
Review Article | DOI: https://doi.org/10.31579/2578-8949/113
1 Department of Dermatology, Dermatology Institute of Guangzhou Medical University, Guangzhou, China and Guiyang Baiyun District People's Hospital, Guiyang, China.
2 Department of Dermatology, The Fifth Affiliated Hospital of Guangzhou Medical University, Guangzhou, China.
3 Department of Dermatology, Dermatology Institute of Guangzhou Medical University and Guangzhou Institute of Dermatology, Guangzhou, China.
# Manman Chen, reviewed the literature and drafted the manuscript and Xingdong Ye, conceptualized the article design, revised the draft, and provided the figures. All authors were involved in revising the manuscript and approving the final version.
*Corresponding Author: Xingdong Ye, Department of Dermatology, Dermatology Institute of Guangzhou Medical University, NO. 56, Heng Fu St, Guangzhou, Guangdong province, 510095, China.
Citation: Manman Chen, Zhimin Xie, Qingqing Li, Biaoyi Luo, Sifan Lin, Xingdong Ye, et al., (2023), Skin Barrier Dysfunction in Hand Eczema, Dermatology and Dermatitis, 8(3); DOI:10.31579/2578-8949/113
Copyright: © 2023, Xingdong Ye. This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 June 2023 | Accepted: 01 July 2023 | Published: 20 July 2023
Keywords: hand eczema; skin barrier; transepidermal water loss; filaggrin; staphylococcus aureus; antimicrobial peptides
Hand eczema (HE) is a common chronic inflammatory skin disease of the hand, the occurrence and development of which are related to the dysfunction of the topical skin barrier. Causes of topical skin barrier dysfunction include dysregulation of gene/protein expression, permeability barrier abnormalities, flora imbalance in the microbial barrier, and abnormalities of antimicrobial peptides in the immune barrier. Because the incidence rate of HE is high and the disease is likely to recur, we wrote this review to identify pathogenic factors through skin barrier analysis of HE and to explore more favorable treatment methods. Previous studies have shown that the mutation of the filaggrin gene, a medical history of atopic dermatitis, and the hyperproliferation of Staphylococcus aureus in lesions are related to the prolongation of HE. Moreover, high pH value, increased transepidermal water loss, and damaged integrity of the stratum corneum are closely related to the activity and severity of chronic HE with or without atopic dermatitis. The S100 family of antimicrobial peptides, including S100A7A, S100A7, S100A8/A9, and S100A11, has also been shown to be highly expressed in vesicular and hyperkeratotic HE.
Hand eczema (HE) is a common chronic hand disease, with a prevalence rate of 5%-8% in the general population and a 1-year incidence in adults of 10%, which is comparable to that in adolescents [1]. The average age of onset is approximately 20 years old [2]. In the age group of < 30 years, women are more affected than men. The reason for this phenomenon is that women are more likely to hold jobs involving wet work, and women aged 20–29 often engage in wet household chores, including taking care of children [3]. Among HE patients, up to 50% have atopic HE [4].The prevalence of HE in patients with atopic dermatitis (AD) is increasing significantly, and the probability of patients with a current or previous history of AD suffering from HE is increased by 2–4 times [5]. Patients with recurrent chronic HE (CHE) are prone to anxiety and depression, and the clinical symptoms can lead to a decline in patients’ quality of life [6]. Therefore, HE is a disease that deserves continued research efforts. Studies have shown that the occurrence and development of HE are related to skin barrier dysfunction [7].
1 Etiology and classification of HE
The etiology of HE is complex and can be divided into exogenous and endogenous factors. The former mainly encompasses irritant and allergic substances, and the latter mainly refers to atopic constitution. Most patients with HE present a mixed etiology, [8] andamong the atopic constitution, a medical history of AD and contact sensitization are related to persistent HE [9]. Regarding the exogenous factors, contact allergens mainly include nickel sulfate (27.06%), cobalt chloride hexahydrate (23.52%), phenyl peroxide (11.76%), and hydroperoxide of linalool (11.76%) [10]. The clinical classification of HE has not yet been unified but is divided into endogenous HE and exogenous HE according to the Chinese expert consensus on HE [11]. Exogenous HE includes irritant contact dermatitis (ICD), allergic contact dermatitis (ACD), contact urticaria (CU), and protein contact dermatitis (PCD), whereas endogenous HE includes atopic HE, vesicular endogenous HE, and hyperkeratotic endogenous HE. HE can also be divided into acute hand eczema (AHE) and CHE based on the disease course. According to the characteristics of clinical manifestations, we propose to simply divide HE into vesicular/bullous HE (e.g., vesicular/bullous HE resulting from both endogenous or exogenous factors, regardless of acute or chronic) and hyperkeratotic HE (Figure 1). Vesicular/bullous HE is mainly characterized by manifestations of acute-phase HE, such as honeycomb vesicle exudation and erosion, with conscious pruritus and scales in the later stage. Hyperkeratotic HE is characterized by dryness, scales, and even fissures, but no vesicular presentation throughout the disease course [12]. HE can also be classified according to the morphology of skin lesions, such as pompholyx (Figure 2), vesicular/bullous HE (Figure 3), discoid eczema (Figure 4), fissured HE (Figure 5), hyperkeratotic HE (Figure 6), and digital abdominal dermatitis [13]. However, this classification is seldom used because it lacks targeted guidance for HE prevention and treatment.Treatment strategies for HE should consider clinical manifestations and skin lesion morphology, whereas prevention strategies should be based on etiology and damage to the skin barrier.
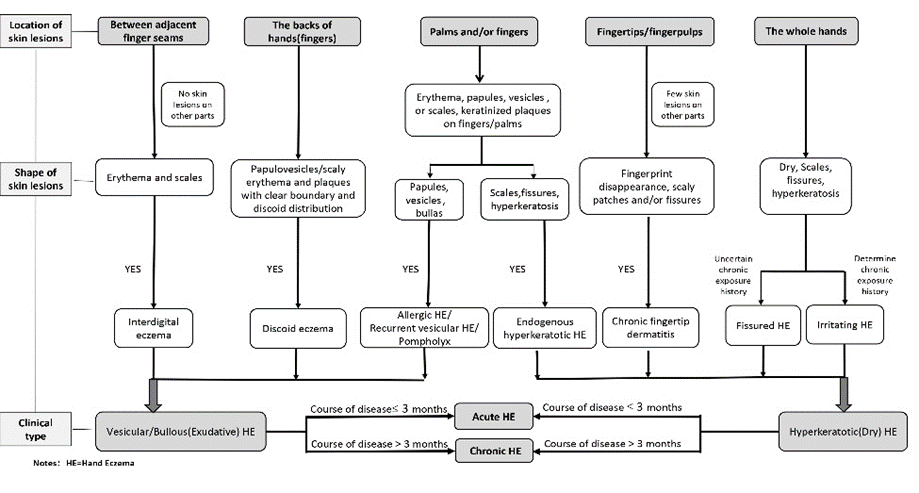
Figure 1. Flowchart of classification and diagnosis of hand eczema.

Figure 2. Pompholyx (clusters of thick-walled vesicles are marked with red arrows)

Figure 3. Vesicular/bullous hand eczema (Acute-phase lesions include vesicles and erosions marked with red arrows)

Figure 4. Discoid eczema (a subacute erosive plaque is indicated by the red arrow)

Figure 5. Fissured hand eczema (linear gaps are marked with red arrows)

Figure 6. Hyperkeratotic hand eczema (hyperkeratotic patches with fissuring are marked with red arrows)
2 Skin barrier
The skin barrier can be defined in a narrow sense or a broad sense. In the narrow sense, the skin barrier refers only to the permeability barrier of the skin. In the broad sense, the skin barrier includes the skin permeability barrier, microbial barrier, chemical barrier, physical barrier, and immune barrier.
The skin permeability barrier is mainly composed of keratinocytes and intercellular lipids in the epidermis, or keratinocyte and the cornified envelope (CE) in the stratum corneum (SC), which form a brick-wall-like structure. The microbial barrier, located in the outermost layer of skin, is composed of microbiota of different species, and it is the first active defense barrier against environmental invaders. The chemical barrier is composed of antimicrobial peptides (AMPs) and natural moisturizing factors (NMFs). AMPs are considered the immediate first-line response to microbial pathogens by the innate immune system. Associated with skin pH and the composition of epidermal lipids, NMFs are metabolized from filaggrin (FLG) and are crucial to the function of the epidermal barrier. SC and tight junction (TJ) proteins have a critical role in the physical barrier [13]. The skin can prevent harmful external factors from invading and maintain the balance of nutrients, such as water and electrolytes, in the internal environment, largely mediated by the TJ and SC. Proteins in the TJ, including the claudin, occludin, and zonula occluden families, are considered as barriers that regulate water and solute transport [14]. The immune barrier is dynamic and consists of resident cell groups, including dendritic cells, innate lymphocytes, natural killer cells, and regulatory T cells in the epidermis and dermis of skin. Resident cells of the immune barrier can promote barrier repair and internal environment stability, so defects in skin barrier function have the potential to cause many diseases, especially skin-related diseases.
3 Permeability barrier of HE
A study by Wang et al. [15] in China showed that in patients with moderate and severe CHE, the integrity of the SC was damaged, the pH value and transepidermal water loss (TEWL) of “normal-appearing” skin were significantly higher than those of healthy volunteers, and the water content of skin was lower than that of healthy volunteers. Tauber et al. [16] used latent class analysis to categorize 71 patients with CHE (among whom hyperkeratotic HE accounted for 60.6%) and showed that the degree of skin barrier dysfunction—including high TEWL and HI, high staphylococcus colonization, high IL-8 level, and high FLG gene mutation frequency—was the most important parameter to distinguish patients with CHE. Additionally, Jungersted et al. [17] studied skin barrier differences in various types of HE and found no significant difference in SC lipids or susceptibility to sodium lauryl sulfate (SLS) between exogenous allergic/irritant HE and endogenous hyperkeratotic HE. Although the permeability barrier of HE has known dysfunction, whether there are differences in the permeability barrier of various types of HE is worthy of further study.
The expressions of various skin permeability barrier-related genes/proteins are abnormal in the lesions of hyperkeratotic HE. In a study by Kumari et al., [18] lesions were collected from 15 patients with chronic hyperkeratotic HE before and after systemic alitretinoin treatment. Subsequently, reverse transcription-quantitative polymerase chain reaction (RT-PCR) and immunohistochemistry were employed to detect the expression of several skin barrier proteins and genes, including Ki-67, three TJ proteins (claudin 1, claudin 2, and occludin), and two KC envelope proteins [loricin (LOR) and transglutaminase 1], two cytoskeleton proteins (KRT10 and FLG), and the thymic stromal lymphopoietin (TSLP) gene. The results showed that the expression of Ki-67 increased in the upper basal part of skin lesions, the expressions of claudin 1, FLG, LOR, and KRT10 decreased, and the expression of TSLP increased. Additionally, there was a negative correlation between TSLP and FLG expression. After alitretinoin treatment, the expression of Ki-67 decreased significantly, the expression of claudin 1 increased, the expressions of FLG, LOR, KRT10, and TSLP were normal, and the expressions of claudin 1, FLG, and LOR were significantly correlated with the severity of HE, confirming that hyperkeratotic HE is associated with disorder of barrier-related gene/protein expression. Politiek et al. [19] also found that the number of Ki-67-positive cells increased, the expressions of K9 and K14 decreased significantly, and the expressions of K5, K6, K16, and K17 increased in hyperkeratotic HE. Moreover, the upregulation of keratin K6, K16, and K17 has been shown to lead to proliferation and hyperkeratosis in KC [20]. Additionally, Molin et al. [21] analyzed the proteomic characteristics of palm tissues from six patients with CHE and six healthy controls using liquid chromatography-tandem mass spectrometry (LC-MS/MS) analysis and label-free quantification. The results showed that the barrier proteins FLG, FLG2, and hornerin were downregulated in patients with CHE. Moreover, the desquamation-related enzymes kallikrein-related peptidase 5, 7 and cystatin E/M were downregulated, and the expression of SPPR2B was upregulated in diseased skin.
Moreover, genes/proteins of epidermal proliferation and differentiation (e.g., SPRR2A, SPRR2B, SPRR2D, SERPINA3, SERPINB3, and SERPINB4, and keratin family members KRT6, KRT16, and KRT17) and LOR (a protein related to epidermal differentiation) have been shown to be downregulated in the skin lesions of vesicular HE [22].
In KC densification and SC formation, FLG is a structural protein of the SC, which enriches keratin filaments. Wong et al. [23] reported that the mice FLG gene mutation led to dry and desquamated skin, abnormal accumulation of keratin, damage of the epidermal permeability barrier, and allergen invasion. Additionally, Molin et al. [21] reported that FLG content was decreased in lesions of HE. Thyssen et al. [24] reported that FLG mutations increased the risk of HE in patients with atopic dermatitis from adolescence to adulthood. FLG mutation sites are associated with clinical manifestations of HE as follows: 1) two FLG gene mutations, namely, heterozygous of R501X or 2282del4, are relevant to irritant HE complicated with allergic CHE [25]; 2) the heterozygous S2889X mutation is common in Indian patients with HE [26]; and 3) the FLG null mutation is significantly associated with atopic HE (less than 12 months) [24]. These findings imply that the mutation of the FLG gene is related to the pathogenesis of HE. Of course, not all cases of HE are associated with FLG mutation, and some cases have similar basic barrier functions regardless of the presence of FLG mutation [27,28]. However, patients with AD with FLG mutation have a risk of combined HE [9,29], with greater severity [30]. In patients without a medical history of AD, FLG mutation does not significantly increase the risk of HE [31, 32]. Therefore, FLG mutation may be an important genetic factor of atopic HE, which is related to the severity of atopic HE. The relationship between other subtypes of HE and FLG mutations needs to be further studied.
Sirtuin 1 (SIRT 1) is a nicotinamide adenine dinucleotide-dependent protein with multiple roles in the process of aging and disease development [33]. Ming et al. used a mouse model to show that FLG is regulated by the protein deacetylase SIRT1 and that SIRT1 is critical for skin barrier integrity [34]. They also demonstrated that the SIRT1 protein level was downregulated in human AD and non-AD. The study by Shin et al. confirms the above results and indicates that SIRT1 promotes activation of the aryl hydrocarbon receptor, and the aryl hydrocarbon receptor ligand restores FLG expression in SIRT1-inhibited cells [35]. Therefore, we speculate that in HE with low FLG expression, SIRT 1 activators may be important for treating HE, and SIRT 1 inhibitors may promote HE and accelerate aging.
In brief, although the skin’s permeability barrier is clearly dysfunctional in HE patients, more in-depth research is needed, especially regarding differences in the skin barrier between patients with different types of HE. We assume that the dysregulation of gene/protein expression relative to the skin barrier is closely associated with a subtype of HE. However, because previous studies show that many candidate genes/proteins are associated with different subtypes of HE, it is difficult to determine the genes/proteins affecting the skin barrier of a specific subtype of HE. Currently, among the most studied genes, FLG mutation is considered as an important genetic factor of atopic HE related to the severity and duration of HE. FLG mutation detection in patients with AD is expected to represent an index to judge the presence of atopic HE, HE severity, or the prognosis of CHE.Further research on SIRT1 activators may have important implications for the treatment of AD and HE.
4 Microbial barrier of HE
The microbial barrier of the skin refers to the microbial ecosystem in the outermost layer of skin, in which microorganisms adapt to each other and conduct mutual checking and balancing to form a steady-state microenvironment, which can inhibit the proliferation and pathogenesis of pathogenic bacteria. An imbalance in flora leads to skin barrier damages, which is further exacerbated by the abnormal proliferation of pathogenic bacteria. Indeed, Staphylococcus aureus (SA), which is the most common epidermal pathogen, can produce a super-antigen and result in severe allergic inflammation of the skin [36]. Microbiota imbalance is also associated with the severity of AD and increased colonization of SA [37]. Moreover, the occurrence of SA colonization in skin lesions in patients with HE is higher than that on non-lesioned skin. Nørreslet et al. [38] conducted a study in which lesion swabs were collected from patients with HE for seven consecutive days and cultured for bacteria, revealing that SA culture results were positive at least once in 54% of patients, and the number of SA colonies was positively correlated with the severity of HE. Additionally, in the hands of patients with HE, the number of SA colonies in patients with AD was higher than that in patients without a medical history of AD.
FLG mutation is considered beneficial to SA skin colonization in patients with AD, [39] but whether it is beneficial to SA skin colonization in patients with HE with or without AD requires further study. Chen et al. [40] reported that SA colonization is common in CHE, with an SA positive rate of 30.0% in reproductive culture, and 37.5% by PCR. Additionally, topical antibiotic treatment (compound preparation of 0.05% halometasone monohydrate and 1% triclosan) is effective for SA colonization. Moreover, a study by Xin et al. [41] showed that the severity of CHE is related to SA colonization, and the elimination of SA colonization is helpful in the remission of CHE. Furthermore, Nørreslet et al. [42] reported the temporal stability of the SA clonal complex and the high incidence of the same subtype in the hand and nose, suggesting that the colonization of SA is permanent in patients with HE.
In conclusion, a high SA colonization rate was observed in all subtypes of HE, especially in atopic HE. SA colonization was significantly associated with severity and chronic prolongation of HE. The elimination of SA colonization is beneficial to alleviate HE and to reduce relapse. Therefore, routine detection of SA and topical antibiotic application to inhibit SA colonization during the acute stage will help to prevent CHE occurrence, which is worthy of further study.
5 Immune barrier of HE
Irritant contact dermatitis is the most common subtype of HE, and contact sensitization is caused by a T cell-mediated immune response. The activation of allergen presenting cells and the formation of allergen-specific T cells are part of the initial sensitization phase, which stimulates the release of inflammatory mediators when recontacting allergens [43]. Keratinocytes convert inactive prohaptens into biologically active haptens and play an important role in the inflammatory eczema response by producing various cytokines and alarmins [44]. The immune barrier of the skin consists of cellular and humoral immunity. Cellular immunity includes keratinocytes, Langerhans cells, neutrophils, macrophages, and endothelial cells. Humoral immunity includes AMPs, complement, immunoglobulins, cytokines, plasmin, arachidonic acid, and neuropeptides. AMPs are important immune defense molecules produced by neutrophils, Paneth cells, mast cells, epithelial cells, and adipocytes. AMPs can promote innate and adaptive immune responses, conduct the initial defense response against microbial pathogens, and directly kill or inactivate many microorganisms, including gram-positive and gram-negative bacteria, fungi, certain viruses, and parasites. AMPs have been found in animals, plants, and microorganisms. AMPs are mainly defensins in vertebrate species, including the S100 family, RNase A family, and cathelicidins. LL-37 is the only known cathelicidin in humans, which is widely distributed throughout skin. LL-37 expression is negligible in healthy skin but significantly increases after infection, inflammation, or injury [45]. Turner et al. 46 observed that LL-37 in sweat has antibacterial activity against bacteria including SA and Staphylococcus epidermidis. Niyonsaba et al. [47] discovered that a low concentration of LL-37 can inhibit susceptibility to skin infection in patients with AD. Vitamin D is an important regulatory factor of LL-37. Indeed, 1,25(OH)2D3-dependent signal activation in keratinocytes leads to the production of Toll-like receptor (TLR) 2/CD14 dependent LL-37. 48 Kanda et al. [49] reported that serum levels of both LL-37 and 25(OH)D3 are reduced in patients with AD, while multiple proteins of the S100 family (S100A7A, S100A7, S100A8/A9, and S100A11) are highly expressed in HE [21,22]. However, there is no relevant research on whether the expression of LL-37 is unbalanced in HE.
Additionally, transcriptome analysis of vesicular HE by Voorburg et al. [22]showed significant upregulation of several genes involved in keratinocyte host defense and inflammation (e.g., LTF, LYZ, LCN2, LCE3A, and PI3) and immune signaling (MMP12, CHI3L2, CCL22, and IL4R)in the lesional skin of patients with vesicular HE. In contrast, the expressions of IL37 and LCE1D/E (host defense-related proteins) were significantly downregulated in skin lesions.
The above findings highlight the abnormal skin immune barrier in HE, with clear dysregulation of some proteins in the S100 family and genes, proteins, and cytokines that are related to host defense and inflammation. Comprehensive relevant studies are needed to find indicators to evaluate the severity of HE, as well as to identify relevant targets for targeted therapy. We believe that LL-37 is an important research direction since LL-37 has anti-inflammatory and antibacterial effects. If it is confirmed that LL-37 has expression imbalance in HE and is related to the severity of the disease, it will be a good indicator for evaluating the severity of HE. If the levels of LL-37 and 25 (OH) D3 in the serum of HE decrease, considering the regulatory effect of vitamin D on LL-37, it would suggest that patients can be advised to supplement vitamin D appropriately during treatment.
There are many skin barrier abnormalities in patients with HE. FLG gene mutation, which is related to the prolongation of HE in patients with AD, is poorly understood in patients without AD. SIRT1 is crucial for maintaining the integrity of the skin barrier and has a regulatory effect on the expression of FLG. Therefore, further research on SIRT1 activators may be of great significance for both the treatment of AD and HE with low FLG expression. Moreover, SA colonization and abnormal proliferation are closely related to the activity and severity of atopic HE and CHE. In CHE lesions, the pH value and TEWL are increased, and the integrity of the SC is damaged. Since each subtype of HE has unique barrier issues, the management strategy of HE should focus on inflammation reduction, moisturization, and promotion of barrier repair according to the specific subtype. The expression differences between vitamin D-dependent LL-37 and other AMPs in different subtypes of HE also requires further study.
The authors report that they do not have any conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
