
case report | DOI: https://doi.org/10.31579/2692-9392/081
1Faculty of Medecine and Pharmacy of Agadir. University Ibn Zohr. Morocco
2Hematology Department. Center University Medical of Agadir. Morocco
3Laboratory of Hsitology Souss. Agadir. Morocco
*Corresponding Author: Salma Fares, Faculté de Médecine et de Pharmacie d’Agadir. Quartier Tilila Bp 7519 Agence Abb Agadir Al Fidia Cp80060.
Citation: Salma Fares, Adil Taoufik, Aissam Maataoui, Ouadie Qamouss, Kaoutar Sokori. (2021) Solitary Ovarian Plasmocytoma: A Rare localization of Extramedullary Plasmocytoma. A case Report. J. Archives of Medical Case Reports and Case Study, 4(5); DOI:10.31579/2692-9392/081
Copyright: © 2021 Salma Fares, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 September 2021 | Accepted: 21 September 2021 | Published: 25 September 2021
Keywords: solitary plasmocytoma; extramedullary; ovary; multiple myeloma
Background: Solitary plasmacytoma is a rare malignant neoplasm of plasma cells accounting 5-10% of all plasma cell dyscrasias with extramedullary plasmocytoma in 3- 5%. Their localization in the female genital tract is quite rare, either as solitary plasmacytomas or as part of a disseminated MM. Solitary ovarian plasmocytoma is extremely rare. Case: A 52-year-old woman, presented presented postmenopausal recurring episodes of metrorrhagia with left ovarian mass. She was diagnosed with solitary ovarianplasmocytoma without systemicdisease. The patient underwent complete surgery resection and a full work up to rule out multiple myeloma that objectived a small serum monoclonal protein that had resolved postoperatively. At 17 months of follow-up, the patient is still alive and doing well with no signs of recurrence or progression to mutliple myeloma. Although rare, solitary plasmacytoma of the ovary can occur without any overt symptoms or laboratory abnormalities tests and require prompt and adequate treatment and rigorous monitoring due to their ability to relapse or progress to MM. Complete surgical resection followed by activesurveillance is appropriate.
Solitary plasmacytoma is a rare malignant neoplasm of plasma cells accounting 5-10% of all plasma cell dyscrasias [1, 2]. The diagnosis of solitary plasmacytoma requires a single lesion composed of monoclonal plasma cells without evidence of systemic disease, such as bone marrow involvement, evidence of systemic amyloidosis, hypercalcemia, and organ damage (ie, renal insufficiency), or multiple sites of involvement on comprehensive imaging [2]. Solitary plasmacytoma of bone (SPB) and extramedullary plasmacytoma (EMP) belong to the broader diagnosis of solitary plasmacytomas, but have distinct characteristics at presentation [3, 4]. EMP comprises 3-5% of all plasma cell tumors [5]. They’re roughly one-third as common as SPB and about 80% present in the upper aerodigestive tract, with nasal cavity, paranasal sinuses, and nasopharynx being the most common sites of involvement [1, 6]. The 5-year risk of advancing to multiple myeloma (MM) is 30-50% for patients presenting with SPB but only 10-30% when found in the extramedullary soft tissue with a 10-year overall survival rate of 70% [7, 8]. EMP in the female genital tract are quite rare, either as solitary plasmacytomas or as part of a disseminated MM. There are few cases described in the literature [9- 12]. We report here a case of solitary ovarian plasmocytoma.
A 52-year-old multiparous woman and mother of 3 children, with past medical history of type 2 diabetes under oral treatment for 7 years, and spontaneous menopause at 49 years without hormonal therapy, presented recurring episodes of metrorrhagia for 3 years. Physical examination showed stable patient with no sign of hemodynamic instability. On vaginal and rectal examination, the uterus and cervix felt normal. A filling of bilateral vaginal sac was identified. There was tenderness during examination. Bilateral parametria were supple and rectal mucosa was free. Pelvic ultrasound revealed enlarged uterus with a heterogeneous thickning of endometrium and a heterogeneous left latero-uterine mass. Biological exams showed, Hb level at 14 g/dl, with normal blood cell count. Serum cancer antigen (CA-125) < 4 U/ml and lactic dehydrogenase (LDH) was high at 489 U/l. Beta human chorionic gonadotrophin (β-hcg), carcinoembryonic antigen (CEA), and alpha fetoprotein levels (AFP) were normal. Serum anti-HIV, and anti-HbSAg levels were also normal. Before surgery, diagnosis of ovarian granulosa tumor was suspected. The exploratory laparotomy revealed an enlarged and dilated left ovary measuring 4.5*3.5*3.0 cm and joined by the uterine cervix (Figure. 1).

Endometrium was polypoid with hemorrhagic stigma and an interstitiel myoma measuring 0.1*0.8 cm in favor of uterine leiomyoma. Histological study of left ovary showed a well circumscribed, encapsulated and white tumor measuring 4.0*3.2 cm. Pathological examination revealed tumor proliferation with insular and trabecular architecture with monotonous mature plasma cells with minimal cytonuclear atypia effacing the ovary (Figure. 2).

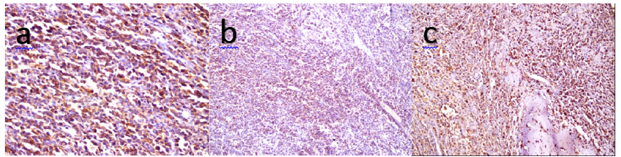
Immunohistochemical staining performed on the ovarian specimen showed positive expression of epithelial membrane antigen (EMA) (Fig. 3a), CD138 (Fig. 3b), with a lambda light chain restriction (Fig. 3c). Tumor cells were negative to cytokeratin, anti-smooth muscle, inhibine and H-Caldesmone. Antigen Ki-67 level was at 10%. Postoperatively, the patient underwent a full work-up to rule out MM, serum protein electrophoresis revealed a small monoclonal protein of 0.4 g/dl present in the gamma region. Urine immunoprotein tests were negative. Kidney function tests and calcemia were normal. Beta-2 microglobulin level was at 3.11 mg/l. Bone marrow examinations revealed 3% of plasma cells. X- ray examinations of the skeleton were normal. The diagnosis of solitary ovarian plasmocytoma was retained and the patient didn’t receive adjuvant treatment because surgical resection was complete. The patient is alive and doing well but the clinical and biological monitoring is irregular given the COVID pandemic and lack of access to specialized care establishment for tests and consultation. The current follow-up is 17 months.
EMP is a rare entity that comprise 3-5% of all plasma cells neoplasms [5] and result from the proliferation of monoclonal plasma cells with < 10% in bone marrow examinations with no evidence of systemic disease and with normal skeletal survey [2], aside from possibly monoclonal gammopathy [6]. EMP are present in 80% in head and neck [1,6], and typically affects the middle-aged persons (median 55- 60 years) with a predominance of female sex. Risk factors for EMP remain unknown; however, prior radiation exposure has been suggested. These patients have a higher rate of progression to MM, and they require close monitoring after appropriate treatment [13]. EMP in the female genital tract are extremely rare, there are few cases described [9- 12] and solitary ovarian plasmocytoma remains exceptional, Voegt et al. reported the first case in 1938 [14], and since then rare cases have been published as single observation or small series [12]. These tumors are usually large at the time of presentation and their size is greater than 12 cm with abdominal pain and/or mass [11]. Our patient presented dilated ovary mesearing 45*35*30 mm with small tumor measuring 40*32 mm, and without symptoms clinically. Metrorrhagia could be explained by the leiomyoma rather than the ovarian mass. Preoperatively, ovarian granulosa tumor was suspected in our patient because of the frequency, age, postmenopause and localization, therefore macroscopic examination and immunohistochemical staining remain essential to confirm or exclude diagnosis. Ovarian plasmocytomas are more likely involving the left ovary and usually without evidence of disseminated disease [11, 12]. In this case, the patient presented left ovarian plasmocytoma with positive CD138, and lambda light chain restriction. The work up to rule out MM showed solitary plasmocytoma with a small monoclonal protein at 0.4 g/dl. Adjuvant radiotherapy is suggested where full resection of the lesion is impossible or cannot be confirmed [6]. Our patient didn’t receive adjuvant radiotherapy due to the complete surgical resection. For solitary EMP, active surveillance after complete surgical resection is recommended. The rate of progression and survival data are very sparse and are collected from case reports. Median survival of patients with EMP is 4- 10 years. Local recurrence and progression to MM may occur, justifying prolonged and rigorous follow up [11, 15]. At follow-up, only 9% of patients progress with resolved serum monoclonal protein versus 71% of progression for patients with persistent serum monoclonal protein after treatment [16]. Our patient had normalized serum monoclonal protein after surgery and she’s doing well after 17 months of follow up.
Although rare, solitary plasmacytoma of the ovary can occur without any overt symptoms or laboratory abnormalities tests. These represent an entity of plasma cell dyscrasias and thus require prompt and adequate treatment and rigorous monitoring due to their ability to relapse or progress to MM. Complete surgical resection followed by active surveillance is appropriate. Due to the disparity in management and prognosis, it is important to distinguish solitary ovarian plasmocytoma from ovarian involvement in the context of MM.
Declaration of Competing Interest
None
Author contributions
SF conceived and designed the manuscript. SF wrote the manuscript. SF and KS reviewed and edited the manuscript and provided patient management. AM and AT contributed to patient management and review of the manuscript. All authors read and approved the final manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Patient Consent
Written, informed consent for publication of this report has been obtained from the patient. All identifying information has been removed to preserve confidentiality. We would like to thank the patient and his family for their contribution to this article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
