
Research Article | DOI: https://doi.org/10.31579/2642-9756/143
Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Miami Health Systems, Jackson Memorial Hospital, Miami, Florida.
*Corresponding Author: Chima Ndubizu, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Miami Health Systems, Jackson Memorial Hospital, Miami, Florida. Holtz Children’s Hospital, Suite 4070, 1611 NW 12th Avenue, Miami, FL 33136.
Citation: Chima Ndubizu, Cristina Colon, Johnny Galli, Cynthia Lebron., Madeline Cohen., et all (2023), Socioeconomic Status and SARS-CoV-2 Incidence Among Parturient Women: a Cohort Study., J. Women Health Care and Issues. 6(2); DOI:10.31579/2642-9756/143
Copyright: © 2023, Chima Ndubizu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 March 2023 | Accepted: 17 March 2023 | Published: 17 March 2023
Keywords: co-morbidities; covid-19; healthcare disparities; minority; obstetrics; pregnancy; socioeconomic factors
Objective: Coronavirus Disease 2019 (COVID-19), caused by the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2), is a public health emergency with high rates of morbidity and mortality in the general population. This study aims to evaluate the association between SARS-CoV-2 infection and socioeconomic factors, comorbidities, and obstetric outcomes among a diverse population of parturient women in South Florida.
Methods: Prospective cohort study conducted between April 30 and July 31, 2020 of parturient women admitted for delivery at a large urban hospital in Miami, Florida. Following consent, participants (n = 225) were screened for SARS-CoV-2 by nasopharyngeal polymerase chain reaction (PCR) upon admission for delivery. The relationship of SARS-CoV-2 with socioeconomic variables was examined, including insurance type, median income status, poverty level, and household density. Patients were categorized into high- versus low-income, defined as reported median income, mean household size and mean poverty rate, per American Community Survey and U.S Census Bureau (2014-2019 data used for this analysis). Variables were analyzed by Chi-square, Fisher’s exact test, t-test and ANOVA.
Results: Of n = 325 patients approached, 225 (68.9%) agreed to participate. Of those, 189 (83.93%) were PCR-negative and 36 (16.07%) were SARS-CoV-2 PCR-positive. SARS-CoV-2 positivity prevalence was higher among patients who identified as Hispanic (p=0.04), foreign-born (p=0.03), and had non-private medical insurance (p=0.02). No differences were found among socioeconomic variables (zip-code dependent median income, poverty rate, or average household size) and SARS-CoV-2 positivity. Additionally, no association was found between SARS-CoV-2 infectivity with comorbidities and obstetric outcomes.
Conclusions: Certain socioeconomic factors are associated with differential SARS-CoV-2 positivity rates among a heterogenous group of pregnant women in South Florida. These results provide insight into characteristics and risk factors in a Hispanic population possibly contributing to increased incidence of infection. These characteristics and risk factors may be useful targets in developing interventions for disease prevention.
Since the start of 2020, the Coronavirus Disease 2019 (COVID-19) pandemic has highlighted the degree of disparity in existing health conditions plaguing communities of color (Anderson-Carpenter and Neal 2021). Minority communities have higher prevalence of compromised immune systems and pre-existing medical conditions, such as cardiovascular disease, diabetes, asthma, which contribute to disproportionate SARS-CoV-2 infection and mortality rates (Anderson-Carpenter and Neal 2021). In the United States, rates of hospitalization, mechanical ventilation, and death due to COVID-19 have been significantly higher among people of color (Anderson-Carpenter and Neal 2021). Hispanic populations have the highest rates of SARS-CoV-2 infection among pregnant women (29.7%) (Anderson-Carpenter and Neal 2021; Zambrano, Ellington, Strid, Galang, Oduyebo, Tong, Woodworth, Nahabedian, Azziz-Baumgartner, Gilboa, Meaney-Delman, Akosa, et al. 2020).
The physiologic changes undergone during pregnancy cause increased susceptibility to respiratory pathogens (Tang, Wang, and Song 2018). Pregnant women with COVID-19 are more likely to be admitted to an intensive care unit, receive invasive ventilation, receive extracorporeal membrane oxygenation, and die (Zambrano, Ellington, Strid, Galang, Oduyebo, Tong, Woodworth, Nahabedian, Azziz-Baumgartner, Gilboa, Meaney-Delman, and Team 2020). Researchers have also found an association between COVID-19 and pregnancy complications, such as preeclampsia, preterm birth, and stillbirth (Wei et al. 2021). Further adverse pregnancy outcomes arise when comparing mild COVID-19 and severe COVID-19 (Wei et al. 2021), and the risk for racial/ethnic minority women is even higher.
Hispanic pregnant women experience a disproportionate risk for COVID-19 infection and death (Zambrano et al 2020). Non-Hispanic Black women, regardless of pregnancy status, experience a disproportionate number of deaths relative to their distribution among reported cases (Zambrano, Ellington, Strid, Galang, Oduyebo, Tong, Woodworth, Nahabedian, Azziz-Baumgartner, Gilboa, Meaney-Delman, and Team 2020). Since the development of vaccines to curb severity of COVID-19, preliminary findings from three safety monitoring systems did not find any safety concerns among pregnant women who received mRNA Covid-19 vaccines (Shimabukuro et al. 2021). Furthermore, data show that women who are vaccinated against COVID-19 during pregnancy are at lower risk for infection and severe illness (Goldshtein et al. 2021), and vaccination during pregnancy produces detectable antibodies against COVID-19 in infants (Gray et al. 2021).
The long standing history of marginalization of minority populations has likely exacerbated the negative impacts of the COVID-19 pandemic (Laurencin and Mcclinton 2020). It is well established that structural racism and health inequities have a profound impact on communities of color. Social determinants of health, such as education, access to health care, and socioeconomic status, also influence baseline health and, when lacking, perpetuate these disparities (Anderson-Carpenter and Neal 2021).
Understanding racial and ethnic inequalities requires cognizance of the disadvantages experienced by minority groups. Much effort has been put forth to understand and mitigate these obstacles; however, significant work remains to eliminate the disparities experienced. To date, the literature regarding minority groups and COVID-19 has primarily focused on infection, hospitalization and death rates, identification of clinical characteristics for risk stratification, and census-derived data analyses (e.g. poverty status) (Hsu et al. 2020; Wortham et al. 2021; Salacup et al. 2021; Ogedegbe et al. 2020; Suleyman et al. 2020). Most studies have been retrospective, observational investigations by design. However, limited information (Goldfarb et al. 2020; Reale et al. 2021; Barbosa-Leiker et al. 2021) exists exploring the impact of COVID-19 on these preexisting health disparities in a perinatal, minority population.
Jackson Memorial Hospital (JMH) is the main public safety net hospital in Miami Dade County and serves as a tertiary referral center for much of South Florida and the Caribbean islands. Miami-Dade County is the largest metropolitan area in the state of Florida, and is comprised of a diverse ethnic, racial, and socioeconomic population. As such, JMH offers a unique opportunity to assess disparity in SARS-CoV-2 infectivity among a predominantly diverse population.
The primary objective of this study aims to evaluate the SARS-CoV-2 infectivity in our pregnant population based on multiple socioeconomic variables. The secondary goals of the study will assess the associations of SARS-CoV-2 infectivity with comorbidities and obstetric outcomes. Through this investigation, we hope to expand the understanding of specific obstacles faced by perinatal women in communities of color in the hopes of identifying possibilities for intervention to decrease future spread of disease. We also discuss the possible underlying etiologies and social determinants of health that should be highlighted with the reporting of differential infection risk for these populations.
Our study was a prospective cohort study of pregnant women admitted for delivery at a large urban hospital in Miami, Florida. Patients were enrolled into the study between April 30 and July 31, 2020. Institutional review board approval from the University of Miami and Jackson Memorial Hospital was obtained for this study. All pregnant women were screened for SARS-CoV-2 using nasopharyngeal PCR per routine hospital protocol. All patients admitted for delivery at Jackson Memorial Hospital between the ages of 18-50 years of age were approached for study participation. Exclusion criteria were inmates and patients under the age of 18. Consent was obtained to collect maternal nasal swab, blood, urine, breast milk, fetal cord blood and cord segment, placental segment, vaginal swab, and amniotic fluid sample. Only the nasal swab results were used for data analysis as there was insufficient number of samples collected for the other specimens. Patient’s age, self-identified ethnicity and race, reported birthplace, and body mass index were obtained. Socioeconomic variables assessed included insurance type (private versus non-private versus other), median income status, poverty level and household density. Other insurance status encompassed patients who were uninsured, paid out of pocket, participated in the institutional financial assistance program, or received specialized grant support. Zip-code data was obtained from American Community Survey (ACS) and United States Census Bureau 2014-2019. These values were used to stratify high- versus low-income zip-codes. Patient zip-codes were divided into high- versus low-income areas using the median income, mean household size, and mean percentage in poverty as cut-off separating high- versus low-income using median reported income for the State of Florida.
The difference in SARS-CoV-2 infection status at delivery was assessed. Categorical and continuous variables were analyzed by Chi-square or Fisher’s exact test, and t-tests or ANOVA respectively. Statistical significance was set at P<0>
A total of 325 patients were approached to participate in the study; 225 (68.92%) were recruited and consented for the study. Of the 225 recruited patients, 189 (83.93%) were PCR-negative and 36 (16.07%) were PCR-positive for SARS-CoV-2. The population recruited was similar in age, race/ethnicity, body mass index, medical co-morbidities and marital status regardless of SARS-CoV-2 status (Table 1). More patients who tested positive for SARS-CoV-2 self-identified as Hispanic (86.11%), compared to those who tested negative (64.36%) (p= 0.04) (table 1). Foreign-born mothers also had higher proportion of SARS-CoV-2 positivity of 80.56% compared to US-born patients which represented 19.44% of the infected patients (p = 0.03) (Table 1).
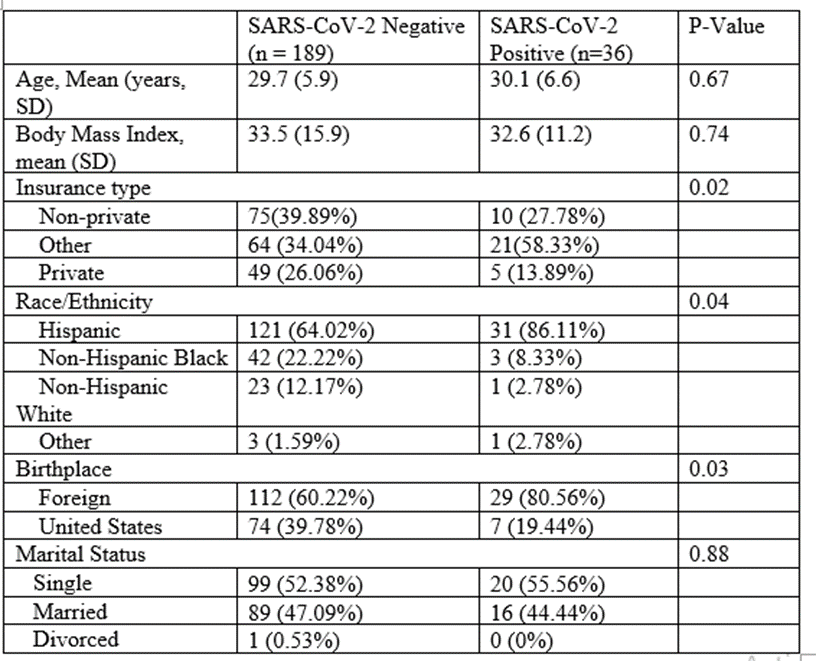
Table 1: Demographic details of study population and SARS-CoV-2 infection rates.
Higher rates of SARS-CoV-2 infection in patients were identified among non-private medical insurance (27.78%) compared to patients with private insurance (13.89%) or other insurance classification (58.33%) (p=0.02).
SARS-CoV-2 infection was not associated with increased comorbidities of pregnancy or different gestational outcomes as seen in Table 2. No differences were observed between the outcome variables (zip-code dependent median income, poverty rate or average household size) and SARS-CoV-2 positivity (Table3). Although not statistically significant, a greater proportion of those who tested positive for SARS-CoV-2 (77.78%), resided in low median income zip code areas compared to patients testing negative (73.26%) (p=0.72) (Table 3).
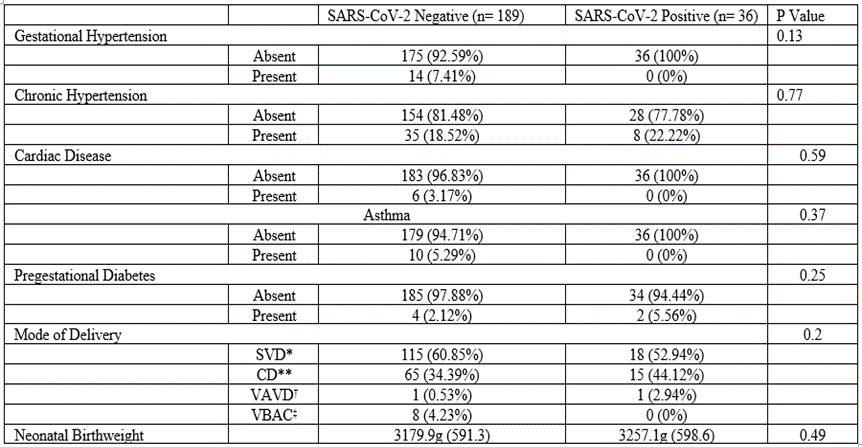
*SVD=spontaneous vaginal delivery, **CD=Cesarean Delivery, †VAVD=Vacuum Assisted Vaginal Delivery, ‡VBAC=Vaginal Birth After Cesarean.
Table 2: Presence of comorbid conditions and obstetrics outcomes versus SARS-CoV-2 infection rates.
Table 3: Socioeconomic data and SARS-CoV-2 infection. Median income reported overall for the state of Florida was $53,267 (12.7%) and an average household size of 2.65.
This study demonstrates differential SARS-CoV-2 positivity rates among a heterogenous group of pregnant women, predominantly Hispanic/Latin American, in South Florida. Study outcomes provide insight into the characteristics and risk factors in a Hispanic population that may contribute to increased incidence of infection. Additionally, results support the findings of similar studies performed in other large metropolitan areas (12).
The structural racism experienced by minority groups has subsequent downstream effects on their health outcomes. Additionally, the history of inequity is generational. Legislation, such as the Social Security Act of 1935, marginalized blue collar/agricultural workers and created unfair advantages for wealth acquisition and development (Bailey et al. 2017). The resulting uneven distribution of wealth in turn affects the choice of residential locations and their access to healthcare (Abraham et al. 2021). Poorer neighborhoods likely inhabited by minority groups, are more likely to have healthcare, educational, and commercial facilities with lower infrastructure (Bailey et al. 2017). Minority groups are more likely to lack health insurance either due to job type or poor job security, which impacts access to healthcare (Abraham et al. 2021). Historical events like the Tuskegee syphilis experiment, among others, further create a mistrust of the medical system by minority groups (Abraham et al. 2021).
Our results indicate a relationship between Hispanic ethnicity and SARS-CoV-2 positivity. This is consistent with previous studies of increased rates of SARS-CoV-2 infection in minority groups when comparing the overall racial/ethnic rate of infection (Laurencin and Mcclinton 2020). In particular for perinatal women, the case series by Grechukhina et al. noted higher SARS-CoV-2 positivity rates among pregnant patients of Hispanic ethnicity compared to non-Hispanic counterparts, OR = 5.5 (Grechukhina et al. 2020). Study results support the differential infection risk for minority groups, however, this finding in our sample population is not surprising considering the demographic make-up of the South Florida community. Our data which showed most of our SAR-CoV-2 positive cohort identifying as Hispanic (86.11%) and foreign-born (80.56%), corresponds to the latest census for Miami Dade County which reported 69.4% of individuals identifying as Hispanic and 53.7% reporting being foreign-born (United States Census Bureau. QuickFacts).
Additionally, slightly more than half the population responding to the local census identified as foreign-born (United States Census Bureau. QuickFacts). Interestingly, this study was able to examine the novel question of the relationship between birthplace and infection, which was explored beyond present housing situation/zip-code to better understand risk factors for infection. In this cohort, Hispanic and/or foreign-born women were approximately four times more likely to test positive compared to domestic born patients. This is a potential target demographic to consider when developing or realizing disease prevention interventions.
It has been previously established that most SARS-CoV-2 positive patients are more likely to have preexisting health conditions, such as obesity, hypertension, diabetes, asthma (Bhattacharyya et al. 2021). For minorities living in low-income areas frequently in multigenerational households, difficulty obtaining affordable, healthy food options, access to exercise facilities or outdoor parks due to poor neighborhood infrastructure contribute to higher rates of or worsening of co-morbidities (Abraham et al. 2021). Worsening COVID-19 has also been shown to be associated with poor gestational outcomes (Wei et al. 2021). In contrast with previous studies, this study did not find a relationship between infection and comorbidities or differences in gestational outcomes for delivery or neonatal birth weight. This result may be attributable to the small study population. Reale et al. have previously established that having multiple risk factors for SAR-CoV-2 infection may produce additive risk (Reale et al. 2021). One of the risk factors analyzed in their study was insurance status. They found pregnant women who were beneficiaries of public insurance had nearly a tenfold higher risk of infection compared to privately insured women (Reale et al. 2021). The current study supported this finding; the majority of women positive for SARS-CoV-2 infection were either non-privately insured or other (out of pocket or uninsured). This finding may be attributed to either unemployment status secondary to the pandemic or job types with inadequate or absent health insurance coverage.
A variety of factors may be attributable to the association between SARS-CoV-2 and minority group status. Minority groups are more likely to reside in crowded multigenerational households, which increases the risk of SARS-CoV-2 transmission due to inability to implement recommended social distancing (Abraham et al. 2021). Utilization of public transportation is more common in low-income earning and minority communities and in crowded cities with equally crowded transit systems, further contributing to SARS-CoV-2 spread within these groups (Abraham et al. 2021). However, in contrast with results from previous studies on higher exposure density in minority groups (Hong et al. 2021) and infection/hospitalization rates in high-poverty census tracts (Wortham et al. 2021), results from the current study did not support a differential rates of infection by zip-code dependent median income, poverty, rate or average household size.
Although not analyzed in our study, emergent measures taken to curtail viral spread may have had uneven impact on minority populations with disproportionate job and income losses as well as reduced access to care for non-COVID-19 related issues (Bambra et al. 2020). These minority groups are also less likely to have employment types that accommodate remote work and are more likely to have multiple employments in industries remaining open during non-essential closures (Abraham et al. 2021).
Many social determinants contribute to the increased rate of SARS-CoV-2 infection in our Hispanic patients. In addition to those contributors previously mentioned, financial constraints and language barriers can impact access to health care and adherence to public health recommendations with regards to social distancing (Boserup, Mckenney, and Elkbuli 2020). Though there has been denial in recognizing the role of both historical and current day racism in health inequalities, it is now acknowledged that minority groups in the United States are more likely to experience poor health outcomes (Bailey et al. 2017). In addition to the existing health disparities for minority groups, Barbosa-Leiker et al. also reported increased stressors developing during the COVID-19 pandemic among perinatal women in minority groups (Barbosa-Leiker et al. 2021). Additional obstacles for health, support, and safety worsened existing disparities in this vulnerable population. This is important in the consideration of developing effective intervention methods that can help to ameliorate the increased disparities during the pandemic.
Characterization of risk factors, understanding exposure patterns (Hong et al. 2021), knowledge, attitudes, and practices (Burger et al. 2021) are essential to assist in development of disease spread prevention. More work is still needed, however, to enhance continued understanding and mitigation of health disparities experienced by minority groups.
To the best of our knowledge, this study is the largest prospective single center series of SARS-CoV-2 positivity in the southeastern United States in a heterogenous group of predominantly Hispanic population. Although this study had a relatively small sample size, it was based on a diverse cohort of patients served in an institution encompassing both university and community health systems. As such, however, results may not be readily generalizable to other areas of the country with different ethnic and racial representation.
Our results echo studies from other parts of the country regarding the relationships between ethnic disparities, insurance status, and SARS-CoV-2 infectivity. In the current cohort, SARS-CoV-2 positivity rates were associated with ethnicity, insurance type and birthplace. However, SARS-CoV-2 infectivity rates did not differ by zip-code median income, poverty, or household size. Our study findings provide insights into characteristics and risk factors that may be useful in developing interventions for disease prevention. Future efforts investigating the etiologies for the disproportionate levels of infectivity are essential to facilitate disease prevention.
This study was funded by the University of Miami Office of the Vice Provost for Research as part of a Pilot Award for the study of COVID-19 in pregnancy to the Department of Obstetrics, Gynecology and Reproductive Sciences.
We would like to thank the University of Miami Office of the Vice Provost for Research for their financial support of this study. We would also like to thank the institution and staff of the University of Miami Health Systems and Jackson Memorial Hospital, which helped to make this study possible.
CN, JP, MJP, AKS contributed to the conception and design of the work. All authors contributed to the writing of the manuscript.
The authors declare that the research was conducted in absence of any commercial or financial relationships that could be construed as potential conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
