
Research Article | DOI: https://doi.org/10.31579/2578-8965/008
1 Department of obstetrics and gynecology, Ain Shams University, Egypt.
*Corresponding Author: Amr El Helali, Department of obstetrics and gynecology, Ain Shams University, Egypt, E-mail: ayman_gamal007@yahoo.com
Citation: Amr abd el Fattah El Helali , Amal el Shabrawi El Sayed, Wesal Hamdi Ali Hassan, (2018) Sonographic Versus Clinical Fetal Weight Estimation Accuracy. J. Obstetrics Gynecology and Reproductive Sciences. 2(1); Doi: 10.31579/2578-8965/008
Copyright: © 2018 Amr El Helali et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 March 2018 | Accepted: 07 May 2018 | Published: 08 May 2018
Keywords: Fetal weight, Ultrasound assessment of fetal weight, clinical assessment of fetal weight.
Background: Sonographic fetal weight estimation is an important component of antenatal care. It was found to be more reliable method to establish fetal weight at term and more consistent in various period of gestations.
Aim of study: to compare clinical and sonographic methods for assessment of fetal weight regarding sensitivity, specificity and accuracy.
Subjects and Methods: The study recruited 100 women scheduled for delivery from ante-natal care clinic with 38 weeks or more of gestation. Fetal weight was assed clinically and by ultrasound. Both techniques were compared and analyzed.
Results: Ultrasound assessment of fetal weight showed better performance than the clinical method regarding absolute errors and error percentages. Ultrasound assessment showed better sensitivity and specificity in detecting fetal weight > 3500 gm. Moreover, it showed less bias on Bland–Altman plot analysis.
Conclusions: Ultrasound assessment of fetal weight is safe, reliable and sensitive method of fetal weight estimation.
The estimation of the fetal weight is of major interest in many situations when the route of delivery has to be determined including breech presentations, diabetes and suspected macrosomia. In fact, delivery of a macrosomic fetus can be linked with significant maternal and perinatal morbidity. Detection of the macrosomic fetus prior to delivery could have a significant impact on reducing that morbidit [1-3].
On the other hand, in imminent preterm birth at the limit of viability between 23(0/7) and 26(0/7) weeks of gestation, it is crucial to determine fetal weight to help manage expected complications. Moreover, estimation of fetal weight proved to be useful in prediction of future events including childhood obesity [4-6].
Clinical estimation and ultrasonographic fetal weight estimation are the 2 methods commonly used to predict fetal weight. Clinical estimation of fetal weight is a routine practice in the delivery room. It has an important role in the assessment and planning of the delivery progress, it allows the clinician to predict possible complications such as macrosomia and plan for obstetric interventions where needed [7-9].
For sonographic assessment of fetal weight, many formulas are used. However, they differ in accuracy. In addition, accuracy differs according to the day of weight estimation. However, it should be noted that high maternal weight, height, body mass index, multiparity, older maternal age, diabetes, and fetal male sex were associated with underestimation of sonographic assessment of fetal weight [10-12].
In a recent study, comparison between clinical and sonographic methods showed significantly better sensitivity, specificity and accuracy of sonographic methods when compared with clinical tools. However, in another study no significant differences were found between clinical and sonographic methods for assessment of fetal weight during labor [13-15].
The present study aims to compare clinical and sonographic methods for assessment of fetal weight regarding sensitivity, specificity and accuracy.
The present study is a prospective comparative study. It was conducted at Ain Shams University Maternity Hospital after obtaining informed consent from all participants. One hundred pregnant woman scheduled for delivery from ante-natal care clinic were recruited for the study. They were selected according to the following inclusion criteria: Singleton pregnancy, gestational age after 38 weeks, normal amniotic index and BMI less than 30 kg/m2. Exclusion criteria included twin pregnancy, gestational age before 38weeks of gestation, abnormal amniotic index, obesity and congenital malformations.Participants included in following study were subjected to careful history taking, full clinical and obstetrical examination.Clinical assessment of fetal weight was achieved by single practitioner (senior resident), by measuring length from mid-point of upper edge of symphesis pupis to the highest fundal point to give fundal height [FH] in centimeter then measuring abdominal girth [AG] by measuring women waist in centimeter then calculate fetal Weight in grams by (FH × AG).Sonographic assessment of fetal weight was achieved by two dimensional ultrasound and single sonographer by measuring biparietal diameter (BPD), head circumference (HC), abdominal circumference (AC) and femur length (FL) then fetal weight was calculated using Hadlock formula where fetal weight = (log10 2D estimate = 1.5115 + 0.0436 [abdominal circumference] + 0.1517 [femur length] – 0.00321 [abdominal circumference × femur length] + 0.0006923 [biparietal diameter × head circumference]). Women were delivered within 3 days, the neonate was weighted, then the clinical and sonographic weight were compared to the actual weight.Data were collected, tabulated, then analyzed using IBM© SPSS© Statistics version 22. Normally distributed numerical data were presented as mean and SD, and skewed data as median and interquartile range. Qualitative data were presented as number and percentage. Comparison of normally distributed numerical data were done using the unpaired Student t test. Categorical data were compared using the chi-squared test or Fisher’s exact test, when appropriate. Correlation analysis was performed using Pearson’s correlation coefficient. Accuracy of fetal weight estimation was examined by calculating the absolute error (EFW - BW) and error percentage using the formula (EFW - BW / BW) ´ 100.
Reliability of clinical and sonographic methods of fetal weigh was determined using receiver operator characteristic (ROC) where area under the curve (AUC) sensitivity, specificity were determined. Bland-Altman plot analysis was used to detect agreement between investigations.
Basic data of 100 women included in the study are shown in table-1.
| Age (years) | Range | 19.0 - 32.0 |
| Mean ± SD | 25.7 ± 4.0 | |
| Weight (Kg) | Range | 60.0 - 82.0 |
| Mean ± SD | 72.2 ± 5.1 | |
Height (m) | Range | 1.5 - 1.72 |
| Mean ± SD | 1.62 ± 0.05 | |
BMI (Kg 2) /m | Range | 22.8 - 29.9 |
| Mean ± SD | 27.3 ± 1.6 | |
| < 25 | 11 (11.0 %) | |
| ≥ 25 - < 30 | 89 (89.0 %) | |
| Gestational age (days) | Range | 267 - 298 |
| Mean ± SD | 274.6 ± 5.7 | |
Parity | Range | 0 – 3 |
| Mean ± SD | 1.5 ± 1.1 | |
| 0 | 21 (21.0 %) | |
| 1 | 36 (36.0 %) | |
| 2 | 19 (19.0 %) | |
| 3 | 24 (24.0 %) | |
| Mode of delivery | Vaginal | 43 (43.0 %) |
| Cesarean Section | 57 (57.0 %) | |
| Clinically estimated fetal weight (gm) | Range | 2784.0 - 4485.0 |
| Mean ± SD | 3545.0 ± 456.9 | |
| US estimated fetal weight (gm) | Range | 2369.0 - 4349.0 |
| Mean ± SD | 3397.7 ± 487.7 |
Table 1: Basic data in the studied women (n=100).
The studied women had an age of 25.7 ± 4.0 years, a BMI of 27.3 ± 1.6 Kg/m2 a gestational age of 274.6 ± 5.7 days and a parity of 1.5 ± 1.1 deliveries. Vaginal delivery was the mode of delivery in 43 women while 57 women were delivered by CS. Clinical fetal weight estimation in the studied women ranged from 2784.0 - 4485.0 grams with a mean ± SD of 3545.0 ± 456.9 grams. Ultrasound fetal weight estimation ranged from 2369.0 - 4349.0 grams with a mean ± SD of 3397.7 ± 487.7 grams.
Comparison between clinical and ultrasound fetal weight estimates and the actual birth weight revealed that both estimates are significantly higher the actual birth weight. In addition, it was shown that clinical estimate is significantly higher ultrasound estimate. Comparing clinical and ultrasound methods showed significantly higher mean absolute error and mean error percentages in the clinical method. Comparison between clinical and ultrasound methods regarding absolute mean error at different gestational ages showed significantly higher absolute mean error in the clinical method at different gestational ages. Comparison between clinical and ultrasound methods regarding error percentages showed significantly higher frequency of high error percentages rates in the clinical methods when compared with the ultrasound methods (Table-2).
| Clinical | Ultrasound | P | |
| Mean absolute error (gm) | 495.6 ± 317.5 | 296.9 ± 308.0 | 0.0001* |
Mean error percentages (%) | 16.3 ± 11.1 | 9.9 ± 11.1 | 0.0001* |
| Absolute mean errorat different gestational ages | |||
(n=23) | 410.1 ± 256.3 | 190.6 ± 151.7 | 0.004* |
(n=41) | 526.9 ± 342.0 | 337.5 ± 350.9 | 0.002* |
(n=30) | 486.6 ± 300.0 | 284.4 ± 285.9 | 0.007* |
(n=6) | 400.7 ± 299.9 | 240.0 ± 295.2 | 0.028* |
| Error percentages | |||
| 25 | 48 | 0.001* |
| 7 | 21 | 0.004* |
| 16 | 10 | 0.21 |
| 19 | 1 | 0.0001* |
| 15 | 5 | 0.018* |
| 18 | 15 | 0.57 |
Table-2: Comparison between clinical and ultrasound methods regarding mean absolute error and mean error percentages, absolute mean error at different gestational ages and error percentages
Correlation analysis between clinically estimated fetal weight and the clinical data showed significantly direct correlation between Clinical EFW and gestational age, ultrasound EFW and actual BW. Also, correlation analysis between clinically estimated fetal weight and the clinical data showed significantly direct correlation between Clinical EFW and gestational age, ultrasound EFW and actual BW (Table-3)
| Clinical EFW | Ultrasonic EFW | |||
| r | p | r | p | |
| Maternal age | -0.05 | 0.62 | -0.14 | 0.14 |
| Maternal BMI | 0.06 | 0.53 | 0.13 | 0.2 |
| Parity | -0.02 | 0.82 | -0.02 | 0.78 |
| GA | 0.27 | 0.007* | 0.36 | 0.0001 |
Ultrasound EFW | 0.58 | 0.0001* | 0.58 | 0.0001* |
| Actual BW | 0.49 | 0.0001* | 0.69 | 0.0001* |
Table-3: Correlation between clinical and ultrasound EFW and the clinical data
Value of clinical and ultrasound EFW determination in predicting actual fetal weight > 3500 gm is shown in table-4 and fig. 1. Ultrasound EFW had higher AUC and better sensitivity.
| Clinical EFW | Ultrasound EFW | |
| Cut-off | 3811 | 3550 |
| AUC | 0.76 | 0.85 |
| P | 0.0001 | 0.0001 |
| Sensitivity | 66.7 % | 80.0 % |
| Specificit | 82.9 % | 81.4 % |
Table-4 : Value of clinical and ultrasound EFW determination in predicting actual fetal weight> 3500 gm
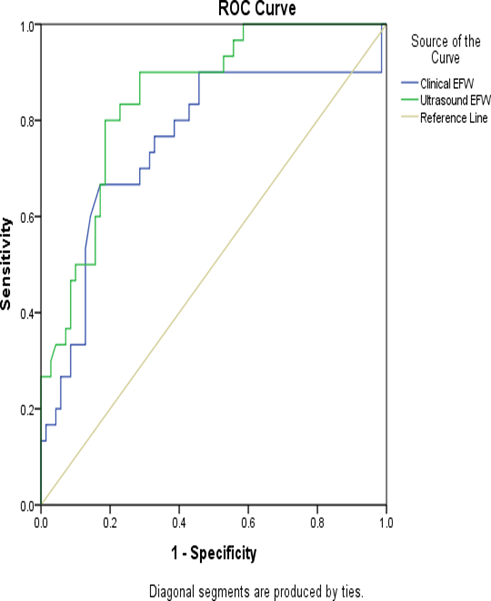
Fig. (1) ROC analysis for predicting actual fetal weight > 3500 gm by clinical and ultrasound methods
Bland–Altman plot analysis for agreement between clinical and ultrasound EFW is shown in fig. 2 and 3 respectively. While both plots shows that most differences lie within the higher and lower confidence intervals, the bias is notably lower in the ultrasound plot.
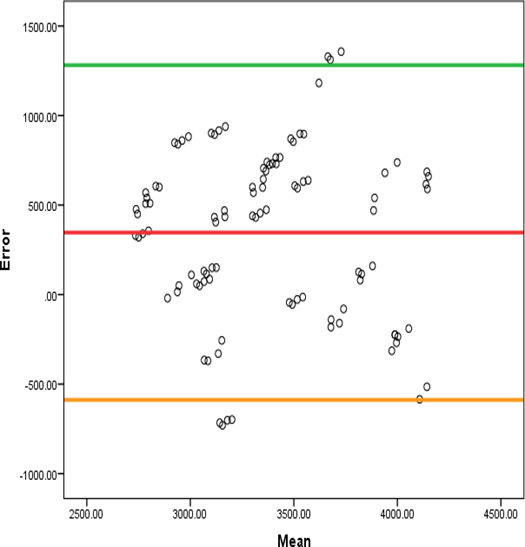
Fig. (2) Bland–Altman plot for clinical EFW- actual birth weight agreement.
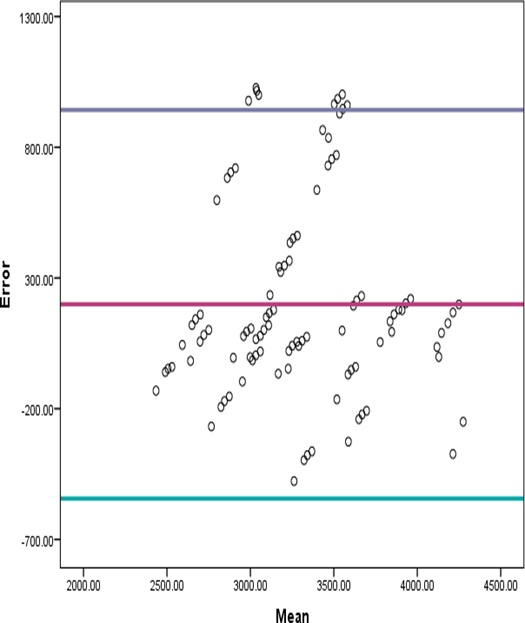
Fig. (3) Bland–Altman plot for ultrasound EFW- actual birth weight agreement.
Perinatal mortality and morbidity remains a chief health issue strongly corelated with fetal growth pattern, an issue of research interest showing that fetal growth issues is correlated to the risk of common non communicable diseases in adulthood.
Fetal weight assessment is one of the most vital aspects of antenatal care. At full term, fetal weight evaluation is an important factor for the clinical decision about the mode of delivery and the timing of induction .Additionally, estimated fetal weight (EFW) and fetal biometry are complementary measures used to screen for fetal growth disturbances.
Sonographic fetal weight estimation is an important component of antenatal care. However, although numerous methods were developed to compute the sonographic fetal weight estimation from fetal parameters, a high random error features most of them, undermining the accuracy of the sonographic fetal weight estimation and probably influencing clinical decision making concerning follow up of gestation and delivery [1-5]. On the other hand, ultrasound was found to be more reliable method to establish fetal weight at term and more consistent in various period of gestations. Clinical method can be reliably used to screen large babies in centers where ultrasound has limited availability [7-9].
The current research study aimed to compare and contrast clinical and sonographic methods for assessment of fetal weight regarding sensitivity, specificity and accuracy. The study recruited 100 women scheduled for delivery from ante-natal care clinic with 38 weeks or more of gestation. Fetal weight was assed clinically and by ultrasound. Both techniques were compared and analyzed. In the current study, comparison between clinical and ultrasound fetal weight estimates and the actual birth weight revealed that both estimates are significantly higher the actual birth weight. In addition, it was shown that clinical estimate is significantly higher than ultrasound estimate. This is in harmony with the study of on 200 term pregnant women. They used three formulae for the estimation of fetal weight at term; the Hadlock formula for the USG method, and two different formulas for clinical methods, maternal symphysis-fundal height and abdominal circumference at the level of umbilicus. The authors concluded that all three methods statistically overestimated birth weight for the high and normal birth weight groups. However, in a previous research study performed comparing the accuracy of clinical and sonographic methods of predicting fetal weights at term, clinical fetal weight estimation was significantly higher actual weight while ultrasound assessment was significantly lower actual weight [10-13].
The discrepancy between different studies may be attributed to different body mass indexes of the studied women. The study of highlighted the value of BMI in modulating the sonographically assessed fetal weight where increased BMI was associated with increased estimates of ultrasound fetal weight assessment [15].
In addition, it was found that comparing clinical and ultrasound methods showed significantly higher mean absolute error and mean error percentages in the clinical method. Furthermore, we noted that comparison between clinical and ultrasound methods regarding absolute mean error at different gestational ages showed significantly higher absolute mean error in the clinical method at different gestational ages. Moreover, comparison between clinical and ultrasound methods regarding error percentages showed significantly higher frequency of high error percentages rates in the clinical methods when compared with the ultrasound methods.[17]
This is in accordance with a prior research performed which compared the accuracy of clinical and ultrasound methods of fetal weight estimation in 200 consecutive term pregnancies. They noted that ultrasound assessment had significantly lower absolute errors and error percentages as compared to clinical methods [10].
Likewise, another research study similarly performed compared the accuracy of sonographic versus clinical methods of fetal weight estimation in 200 term women. The study found significantly lower mean percentage error and mean absolute percentage error with ultrasonic fetal assessments in babies weighing less than 4 kg [4].
More recently a group of researchers, performed a cross sectional study over a period of 6 months. All singleton term mothers with cephalic presentation and intact membranes with ultrasound examination done within a week were included in the study. The study found significantly lower mean error, absolute error and error percentages in the ultrasonic weight assessment versus clinical fetal weight assessment as contrasted to the actual weight of the studied babies [7-8].
Correlation analysis between clinically estimated fetal weight and the clinical data showed significantly direct correlation between Clinical EFW and gestational age, ultrasound EFW and actual BW likewise, These findings are in accordance with the a fore mentioned previous research.
Moreover, the study of by a research group evaluated the accuracy of fetal weight prediction by ultrasonography in 145 cases and found a significant, yet low, linear relationship between birth weight and estimated fetal weigh
Importantly, it was shown that ultrasound EFW had higher AUC and better sensitivity and specificity for the estimation of fetal weight > 3500 gm. The reliable sensitivity and specificity of ultrasound fetal weight estimation was also reported by the study who compared the accuracy of ultrasound, clinical and maternal estimates of fetal weight in 246 parous women with singleton, term pregnancies. In their work, ultrasound assessment of fetal weight was comparable to clinical methods.
In addition, reported that the sensitivity and specificity of clinical method and ultrasonographic method for identifying fetal birth weight above 3500 gm was 69.23; 65.67% and 46.15; 80.60%, respectively. Moreover, the study of in their work, they compare the accuracy of abdominal palpation with that of ultrasound performed by different examiners to estimate fetal weight. The authors showed that ultrasound notably dominated the clinical methods in the accurate assessment of fetal weight.
Bland–Altman plot analysis showed that most differences lie within the higher and lower confidence intervals, the bias is notably lower in the ultrasound plot. This is in agreement with the study of. In their work, they proposed to sonographically estimate fetal weight at term in a convenience sample of 282 women and to compare estimated with actual birth weights to determine the validity of estimated fetal weights. The study found that Bland and Altman plot analysis showed strong agreement between EFWs and ABWs because it was only in very few instances that differences between the two fell outside the 95% limit of agreement.
Also, in aprior study involving 500 singleton gestations, sonographic assesments were performed. Estimated fetal weights have been calculated and compared with the corresponding birth weights. According to Bland-Altman analysis, bias was -85.06 g (95% limits of agreement: -663.33 to 494.21) indicating good agreement between actual and ultrasound fetal assessments.
Sonographic evaluation of fetal weight displayed superiority than the clinical approach as regards absolute errors and error percentages. Sonographic examination additionally revealed better statistical sensitivity and specificity in detection of fetal weight > 3500 gm. Moreover, it showed less bias on Bland–Altman plot analysis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
