
Research Article | DOI: https://doi.org/10.31579/2641-0419/170Copyright
Department of Cardiovascular Surgery, Yozgat State Hospital, Yozgat, TURKEY
*Corresponding Author: Görkem Yiğit, Department of Cardiovascular Surgery, Yozgat City Hospital, Yozgat, TURKEY
Citation: Görkem Yiğit (2021) Single Center Experience in Vascular and Endovascular Surgery during the COVID-19 Pandemic: Walking on the Icy Road. J. Clinical Cardiology and Cardiovascular Interventions, 4(9); Doi:10.31579/2641-0419/170
Copyright: © 2021 Görkem Yiğit, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 April 2021 | Accepted: 27 April 2021 | Published: 03 May 2021
Keywords: coronavirus disease 2019; embolectomy; traumatic vascular injury; vascular surgery; endovascular surgery
Background: Along with other areas of specialization, the cardiovascular surgery clinic is a department that has a significant contribution to the COVID-19 pandemic process with both the management of vascular emergencies and the rapid and effective use of interventional methods. This study aims to present endovascular and open vascular surgical procedures performed in single center between March 2020 and December 2020 during the ongoing pandemic.
Materials and methods: A total of 230 patients underwent open surgery 60 patients and endovascular / interventional treatment 170 patients by the Cardiovascular Surgery clinic were included in the study. It was aimed to determine the procedural details of the patients, follow-up results, complications and mortality rates. The compatibility of the variables to normal distribution was examined using visual and analytical methods. The Shapiro-Wilk test was used to check the normal distribution of continuous variables.
Results: In the open vascular surgery group, the mean age was 51.4±23.2 years (range 12–90 years). Sixteen (26.7%) patients were female and 44 (73.3%) male. The median follow-up from the time of the open vascular procedure was 4.3±1.2 months. There were ten (16.7%) minor complications. There were five deaths after procedures. In the endovascular / interventional group, the mean age was 58.5±18.6 years (range 18–94 years). Ninety one (53.5%) patients were female and 79 (46.5%) male. The median follow-up from the time of the drug-eluting balloon angioplasty and pharmacomechanical thrombectomy patients were 4.0±1.1 months. There were thirty four (20%) minor complications and two deaths after procedures.
Conclusion: Our experience and successful results shows how surgical and interventional procedures participated in the care of hospitalized COVID-19 patients during the height of the coronavirus pandemic.
The pandemic spread of the novel coronavirus (SARS-CoV-2; COVID-19) has seriously affected the delivery of health care services around the world. [1] Patients who are hospitalized, respiratory and renal insufficency can be seen in addition to cardiac damage due to venous and arterial thromboembolism in severe COVID-19 disease. [2]
Along with other areas of specialization, the cardiovascular surgery clinic is a department that has a significant contribution to the pandemic process with both the management of vascular emergencies and the rapid and effective use of interventional methods. In this period, cardiovascular surgeons and interventional radiologists can place tunneled-cuffed or temporary hemodialysis catheters in patients with COVID-19 who develop renal failure, as per their experience. [3] Besides this, acute limb ischemia and major traumatic vascular injuries are significant vascular emergencies that require fastly and early intervention, resulting in functional deficit, limb loss, and even death. [4] Moreover, in selected patients with proximal deep vein thrombosis (DVT), pharmacomechanical thrombectomy (PMT) and catheter-directed thrombolysis can be performed in terms of life-threatening venous thromboembolism (VTE). [5]
This study aims to present endovascular and open vascular surgical procedures performed in single center between March 2020 and December 2020 during the ongoing pandemic.
During the pandemic period between March 2020 and December 2020, 300 patients who underwent open surgery due to vascular injuries and acute embolism or endovascular / interventional treatment due to hemodialysis (HD) catheter placement, pharmacomechanical thrombectomy for deep venous thrombosis and chronic critic leg ischemia by the Cardiovascular Surgery clinic were screened. Data were retrieved from the electronic patient’s records. Patients who were taken to elective surgery, had incomplete information in their files, and did not agree to participate in the study protocol were excluded from the study.
Finally, a total of 230 patients who underwent vascular surgery or endovascular treatment
were included. There were 60 patients in the vascular surgery group and 170 patients in the interventional treatment group. The patients in the vascular surgery group were evaluated retrospectively in terms of accompanying comorbid diseases, injury sites, type of anesthesia, surgical procedure, operation time, complications, intensive care and hospital stay and follow-up results. [4,6] The patients in the interventional group were evaluated retrospectively in terms of comorbid diseases, type of interventional or endovascular treatments, duration of procedure, type of anesthesia, and complications. [7] The demographic data and procedural details of both groups are shown in Table 1 and Table 2.
Open vascular procedures
In patients who were evaluated as an outpatient clinic by cardiovascular surgery, the patient's history and physical examination revealed that the presence of pulse deficit, coldness, cyanosis, uncontrollable or pulsatile bleeding at the injury site, enlarged or large hematoma, murmur or trill were interpreted as vascular injury findings. [4] The rapid COVID-19 PCR swab test was taken in patients who were diagnosed quickly, without the need for advanced diagnostic methods, and after the patient was taken into operation. Blood and blood products have been used in multi-trauma patients with excessive blood loss and haemodynamic instability. In addition, the operations were carried out simultaneously with other surgical specialists.
Patients who presented with limb pain, pallor, coldness, and discoloration and who were found to have an appearance consistent with acute embolism as a result of contrast-enhanced extremity computed tomography (CT) angiography were taken into emergency surgery. [4] Simultaneously, high resolution Thorax CT imaging was performed and rapid COVID-19 PCR swab test was taken for all patients.
General (61.7%) and local anesthesia (38.3%) was preferred in patients undergoing open surgery. After the hemodynamic stabilization of the patients was achieved, if there was no contraindication, 100 U / kg heparin IV bolus was given before placing the vascular clamp. [4] Subsequently, the proximal and distal ends of the injured vascular structures were determined visually, and if necessary, thrombectomy was performed first with a Fogarty catheter. Primary repair or saphenous vein graft interposition is aimed in the anastomosis in order to ensure the continuity of the vascular structures and optimum circulation. No ligation was performed in any vascular injury patient. Tetanus prophylaxis was administered to all patients presenting with vascular injury or acute limb embolism in the emergency department. After the operation, antibiotherapy and low molecular weight heparin were started during their hospitalization. [4,6] In addition, the necessary medications were added to the patients whose COVID-19 PCR test was positive. Later, the follow-up of the patients was continued with the infection and microbiology physician. In the presence of other accompanying tissue and organ injuries, the relevant branch physician was enabled to participate in the operation and the patient was followed up together.
Endovascular and interventional procedures
In the interventional group, COVID-19 PCR swab samples were obtained from all patients. If the patients were diagnosed with acute renal failure (ARF) during outpatient or ward follow-ups, a temporary hemodialysis (HD) catheter was placed under local anesthesia and under sterile conditions at the bedside or in the outpatient operating room. [7] A bedside temporary HD catheter was placed in patients who developed ARF during intensive care unit follow-ups. Permanent tunneled HD catheter was placed in the operating room under fluoroscopy and under local anesthesia in patients who developed chronic renal failure (CRF) and needed long-term dialysis. Permanent tunneled HD catheters were placed in the internal jugular vein in 20 patients and femoral vein in 2 patients using the standard Seldinger method.
Besides, symptomatic cases involving the lower extremity iliac veins and presenting within 14 days were hospitalized by starting low molecular weight heparin. Then, in the angiography unit under local anesthesia, the vena cava inferior filter was placed from the contralateral leg, and pharmacomechanical thrombectomy and catheter-mediated thrombolysis was performed from the occluded leg. Afterwards, oral anticoagulation was continued and they were discharged.
Appropriate patients who did not have acute ischemia, were followed up with maximal medical therapy from the outpatient clinic and had intermittent claudication with resting pain were hospitalized. Subsequently, digital subtraction angiography (DSA) imaging and drug-eluting balloon angioplasty (DEB) / stent procedures were performed on these patients in our angiography unit. Prior to PTA, all patients were evaluated with Duplex ultrasound and DSA. In the clinical practice of our department, PTAs are performed under local anesthesia with monitorization by cardiovascular surgeons in the hybrid operating theater. [8] We usually prefer antegrade femoral or contralateral retrograde femoral access. Following the insertion of a 7-Fr single lumen sheath, intravenous heparin is administered according to an activated clotting time (ACT) of 180 to 200 sec. [8] All lesions are dilated with PCB (at a vessel/balloon ratio of 1:1 on the basis of visual estimate) for a total inflation time of 3 min at 6 to 14 atm. Balloons are inflated only once. However, when control angiography reveals a residual lesion (>50% stenosis), flow-limiting dissection or atherosclerotic plaque deformation, a second PCB is carried out and dilatation is maintained for a longer period (≥3 min). In such cases in which residual stenosis or flow-limiting dissection persists after repeated dilatation, self-expanding nitinol stents are implanted as bail-out therapy. [8]
This retrospective study has been conducted in accordance with the principles of the Helsinki Declaration and approved by the Yozgat City Hospital and Yozgat Provincial Health Directorate Commitee (Date: 21.12.2020, No: 92198657-000-7080).
All statistical analysis was performed using the SPSS version 21.0 software (SPSS Inc., Chicago, IL, USA). Descriptive data were expressed in mean ± standard deviation (SD) or median (min-max) for continuous variables and in number and frequency for nominal variables. The compatibility of the variables to normal distribution was examined using visual (histogram) and analytical methods (Kolmogorov-Smirnov / Shapiro-Wilk Tests). The Shapiro-Wilk test was used to check the normal distribution of continuous variables. A p value of ˂0.05 was considered statistically significant. The graphs are edited with the GraphPad Prism version 8.0.3 (GraphPad Software, La Jolla, CA, USA) software.
Among the 230 patients hospitalized during the pandemic period between March 2020 and December 2020, there were 60 (26.1%) patients underwent open vascular procedures and 170 (73.9%) patients endovascular / interventional treatment. Demographic characteristics and procedural details of the patients in vascular surgical group was shown in Table 1.
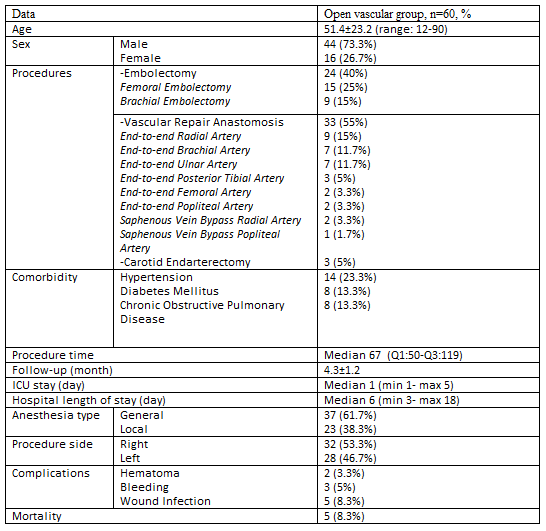
Open vascular surgical procedures were performed utilizing general anesthesia in 37 (61.7%) patients, mild sedation and local anesthetic only in 23 (38.3%). The median length of intensive care unit (ICU) stay was 1 day (range 1–5 days). The median length of hospitalization was 6 days (range 3–18 days). The median follow-up from the time of the open vascular procedure was 4.3±1.2 months. There were ten (16.7%) minor complications. There were five deaths after procedures. Four patients in embolectomy group because of older ages and severe COVID-19 pneumonia. One patient was admitted with a gunshot injury, severe hemodynamic impairment and major bleeding, and the saphenous vein bypass was applied to the popliteal artery, but the patient died in the intensive care follow-up.
Demographic characteristics and procedural details of the patients in endovascular / interventional group was shown in Table 2.

Bedside procedures included placement of tunneled or temporary HD catheter. Other procedures were performed in the angiography unit. Endovascular / interventional vascular procedures procedures were performed utilizing general anesthesia in 2 (1.2%) patients, local anesthetic only in 168 (98.8%). The median length of hospitalization in drug-eluting balloon angioplasty and pharmacomechanical thrombectomy patients were 2 days (range 3–10 days). The median follow-up from the time of the drug-eluting balloon angioplasty and pharmacomechanical thrombectomy patients were 4.0±1.1 months. There were thirty four (20%) minor complications. There were two deaths after procedures. One patient who underwent pharmacomechanic thrombectomy for DVT died after cardiac arrest due to pulmonary embolism. The other patient died because of older age and severe COVID-19 pneumonia in the ICU unit.
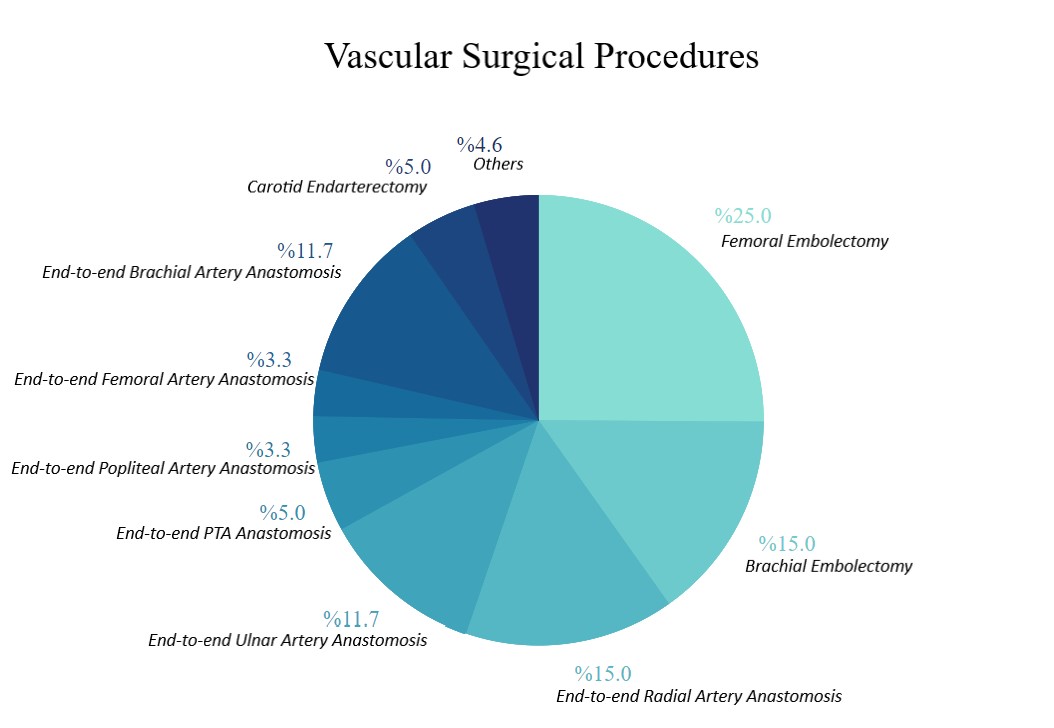
Also, procedural details of the patients in both groups were shown in Graphic 1 and 2.
Graphic 1: Vascular surgical procedural details of the patients.
As a result of the severe COVID-19 pandemic all over the world, health care systems have been disrupted, however, it has been decided that elective surgical cases should be postponed worldwide. [9,10] Given these discussions, most vascular surgeons have reduced their practice patterns to emergency vascular surgery and very urgent cases.
In treating COVID-19 or suspected patients, it is very important to perform surgical procedures using personal protective equipment (PPE) in emergency cases. In addition, appropriate sterilization should be done between cases and patient-based protocols should be applied. [11] Procedures that can be applied to the bedside are very important in terms of preventing minimal contact and inter-patient transmission. Compared to surgeries in the operating room, interventional radiology procedures may potentially require less PPE and less support staff. [11] During the operations of COVID-19 or suspected patients, it is also recommended to use glasses, visors and double-layer gloves. [12]
As known, acute limb ischemia (ALI) is an important condition that leads to limb loss an deven death of patient if the diagnosis is delayed. [13] The rate of limb loss in ALI is about 40% with a high mortality rate ranging between 15 and 20%. [14] In the present study, there were no limb loss in any of the patients and postoperative mortality in 4 patients in their follow-up because of COVID-19 pneumonia and older age. However, another important issue is traumatic vascular injuries. Vascular injuries constitute approximately 2-3% of all injuries. [4] These life-threatening serious injuries can cause loss of limb function or limb loss if they are not treated timely and appropriately. [4,6]
Multisystemic organ failure associated with COVID-19 requires a multidisciplinary approach by many specialists. Among these, radiologists, neurologists, cardiovascular surgeons and cardiologists with interventional radiology experience play an important role in this field. Immune system activation due to COVID-19 causes prothrombotic conditions to occur. [15] For this reason, it is very important to diagnose DVT and start an appropriate anticoagulant regimen in patients who are hospitalized for a long time due to COVID-19. However, the management of these phenomena can be very difficult and complex. PMT treatment can be considered as an important option in suitable patients with low bleeding risk, young age, no history of cancer and no history of recurrent thrombosis. [16] In patients hospitalized for severe COVID-19, acute pulmonary embolism (PE) detected by imaging methods is seen in 30% of patients. [17] Especially the management of these cases is very difficult due to coagulopathy and anti-thrombotic treatments. [18] In addition, the effectiveness of inferior vena cava (IVC) filter placement in these patients is unknown.
When renal complications associated with COVID-19 were examined, 36.6% of hospitalized patients had acute kidney injury, and 14.3% of them required dialysis and renal replacement therapy. [19] In our clinic, we frequently place a temporary hemodialysis catheter from the femoral vein as bedside in patients with acute renal failure.
Although this study has some limitations including retrospective and single-center design with a relatively small sample size.
The present study shows how surgical and interventional procedures participated in the care of hospitalized COVID-19 patients at a tertiary care center in Yozgat City during the height of the coronavirus pandemic. In the face of this highly contagious disease, it is critical to have infection control measures, whether invasive or open procedure or not. As cardiovascular surgeons, feel comfortable doing our best in this challenging process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
