both analyses (approximately 92-95%) than in the groups without evident osteomyelitis, suggesting that this commonly used physical exam finding may not be a reliable predictor of osteomyelitis. 20(24%) of the 83 patients had positive bone cultures in the absence of histopathologic evidence of osteomyelitis, suggesting either that histopathology alone may either miss some cases of true bone infection or that cultures may have been falsely positive because of contamination by wound colonizing flora or skin commensals.
Many limitations should be noted. The majority of pathology specimens were from biopsy rather than bone resection; this could potentially cause sample bias. Further, this was a retrospective analysis of routinely generated clinical MRI and pathologic data. Neither MRIs nor pathologic specimens were re-reviewed, nor were they double read, both methods which might enhance the diagnostic accuracy of both procedures, and as has been done in idealized setting such as prospective studies (10, 11). The interpretation of the MRI findings used in our study was solely based on those documented in the final radiologist MRI reports; not all MRI reports specifically addressed the presence or absence of each potential MRI finding. Similarly, the final pathologic reports varied in the degree of detail provided, again differing from the rigor that might be obtained by blinded or double review in a prospective study. Further, MRI findings and pathology specimens were not all reviewed by the same radiologist or pathologist as part of the study protocol. Thus, the potential inter-reader variability may have affected the sensitivity and specificity of MRI findings in our study. However, while either prospective blinded double reading of both MRIs and histopathology or post-hoc re-review of MRI and histopathologic reports might have enhanced the ability to identify the potential of MRI to identify or exclude osteomyelitis under ideal conditions, such as in formal studies, the value of examining the results based on the routinely generated clinical reports is that this analysis then more accurately reflects the data routinely available to clinicians in real world practice.
We did not observe significant difference in the frequency of specific MRI findings or in the final MRI impression between patients with and without proven osteomyelitis. The sensitivity, specificity, positive and negative predictive value of MRI in the detection of osteomyelitis identified in this clinical setting were lower than that generally reported in formal clinical studies. Clinicians should be aware that the correlation between MRI findings and histopathologic or microbiological results obtained in routine practice may be lower than suggested by the literature. Further studies in well-defined but real-world clinical cohorts are warranted.
The authors report no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
