
Research Article | DOI: https://doi.org/10.31579/2578-8868/318
Department of Neurological Surgery, University of Wisconsin School of Medicine and Public Health, Madison, WI, USA.
*Corresponding Author: Ahmed Elbayomy, MD Department of Neurological Surgery, University of Wisconsin School of Medicine and Public Health, Madison, WI, USA.
Citation: Ahmed Elbayomy, Jason Kim, Simon Ammanuel, Momin Mohis, Ian Koszewski, et al, (2024), Socioeconomic Disparities in the Utilization of Endoscopic Transsphenoidal Pituitary Surgery: A Retrospective Analysis of the National Inpatient Sample, J. Neuroscience and Neurological Surgery, 16(4); DOI:10.31579/2578-8868/318
Copyright: ©, 2024, Ahmed Elbayomy. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 06 May 2024 | Accepted: 14 October 2024 | Published: 01 November 2024
Keywords: glioblastoma; adult diffuse glioma; heberferon
Introduction Pituitary neoplasms account for 15% of all intracranial neoplasms and affect 20% of the population.
Objective We aim to use the National Inpatient Sample (NIS) to ascertain disparities in utilization and outcomes among endoscopic endonasal pituitary surgery patients.
Methods NIS was used from 2010 to 2020. Pearson's v2, Fisher's Exact, and independent 2-tailed t-tests were used to assess patient characteristics and outcomes. A logistic regression model was used to compare in-hospital mortality and post-operative complications between Racial groups. Statistically significant postoperative complications were analyzed with a multivariable logistic regression to determine the independent impact of obesity on postoperative outcomes.
Results Hospitalization rates for this procedure declined significantly over the decade, from 10,279 in 2010 to 5,875 in 2020 (trend p value < 0.001). The majority of patients were between 25 and 64 years old (72.16%), with 60.73% having no comorbidities. While the gender distribution was nearly even, disparities emerged across racial and socioeconomic groups. Black and Hispanic patients were more likely to reside in lower income zip codes and depend on Medicaid compared to White patients. Black patients had higher odds of any postoperative complication (adjusted OR: 1.14, p=0.003) and specific complications like diabetes insipidus, fluid/electrolyte disorders, and renal/urinary issues compared to White patients. Both Black and Hispanic patients faced higher mortality risks post-surgery compared to White patients (adjusted OR: 2.62 and 2.44, respectively, p<0.05). Medicaid coverage was associated with higher odds of any complication (adjusted OR: 1.18, p=0.016), while private insurance was linked to lower odds (adjusted OR: 0.88, p=0.015).Patients in the lowest income quartile had higher odds of complications compared to those in higher quartiles. Obesity independently predicted increased odds of pulmonary, renal, and hemorrhagic complications.
Conclusion Despite advancements in endoscopic endonasal pituitary surgery, disparities in access and outcomes persist across racial, socioeconomic, and insurance groups. These findings underscore the need for targeted interventions to address these inequalities and ensure equitable access to quality care.
Pituitary neoplasms account for 15% of all intracranial neoplasms and impact approximately 20% of the global population [1]. The mechanism underlying development and growth of pituitary neoplasms remains largely elusive, though current hypotheses propose hormonal changes as a key driver [1, 2]. Additionally, it's posited that these hormonal responses could be influenced by stress levels, leading to speculation that socioeconomic factors might play a role in the disease's pathophysiology [1, 3]. Historically, symptomatic tumors, which are capable of inducing neurological deficits, have been managed through microscopic surgical interventions [4].
Over the past two decades, the advent of endoscopic pituitary surgery has marked a significant evolution in treatment practices [5]. Comparative studies have consistently shown the endoscopic endonasal technique to be safer and more effective than its microscopic counterpart [4, 5]. This technique's advantages, including superior visualization and shorter hospital stays, have contributed to its increasing adoption for treating pituitary tumors [4]. However, the literature has not fully quantified the impact of preoperative factors such as high BMI, limited surgeon experience, and female gender on the risk of complications, notably cerebrospinal fluid (CSF) leaks [5]. Additionally, studies have exposed stark disparities in access to neuro-oncological care related to socioeconomic status and race/ethnicity, highlighting the critical issue of inequality within the healthcare system [5, 6].
Despite the recognized importance of socioeconomic factors, there appears to be a lack of comprehensive analyses on how socioeconomic status (SES) influences the complications and outcomes of endoscopic pituitary surgery. Our study seeks to address this gap by leveraging data from the National Inpatient Sample (NIS) to explore variations in surgical utilization and patient outcomes based on procedure type (endoscopic endonasal or tranfrontal), SES, race, payer type, and obesity. and. We also evaluated the mortality and morbidity associated with these procedures based on medical and endocrine complications and 30day readmission for CSF leak.
Study Design and Patient Eligibility
A retrospective cross-sectional investigation was conducted utilizing the NIS from 2010 to 2020, which is part of the Healthcare Cost and Utilization Project (HCUP) from the Agency for Healthcare Research and Quality. Furthermore, the NIS is a hospital discharge database that represents 20% of all inpatient admissions to non-federal hospitals in the U.S. [7]. Prior to 2012, the NIS represented 100% of discharges from a 20% sample of all hospitals in the HCUP strata. However, beginning in 2012, the sampling procedure was modified to reflect a 20% sample of hospital discharges from all HCUP hospitals. Consequently, the database name was modified in 2012 to reflect these changes. Each discharge in the NIS database represents one hospitalization. In this regard, the NIS does not have unique patient data; therefore, one patient may represent multiple discharges. We also examined the national Readmission Database (NRD) for the same period, focusing on 30-day readnission specifically for CSF leaks.
In the present study, a discharge is referred to as a patient. All patients undergoing endoscopic transsphenoidal and transfrontal pituitary surgeries were identified using the International Classification of Diseases, the 9th Revision (ICD-9 CM) codes (07.62, 07.65, and 07.61, 07.64), and the 10th Revision (ICD-10 CM) codes (0GB04ZX,0GB04ZZ, and 0GB00ZZ, 0GT00ZZ) for diagnosis and procedure coding for endoscopic transsphenoidal and transfrontal approaches, respectively.
Data Collection and Outcomes
Patient-level data includes the patient's age, sex, race (White, Black, Hispanic, Asian or Pacific Islander, Native American, and others), median household income in the patient's zip code (1st quartile, 2nd quartile, 3rd quartile, and 4th quartile), primary expected payer (Medicare, Medicaid, private insurance, and uninsured), discharge status (routine, transfer to short-term hospital, transfer to another facility [including skilled nursing facility (SNF), intermediate care facility (ICF), another type of facility], home health care, against medical advice [AMA], died in hospital, discharged alive, discharged to court/law enforcement, destination unknown), length of stay, hospital bed size (small, medium, and large), teaching status, hospital region (Northeast, Midwest, South, and West), along with location (urban and rural), principal diagnosis, as well as secondary diagnosis using the ICD-9 and ICD-10 revisions. The comorbidity burden was assessed using Deyo's modification of Charlson's comorbidity index (CCI). Finally, in-hospital mortality is directly coded in the NIS database, and complications were examined in all secondary diagnosis fields using ICD-9 CM and ICD-10 CM codes.
The analyzed complications included CNS infection, CSF leak, diabetes insipidus (DI), iatrogenic pituitary disorder, fluid and electrolyte disorders, neurological disorders, pulmonary disorders, cardiac disorders, renal disorders, hemorrhage, and hematoma. All statistical calculations for this analysis were performed using STATA version 17. Additionally, patient characteristics and outcome variables were tested using Pearson's chi-square test, Fisher's exact test, and independent two-tailed t-tests, as appropriate. Variable differences between the groups were deemed to be statistically significant if the P-value was less than 0.05. Moreover, a logistic regression model for comparison of in-hospital mortality and postoperative complications between racial groups included race, age, sex, and CCI as independent variables. Furthermore, statistically significant postoperative complications were analyzed with a multivariable logistic regression (which accounts for age, gender, race, and statistically significant demographic differences) to determine the independent impact of obesity on postoperative outcomes.
Over the span of a decade from 2010 to 2020, a total of 82,249 patients who underwent endoscopic transsphenoidal pituitary surgery were identified. The hospitalization rates for endoscopic transsphenoidal pituitary surgeries in the United States displayed a notable decline. The rates started at 10,279 hospitalizations in 2010, peaked slightly in 2011 with 10,798 cases, and then followed a downward trajectory to 5,875 by 2020. This trend of decreasing hospitalization rates was statistically significant, with a trend p-value of less than 0.001. (Table1, fig 1).
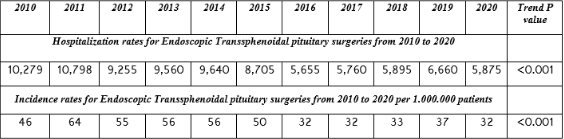
Table 1
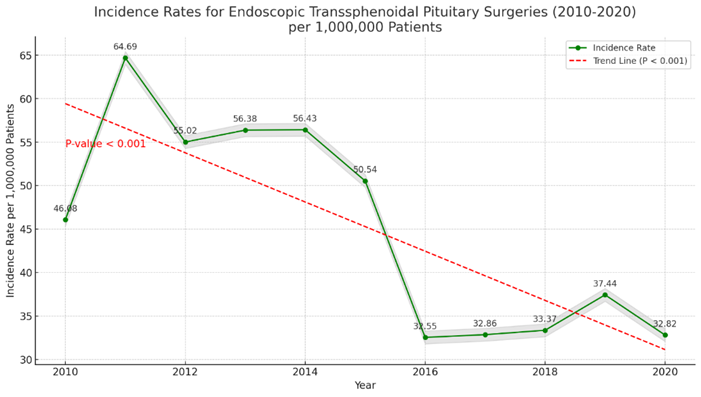
Figure 1: Incidence rates for endoscopic transsphenoidal pituitary surgeries from 2010 to 2020 per 1.000.000 patients. This figure was created with M.S. Excel version X.
The incidence rates of endoscopic transsphenoidal pituitary surgery in the U.S. were calculated using the annual estimates of the U.S. resident population on July 1st as the denominator. In parallel, the incidence rates of these surgeries per 1,000,000 patients also saw a decline over the same period. The incidence rate was at its highest in 2011, with 64 cases per million, before gradually decreasing to 32 cases per million by 2020, mirroring the trend observed in hospitalization rates. This reduction in both hospitalization and incidence rates underscores a significant shift in the management of pituitary disorders, potentially indicating improvements in non-surgical interventions, changes in clinical guidelines, or access to care, and is also statistically significant with a trend p-value of less than 0.001. (Table 1, Figure 2).
In this study, patient age distribution was as follows: 22,597 (27.47%) were between 25 to 44 years, 36,758 (44.69%) were aged 45 to 64 years, 22,072 (26.83%) were in the 65 to 84 years age group, and 823 (1.00%) were 80 years or older, with this age distribution being statistically significant (P<0>Among the study population, the vast majority (89.61%, n=73,687) were routinely discharged to their homes. A smaller proportion were
transferred to short-term hospitals (0.35%, n=290), skilled nursing or intermediate care facilities (3.75%, n=3091), or received home health care (5.74%, n=4725). A negligible number were discharged against medical advice (0.09%, n=75), while a few patients either died or had an unknown discharge status (0.04%, n=352), indicating significant differences in discharge outcomes (P<0 n=40,675) n=41,436) n=4845) n=11377) n=65675), n=74209), n=7697)>Geographically, hospital patient counts were as follows: Northeast (18.70%, n=15,387), Midwest (19.91%, n=16,380), South (36.61%, n=30,114), and West (24.76%, n=20,368), exhibiting a mean hospital stay of 4.43 days, which was statistically significant (P<0 n=44,443), n=22,971), n=8,053), n=2,895), n=3,292), n=434) n=21,446), n=20,564), n=19,566), n=18,844)>
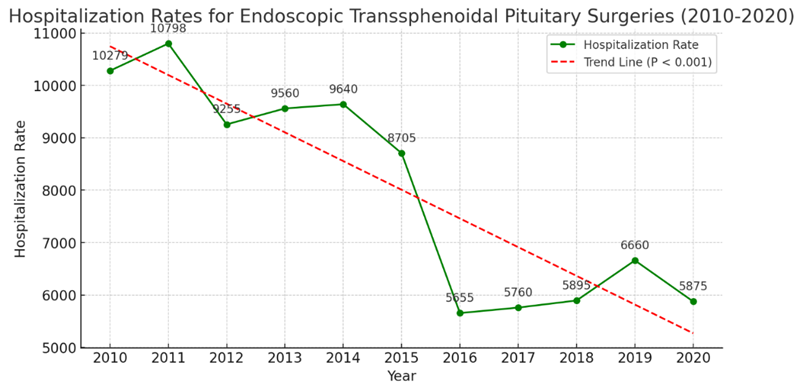
Figure 2: Hospitalization rates for endoscopic transsphenoidal pituitary surgeries from 2010 to 2020. This figure was created with M.S. Excel version X.
Racial Disparities
This study identified 74,547 patients—White (48,356), Black (15,133), and Hispanic (11,058)—undergoing endoscopic transsphenoidal pituitary surgery. The analysis revealed Hispanic patients as the youngest group with a mean age of 48.04 years, closely followed by Black (53.08 years) and White patients (53.13 years), showing significant age differences (P<0>
| Variable | White (N= 48356), % | Black (N= 15133), % | Hispanic (N= 11058), % | P-value |
| Age (mean ± S.D.) | 53.13 ± 19.60 | 53.08 ±29.35 | 48.04 ±35.91 | <0> |
| 25 to 44 | 25.40% | 25.34% | 35.84% | |
| 45 to 64 | 43.54% | 48.20% | 44.81% | |
| 65 to 84 | 29.85% | 25.95% | 18.71% | |
| 85 and older | 1.21% | 0.51% | 0.64% | |
| CCI | <0> | |||
| Zero | 63.72% | 53.26% | 62.93% | |
| One | 21.50% | 26.51% | 24.37% | |
| Two | 7.91% | 9.91% | 6.71% | |
| Three and higher | 6.87% | 10.32% | 5.99% | |
| Sex | <0> | |||
| Male | 49.83% | 47.73% | 45.88% | |
| Bed Size | 0.818 | |||
| Small | 5.27% | 5.92% | 4.95% | |
| Medium | 14.37% | 14.44% | 15.14% | |
| Large | 80.36% | 79.63% | 79.91% | |
| Hospital Region | <0> | |||
| Northeast | 20.29% | 18.11% | 12.93% | |
| Midwest | 20.91% | 16.41% | 7.94% | |
| South | 35.81% | 54.82% | 37.10% | |
| West | 22.99% | 10.65% | 42.03% | |
| LOS | 4.05 ± 6.96 | 5.38 ± 14.26 | 5.10 ± 17.79 | |
| Payer | <0> | |||
| Medicare | 29.03% | 28.32% | 17.49% | |
| Medicaid | 6.71% | 14.98% | 20.91% | |
| Private | 58.71% | 45.80% | 46.58% | |
| Self-pay | 2.05% | 4.30% | 8.00% | |
| No charge | 0.19% | 0.71% | 1.79% | |
| Others | 3.31% | 5.89% | 5.22% | |
| Disposition | <0> | |||
| Routine | 90.95% | 85.39% | 91.29% | |
| Short term hosp | 0.25% | 0.50% | 0.37% | |
| SNF, ICF, Another | 3.49% | 5.15% | 2.50% | |
| HHC | 5.03% | 8.06% | 5.31% | |
| Others | 0.28% | 0.90% | 0.53% | |
| Teaching Status | <0> | |||
| Non-teaching | 10.02% | 8.00% | 11.58% | |
| Teaching | 89.98% | 92.00% | 88.42% | |
| Median Income | <0> | |||
| 1st quartile | 19.33% | 40.35% | 32.07% | |
| 2nd quartile | 24.18% | 23.34% | 22.92% | |
| 3rd quartile | 27.06% | 20.10% | 26.69% | |
| 4th quartile | 29.43% | 16.22% | 18.32% | |
Table 2: Patients' demographics and Hospital characteristics by Racial and Ethnic Group
Abbreviations: LOS, Length of stay; Short term hosp; Short-term hospital; SNF, Skilled Nursing Facility ; ICF, Intermediate Care Facility;Another, Another type of facility;HCC, Home Health Care.
Analysis of Complications by Race
Table 3 summarizes the in-hospital mortality and complication rates among racial groups, with Table 4 detailing the odds of complications for Black and Hispanic patients relative to White patients. Black patients had significantly higher odds of experiencing any postoperative complication (unadjusted OR [uOR]: 1.19 [1.09-1.30], P<0 P=0.003) P=0.03), P=0.004) P=0.02),>
| Complications | White, % | Black, % | Hispanic, % | P-value |
| Died | 0.22% | 0.70% | 0.49% | <0> |
| Any Complication | 35.98% | 40.11% | 38.34% | <0> |
| CSF leak | 7.53% | 8.38% | 9.39% | 0.013 |
| CNS Infection | 0.88% | 0.75% | 0.97% | 0.69 |
| Diabetes Insipidus | 14.89% | 16.62% | 16.88% | 0.014% |
| Iatrogenic Pituitary Disorder | 1.07% | 1.03% | 0.85% | 0.66% |
| Fluid and Electrolyte Disorders | 14.23% | 17.55% | 14.50% | <0> |
| Neurological Diseases | 6.91% | 7.07% | 7.36% | 0.77% |
| Pulmonary Diseases | 1.80% | 2.16% | 1.81% | 0.42% |
| Cardiac Diseases | 0.66% | 0.59% | 0.41% | 0.40% |
| Renal Diseases | 1.60% | 4.08% | 1.71% | <0> |
| Hemorrhage | 0.89% | 1.29% | 1.14% | 0.15% |
Table 3: Complication and Mortality Rate by Racial and Ethnic Groups
| Complications | Black | Hispanic | ||||||
| uOR (95% CI) | P-value | aOR (95% CI) | P-value | OR (95% CI) | P-value | aOR (95% CI) | P-value | |
| Died | 3.20(1.69-6.03) | <0> | 2.62(1.36-5.06) | 0.004 | 2.24(1.06-4.71) | 0.032 | 2.44(1.11-5.33) | 0.025 |
| Any Complication | 1.19(1.09-1.30) | <0> | 1.14(1.04-1.24) | 0.003 | 1.10(1.00-1.22) | 0.045 | 1.07(0.97-1.18) | 0.14 |
| CSF leak | 1.12(0.96-1.31) | 0.13 | 1.08(0.91-1.27) | 0.34 | 1.27(1.05-1.53) | 0.010 | 1.24(1.01-1.51) | 0.034 |
| CNS Infection | 0.85(0.54-1.34) | 0.49 | 0.75(0.47-1.19) | 0.23 | 1.09(0.68-1.76) | 0.70 | 1.10(0.68-1.77) | 0.68 |
| Diabetes Insipidus | 1.13(1.02-1.27) | 0.02 | 1.15(1.02-1.28) | 0.016 | 1.16(1.01-1.32) | 0.02 | 1.00(0.88-1.15) | 0.91 |
| Iatrogenic Pituitary Disorder | 0.96(0.64-1.43) | 0.86 | 0.93(0.62-1.40) | 0.76 | 0.79(0.48-1.31) | 0.37 | 0.77(0.46-1.29) | 0.33 |
| Fluid and Electrolyte Disorders | 1.28(1.14-1.44) | <0> | 1.21(1.08-1.36) | <0> | 1.02(0.89-1.17) | 0.75 | 1.10(0.95-1.26) | 0.16 |
| Neurological Diseases | 1.02(0.87-1.20) | 0.76 | 0.99(0.84-1.17) | 0.97 | 1.07(0.87-1.30) | 0.50 | 1.05(0.86-1.28) | 0.61 |
| Pulmonary Diseases | 1.20(0.90-1.60) | 0.20 | 1.07(0.80-1.43) | 0.63 | 1.00(0.71-1.41) | 0.97 | 1.09(0.77-1.53) | 0.60 |
| Cardiac Diseases | 0.90(0.53-1.53) | 0.71 | 0.81(0.48-1.38) | 0.45 | 0.62(0.31-1.24) | 0.18 | 0.75(0.37-1.49) | 0.41 |
| Renal Diseases | 2.61(2.05-3.32) | <0> | 2.35(1.83-3.02) | <0> | 1.07(0.73-1.56) | 0.71 | 1.31(0.90-1.93) | 0.15 |
| Hemorrhage | 1.46(0.99-2.14) | 0.053 | 1.42(0.96-2.10) | 0.073 | 1.28(0.77-2.15) | 0.32 | 1.46(0.87-2.46) | 0.14 |
Table 4: In-hospital mortality and postoperative complications in Black and Hispanic patients compared to White patients.
Analysis of Complications by Insurance Status
Table 5 delineates the odds of postoperative complications across different insurance types relative to Medicare. Patients with Medicaid exhibited higher odds of any complication (uOR: 1.31 [1.17-1.46], P<0 P=0.016), P=0.008; P=0.015). P=0.007) P=0.03), P=0.008).>
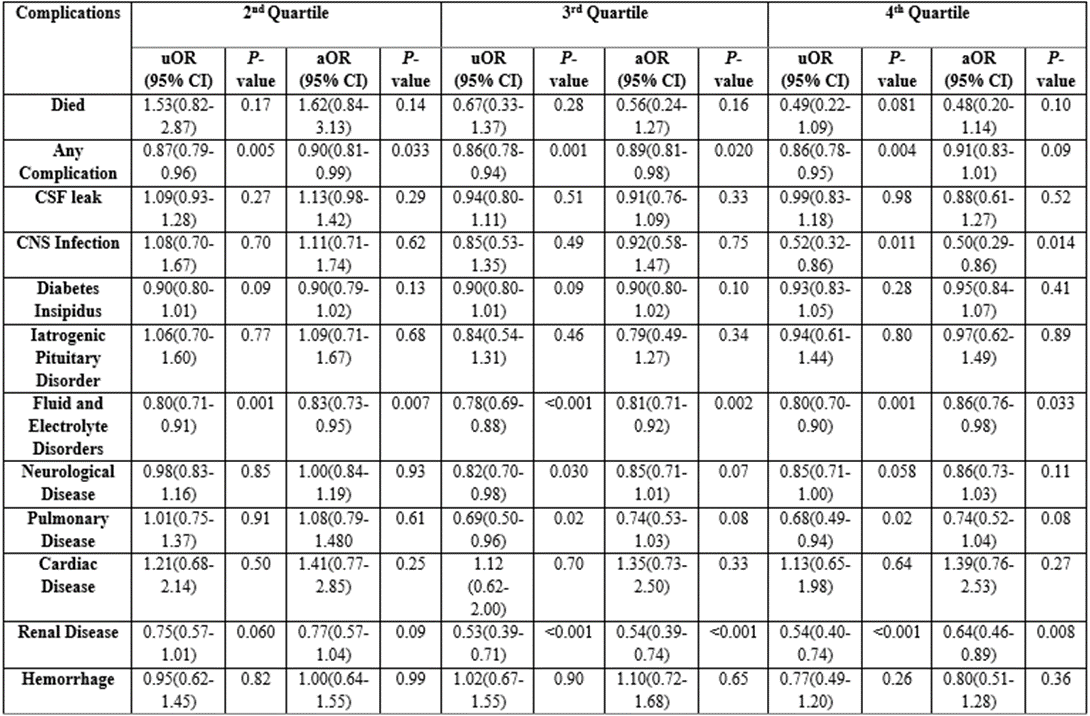
Table 6: In-hospital mortality and postoperative complications by hospital volume quartiles compared to the lowest quartile.
Analysis of CSF Leak After Endoscopic Transsphenoidal Pituitary Surgery and Transfrontal Pituitary surgery
Our data revealed a significant difference in the proportions of patients experiencing CSF leaks with endoscopic transsphenoidal and transfrontal pituitary surgeries. CSF leaks were reported in 8.0% of patients undergoing the endoscopic approach compared to 10.3% in the transfrontal group (p < 0>To further investigate the accuracy of CSF leak reporting, we examined the NRD for the same period, focusing on 30-day readmissions specifically for CSF leaks. This analysis revealed 529 readmission cases (10.11%) following endoscopic transsphenoidal surgery and 152 cases (10.79%) after transfrontal surgery. Readmission rates based on sex were similar across both surgical approaches, with no statistically significant
differences observed (p = 0.58 and 0.67 for endoscopic and transfrontal groups, respectively).
Interestingly, a linear trend analysis of CSF leak readmissions showed an increase over time for the endoscopic group, with a statistically significant odds ratio of 1.07 (p = 0.002). This trend was not observed in the transfrontal group, where the odds ratio was 1.05 with a non-significant p-value (1.65).
Analysis of Obesity on Mortality and Postoperative Complications for Endoscopic Transsphenoidal Pituitary Surgery
Univariate regression analysis revealed significantly lower odds of hemorrhagic complications (OR: 0.65, P=0.015), alongside higher odds for developing overall complications (OR: 1.17, P≤0.001), CNS infection (OR: 1.56, P=0.014), DI (OR: 1.48, P=0.017), and complications related to fluids and electrolytes (OR: 1.11, P=0.046), pulmonary (OR: 1.53, P<0 P=0.015). P=0.027), P=0.005) P=0.027)>
| Variables | uOR (95% CI) | P-value | aOR (95% CI) | P-value |
| Died | 0.82(0.43-1.55) | 0.55 | 0.53(0.23-1.24) | 0.15 |
| Any Complication | 1.17(1.08-1.26) | <0> | 1.08(0.99-1.18) | 0.060 |
| CSF leak | 1.19(1.04-1.36) | 0.010 | 1.00(0.86-1.15) | 0.99 |
| CNS Infection | 1.56(1.09-2.25) | 0.014 | 1.20(1.04-1.17) | 0.37 |
| Diabetes Insipidus | 1.09(0.98-1.20) | 0.082 | 0.99(0.88-1.10) | 0.85 |
| Iatrogenic Pituitary Disorder | 1.48(1.07-2.05) | 0.017 | 1.41(0.96-2.06) | 0.073 |
| Fluid and Electrolyte Disorders | 1.11(1.00-1.24) | 0.046 | 1.08(0.96-1.21) | 0.17 |
| Neurological Diseases | 1.05(0.90-1.22) | 0.46 | 1.05(0.90-1.24) | 0.49 |
| Pulmonary Diseases | 1.53(1.20-1.95) | <0> | 1.50(1.13-2.01) | 0.005 |
| Cardiac Diseases | 0.81(0.47-1.37) | 0.43 | 0.82(0.47-1.42) | 0.48 |
| Renal Diseases | 1.52(1.21-1.92) | <0> | 1.33(1.03-1.71) | 0.027 |
| Hemorrhage | 0.65(0.63-0.89) | 0.015 | 0.57(0.35-0.94) | 0.027 |
Table 7: Effect of obesity on endoscopic transsphenoidal pituitary surgery
Analysis of Mortality and Postoperative Complications Between Endoscopic Transsphenoidal and Transfrontal Approaches for Pituitary Surgeries
Among the surgical cases reviewed, 88,081 underwent endoscopictranssphenoidal approach, while 21,836 received a transfrontal approach. The analysis revealed that the transfrontal approach was associated with a higher incidence of mortality (0.88% vs. 0.38%, P<0 P=0.013),>
| Variables | Transsphenoidal (N=88081), % | Transfrontal (N= 21836), % | P-value |
| Died | 0.38% | 0.88% | <0> |
| Any Complication | 36.88% | 45.11% | <0> |
| CSF leak | 8.00% | 10.3% | <0> |
| CNS Infection | 0.86% | 1.27% | 0.013 |
| Diabetes Insipidus | 15.48% | 22.69% | <0> |
| Iatrogenic Pituitary Disorder | 1.03% | 2.00% | <0> |
| Fluid and Electrolyte Disorders | 14.70% | 19.92% | <0> |
| Neurological Diseases | 6.95% | 5.54% | <0> |
| Pulmonary Diseases | 1.85% | 3.52% | <0> |
| Cardiac Diseases | 0.58% | 0.67% | 0.45 |
| Renal Diseases | 2.01% | 3.03% | <0> |
| Hemorrhage | 0.99% | 1.08% | 0.60 |
Table 8: Comparison between Endoscopic transsphenoidal and transfrontal approach for mortality and postoperative complications
Over the decade spanning 2010 to 2020, patients undergoing endoscopic transsphenoidal pituitary surgery predominantly fell within the 25 to 44 age group, with a significant majority (61.47%) presenting no comorbidities (CCI = 0). Female patients slightly outnumbered male patients (51.18% vs. 48.82%). Private insurance was the primary coverage for most patients, followed by Medicare. While surgical interventions were broadly distributed across all income quartiles, the highest income group exhibited the greatest surgery rates. Predominantly, these procedures were executed in academic settings, with a staggering 90% taking place in large teaching hospitals. Regional analysis showed that Southern and Western centers accounted for a larger share of cases, surpassing those in the Midwest and Northeast. These findings suggest that socioeconomic factors significantly influence access to and outcomes of endoscopic transsphenoidal pituitary surgery. The distribution of surgeries across different income quartiles, with a skew towards higher income groups, indicates potential barriers to access for lower-income patients. This disparity emphasizes the need to address socioeconomic factors as key determinants of health care access and quality.
A previous study analyzing pituitary adenomas and carcinomas from 1997 to 2016 using the NIS database revealed a peak incidence among individuals aged 65 to 84 [1]. This trend suggests an enhanced detection of pituitary adenomas over the years, likely attributed to the proliferation of head imaging techniques that increase the rate of incidental findings [8]. Despite observing a higher incidence in women, statistical significance was not established in sex differences [1]. Interestingly, while urban centers reported a higher incidence rate, our analysis indicates a predominant surgical treatment of adenomas in academic centers [1]. This pattern implies a referral system funneling patients from rural or suburban diagnoses to academic surgical facilities, highlighting concerns about equitable access to care for those living far from such centers. Additionally, the most pronounced disparities were observed in the incidence and treatment utilization across different racial demographics. The notable emphasis on academic centers for surgical treatment raises concerns about access for patients in non-urban areas, potentially exacerbating existing socioeconomic and geographic disparities. This situation underscores the importance of developing strategies to ensure equitable access to specialized surgical care, irrespective of patients' geographical location or socioeconomic status.
Research reveals variable incidences of pituitary tumors across racial groups, with Black Americans experiencing nearly double the incidence rate of their White, Asian, and American Indian counterparts, particularly among older populations. Despite a similar peak incidence age between Black, White, and Asian Americans (75-79 years) as indicated in previous studies [8], our analysis uncovers a significant treatment gap, showing lower surgical intervention rates for Black Americans compared to White Americans. This disparity could be attributed to several factors, including higher stroke rates among Black Americans leading to more frequent imaging and incidental tumor findings not requiring surgery, systemic barriers limiting access to specialized neuro-oncological care and patient education, and insurance-based discrepancies. Predominantly, private insurance serves as the primary payer, whereas Black and Hispanic patients are more likely to depend on Medicare, Medicaid, or lack insurance, constraining their surgical treatment options. Furthermore, there appears to be a financial incentive for prioritizing well-insured patients, who are mostly White, for surgery over other monitoring approaches that might be equally viable. The disparities in surgical intervention rates among Black Americans compared to White Americans highlight significant racial inequalities in healthcare. These findings point to the need for targeted interventions to reduce barriers to care and improve surgical outcomes for racial and ethnic minorities. Understanding and addressing the root causes of these disparities, including systemic barriers and insurance-based discrepancies, are critical steps toward achieving equity in healthcare.
In our study, similar to patterns of utilization, we observed potential disparities in outcomes among different racial groups. Notably, both Black and Hispanic Americans exhibited higher odds of total postoperative complications compared to White Americans, with Black Americans experiencing not only higher mortality rates but also an increased incidence of specific complications such as diabetes insipidus, fluid/electrolyte disorders, and renal and urinary issues. This discrepancy might be linked to the higher prevalence of renal disease and hypertension observed in the Black population relative to White Americans. Furthermore, the connection between electrolyte/fluid disorders and income disparities could point to issues like inadequate nutrition or lower caloric intake, leading to electrolyte imbalances and compromised fluid status. These outcome disparities may stem from a range of underlying causes, including socioeconomic inequalities and diminished trust in the healthcare system, reflecting the complex interplay between health outcomes and social determinants of health.
Our study uncovered a notable discrepancy in postoperative complications based on the type of insurance, where patients covered by Medicaid experienced a higher rate of complications compared to those with private insurance, who demonstrated lower odds of such outcomes. Furthermore, we observed an inverse relationship between income levels and complication rates, with patients in the highest income quartile exhibiting lower odds of experiencing complications than those in the lowest quartile. These findings are consistent with prior research indicating an association between Medicare or Medicaid coverage and adverse outcomes, particularly in studies examining frailty [11]. Additionally, our results suggest a potential interaction effect between low-income status and increased frailty among patients undergoing pituitary surgery. This interaction could mean that the longer hospital stays, and higher medical expenses typically associated with frailty might exert a more significant burden on patients with lower income levels, highlighting the compounded impact of socioeconomic factors on health outcomes.
Our study revealed a notable difference in the proportion of patients experiencing CSF leak with the endoscopic and transfrontal approaches. The overall rates of CSF leak were lower than those typically reported in the literature, with 8.00% with the endoscopic approach and 10.3% with the transfrontal approach and were statistically significant (P<0>
In our analysis, after adjusting for age, sex, race, and CCI, we discovered that a BMI over 25 independently predicted an increased likelihood of pulmonary, renal, and hemorrhagic complications. This aligns with existing research indicating that obese individuals are at a heightened risk for various postoperative complications and hospital readmissions when compared to their non-obese counterparts [12, 13]. The elevated complication rates in obese patients have been attributed to both surgical and medical challenges [14, 15]. Specifically, studies have reported CSF leak rates exceeding 10% in obese patients [14, 15], a stark contrast to the 1.3% to 1.7% range observed in non-obese individuals [16, 17]. Moreover, medical issues like pneumonia contribute to the overall higher complication rates seen in the obese population [13], underscoring the complex interplay between obesity and postoperative health outcomes.
Our study is subject to several limitations that merit consideration. Firstly, the transition from ICD-9 to ICD-10 coding systems introduced significant changes. Additionally, the inconsistency in recording obesity before 2016 posed challenges in accurately assessing its impact on surgical outcomes. Despite these challenges, our results align with existing literature, underscoring their relevance. However, it's important to highlight that the database does not provide information on radiographic tumor characteristics, which means that patients predisposed to higher complication risks, possibly due to larger tumor sizes, cannot be distinctly identified through this analysis.
Despite advancements in endoscopic endonasal pituitary surgery, its access and utilization remain uneven across different populations, highlighting persistent disparities in healthcare access and outcomes influenced by socioeconomic factors, race, and ethnicity. Racial and ethnic minorities, in particular, experience higher rates of complications from such surgeries. The root causes behind these disparities are complex and multifaceted, with socioeconomic determinants of health playing a crucial role in these variations, thereby presenting numerous opportunities for in-depth research. It raises the question of whether these disparities stem from differing perceptions and acceptance of pituitary surgery among various racial groups, potentially with some groups more hesitant to undergo surgery, or if they are attributable to variations in access to healthcare financing and specialized care facilities capable of performing such surgeries. Additionally, the observed higher incidence of stroke and other comorbid conditions within the Black population might contribute to more incidental findings of pituitary issues and subsequently poorer postoperative outcomes, further complicating the landscape of healthcare equity in the context of pituitary surgery.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
