
Research Article | DOI: https://doi.org/10.31579/2690-1919/323
Professor (Retired) of Statistics, Jahangirnagar University, Dhaka
*Corresponding Author: K.C.Bhuiyan, Professor (Retired) of Statistics, Jahangirnagar University, Dhaka.
Citation: K.C.Bhuiyan (2023), Socioeconomic Variables Enhancing Prevalence of Diabetes Disability in Bangladeshi Adults of High Normal and Hypertensive Blood Pressure, J Clinical Research and Reports, 13(5); DOI:10.31579/2690-1919/323
Copyright: © 2023, K.C.Bhuiyan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 May 2023 | Accepted: 06 June 2023 | Published: 19 June 2023
Keywords: diabetes; hypertensive blood pressure; risk ratio
The present analysis was based on data collected from rural and urban Bangladeshi 995 adults of 18 years and above. The investigation was done to observe the prevalence of diabetes-disability in respondents of high normal and hypertensive blood pressure. Prevalence was noted in 9 such adults; among them 7 were males and 2 were females. The sample contained males and females in the ratio 50.1: 49.9. The respondents were interviewed during their visit in some diagnostic centres of urban and semi-urban areas. The sample diabetic adults were 67%. Among them who were suffering for 10 – 15 years the percentage of diabetic disable adults of higher blood pressure were 5.1%. For this group the risk of prevalence was 11.31 times. Higher risk was also noted among elderly adults and adults of high economic status. The most responsible variable which enhanced diabetes disability was duration of diabetes. The other enhancing variables were age, body mass index, and sedentary activity. These were identified on the basis of significant correlation coefficient of the variables and discriminant function score. However, rural people, males, illiterate people, housewives, adults of high economic status, had higher risk of prevalence. These were identified from the values of risk ratios. Beside these, the other responsible variables for enhancing the prevalence of the disease were habit of taking process food, and physical inactivity.
Many physically disable persons cannot perform their daily routine work, even they cannot walk and maintain their physical balance without any support. The problem increases among obese and diabetic patients when these two are beyond control or are untreated. In the long run the complications in mobility conditions, in hearing capacity and in visual impairment, including cardiovascular disease (CVD) and peripheral neuropathy arises among diabetic patients [1, 2, 3, 4]. Again, diabetes is a prime risk factor for cardiovascular diseases as diabetes and CVD are the two of the four groups of non-communicable diseases [5]. Diabetic patients suffering for longer duration without control of high blood glucose may face the heart problem as high blood glucose can damage the blood vessels and the nerves that control heart. Thus, reduction of CVD risk in diabetic patients is very important and it can be done by treating dyslipidaemia and hypertension [6]. In that sense hypertension, high normal blood pressure, diabetes and disability are interrelated non-communicable diseases.
Due to upward social mobility the rates of incidence of obese and diabetic patients are increasing day by day, specially the rate of type II diabetic patients in elderly people [7] and in course of time the rate of disable adults will be increased. It was reported that the adults in home and abroad are in risk of diabetes [8 – 16]. The disability among elderly diabetic patients is expected to be increased by 2025 in developed countries since older people will comprise two-thirds of the diabetic patients in those countries [ 17,18 ]. In one paper it was reported that the risk of disability might be increased 67% due to diabetes [19]. Researches indicated that neuropathy is a common physical disorder among elderly diabetic patients [1, 19]. In one research it was found that 90% diabetic patients of Bangladesh were disable [10]. The rate of prevalence of diabetes-disability was 4.3% in 2006 in India compared to 1 to 2 per cent in western world [20]. Disability increases the chance of sleep apnoea, lower limb amputation, morbidity and it creates a great economic burden [20 - 27]. This health hazard is predominant among females, elderly people and diabetic patients of longer duration [ 28, 29]. As more disable persons are observed among diabetic patients and, some influencing factors of diabetes viz. old age, female, illiteracy, physical inactivity, lifestyle, sedentary activity, food habit, family history etc. may be the causes of disability [21, 30 – 34]. Again, diabetes and hypertension are two associated non-communicable diseases. This was reported in separate studies [35 – 39].
Hence it was decided to observe the influence of the socioeconomic variables for simultaneous prevalence of diabetes disability in Bangladeshi adults of high normal and hypertensive blood pressure.
The study was done using the data collected from 995 adults of 18 years and above. These adults were interviewed by some nurses and medical assistants working in some purposively pre-selected diagnostic centres of urban and semi-urban areas of Bangladesh. The male and female units were interviewed to maintain the national sex ratio of 50.1: 49.9 in the population of Bangladesh during investigation in the session 2018 – 2019 [40] . The investigated males and females were 498 and 497, respectively. These respondents were interviewed when they were visiting the diagnostic centres; as a result we had information from adults mostly suffering from diabetes (67%).
The data of different socioeconomic variables were recorded from each selected respondent using a pre-designed and pre-tested questionnaire. The questionnaire contained different questions related to socio-demographic characteristics of the respondents. The information of life-style, and the information of suffering from any of the non-communicable diseases including period of suffering, the stages of treatment and the information of cost of treatment were also noted. The variables under investigation were mostly qualitative and a few were quantitative, but the values of all the variables were recorded in nominal scale so that data analysis would be easy. The value of body mass index (BMI) of each respondent was found out from the result of his/her weight ( in kg ) divided by height ( in metre2) . The adults were classified in to 4 classes on the basis of value of BMI. Obese adults were identified if BMI ≥ 27.5. The other 3 groups were underweight group, if BMI< 18> 140/90 ) [43, 44]. The respondents were also classified into 4 classes on the basis of their monthly family income and family expenditure. These classes were (i) lower ( if income < 50>
To fulfil the objective of the study, association of each of the socioeconomic variable with simultaneous prevalence of diabetes disability in Bangladeshi adults of high normal and hypertensive blood pressure was studied. Significant association was decided using the value of Chi-square and its p-value. A variable was considered as significantly associated if p-value of any ≤ 0.05. The risk ratio and its confidence interval was calculated for a group of adults for whom rate of prevalence of the diseases was noted higher for a level of the socioeconomic variable. Finally, the diabetic- disable group of adults of high normal and hypertensive blood pressure was discriminated from other adults by performing discriminant analysis. The analysis helped in identifying the socioeconomic variable(s) responsible for discrimination. The most responsible variable was one for which the absolute value of correlation coefficient of the variable and discriminant function score was highest [45, 46, 47, 48, 49]. For analysis SPSS Version 25 was utilized.
There were 9 patients who were suffering simultaneously from either high normal or hypertensive blood pressure and diabetes disability. The respondent was found out from the result of his/her weight ( in kg ) divided by height ( in metre2) . The adults were classified in to 4 classes on the basis of value of BMI. Obese adults were identified if BMI ≥ 27.5. The other 3 groups were underweight group,if BMI< 18>
remaining 986 respondents were free of simultaneous prevalence of these health problems. Total respondents were classified by the prevalence of high normal and hypertensive blood pressure and prevalence of diabetes-disability. The classified results were presented in Table 1.
| Prevalence of high normal and hypertensive blood pressure [B.P.≥ 130/85] | Prevalence of diabetes-disability | Total
| |
| Yes | No | ||
Yes Number % | 9 5.1 | 166 94.9 | 175 17.6 |
No Number % | 34 4.1 | 786 95.9 | 820 82.4 |
Total Number % | 43 4.3 | 952 95.7 | 995 100.0 |
Table 1: Adults classified by prevalence of Diabetes-disability and high normal and hypertensive blood pressure
In the sample there were 17.6
The results presented above indicated that variables age, economic status, involvement in sedentary activity, body mass index and duration of diabetes were significantly associated with the prevalence of diabetes disability in adults of high normal and hypertensive blood pressure. But none of the above socioeconomic variables was identified as most responsible for this prevalence. Discriminant analysis was done to identify the responsible variables for prevalence of diabetes-disability in adults of higher blood pressure. For the analysis the variables included were residence, religion, gender, age, marital status, education, occupation, economic status, smoking habit, habit of taking process food, habit of doing physical work.
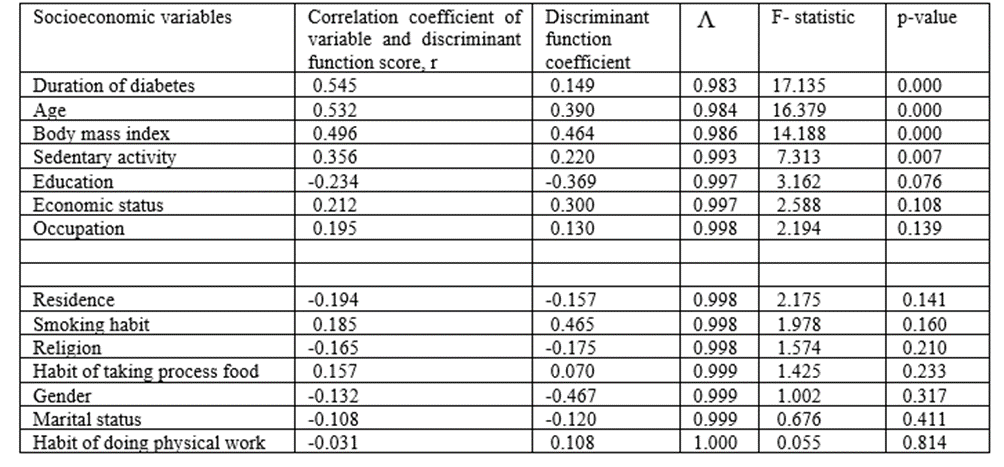
Table 3: Results found in discriminating diabetic-disable patients of higher blood pressure from other adults
body mass index, involvement in sedentary activity, and duration of diabetes. The influence of some of these variables were significantly different for two groups of adults. These variables were significantly sufficient in discriminating the patients of diabetes- disability along with higher blood pressure from other adults as was observed from the results = 0.945,=55.772 and p –value=0.000. The analytical results of the discrimination were presented in Table 3. It was seen that duration of diabetes was the most responsible variable to discriminate two groups of adults as the correlation coefficient (0.545) of this variable with discriminant function score was highest. The second, third and fourth most responsible variables were age, body mass index and involvement in sedentary activity, respectively. Though not significant, level of education also enhanced the prevalence of the diseases in patients.
Overweight, obesity, diabetes, hypertension are interrelated non-communicable diseases and are responsible for other non-communicable diseases [ 11, 17, 19, 20, 42, 48, 51, 52 – 55]. Diabetes and its related non-communicable diseases were well documented in home and abroad [ 35 – 38, 55, 56]. Suffering from diabetes for longer duration creates many types of complications in health, specially physical disability. It was reported in some earlier studies [4, 5, 6, 8, 11]. When simultaneous prevalence of diabetes and disability is observed in a person, he/she is identified as diabetic disable patient. This type of incidence is found among elderly adults in both developed and developing countries [7, 9, 57]. Strong association between diabetes and physical disability was reported in earlier studies [ 1, 36, 37]. Beside diabetes, some other clinical and socioeconomic variables were found associated with disability [19, 32, 42, 51, 52]. This paper was to identify some responsible socioeconomic variables for the prevalence of diabetes disability in 995 Bangladeshi adults of high normal and hypertensive blood pressure residing in urban and rural areas. The adults were of ages 18 years and above. Data were collected from these adults when they were visiting some diagnostic centres located in some urban and semi-urban localities. Among the adults 498 were males and 497 were females. The number of diabetic disable persons having higher blood pressure was 9( 0.9%). The remaining 986 (99.1%) adults were not suffering simultaneously from high normal and hypertensive blood pressure along with
diabetes-disability. The main objective of the work was to discriminate these two groups of adults and to identify the socioeconomic variables responsible for the discrimination.
In the sample there were 53.4% rural adults, 85.2% Muslim adults, 49.9
In this paper attempt was made to identify some socioeconomic variables which enhanced the prevalence of diabetes disability in adults of high normal and hypertensive blood pressure. For this, 995 adults of ages 18 years and above were interviewed when they visited some pre-selected diagnostic centres located in urban and semi-urban areas of Bangladesh. The sex ratio 50.1: 49.9 of the adults was maintained as this was the sex ratio at national level during investigation.
Among the respondents 9 (0.9%) were simultaneously suffering from higher blood pressure and diabetes-disability. The prevalence rate of these diseases in rural adults was 1.3%. The risk of prevalence in these rural adults was 206% more compared to the risk of urban adults. The risk was 2.00 times for males, 4.09 times for illiterate persons, 2.66 times for housewives. The prevalence rates in the above mentioned adults were 1.2%, 3.1%, 1.7% respectively. But residence, gender, education. and occupation were independent of prevalence of the diseases under consideration. All 9 affected patients were Muslims and all were married. But religion and marital status were not associated with the prevalence of the diseases. Similar independence of prevalence of the diseases with smoking habit, habit of taking process food and habit of doing physical work was noted. Significant association of prevalence of diabetes-disability in adults of higher blood pressure with age, economic status, sedentary activity, body mass index and duration of diabetes was observed. The prevalence rate in elderly people of ages 50 years and above was 3.1% and for them the risk of prevalence was 8.21 times. Prevalence rate in adults of higher economic status was 3.3%; the risk of prevalence for them was 5.57 times. The risk was 10.01 times for patients involved in sedentary activity. For this group the prevalence rate was 1.8%. All 9 patients were obese. Prevalence rate in diabetic patients suffering for 10 – 15 years was 5.1%. For them the risk of prevalence was 11.31 times.
It was observed that old age, obesity, sedentary activity and longer duration of diabetes were the highly risky factors for enhancing the prevalence of diabetes-disability in adults of high normal and hypertensive blood pressure. The variables related to these factors discriminated well the patients group from other adults. Out of these variables, duration of diabetes was the most responsible one followed by age, body mass index and sedentary activity for discrimination.
The risk of diabetes and its related diseases is increasing day by day. To get rid of the problem there should be cautious action at planning stage by the health planners. Rural and urban health workers can do a lot to encourage the people to try for leading a healthy life. This is needed for the welfare of the people and of the society . In that case the people can take some steps for leading a healthy life. These steps are :
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
