
Case-Report | DOI: https://doi.org/10.31579/2641-0419/099
*Corresponding Author: Xuguang Qin, Department of Cardiology, Beijing North Asia Orthopedics Hospital. Beijing 102445, People's Republic of China,
Citation: Xuguang Qin., Weiguo Xiong., Lin Yang., Chunpeng Lu., (2020) Simple Provisional Stenting or two-stent Strategies to Treat Anomalous Right Coronary Originating from the mid of left Anterior Descending Coronary Artery. J. Clinical Cardiology and Cardiovascular Interventions, 4(1); Doi:10.31579/2641-0419/099
Copyright: © 2020 Xuguang Qin, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 October 2020 | Accepted: 07 November 2020 | Published: 13 November 2020
Keywords: percutaneous coronary intervention; single coronary anomaly; anomalous right coronary artery; bifurcation lesions; DK- culotte crush stenting
Congenital anomalies of coronary arteries (CAAS) are very rare and usually documented as an incidental finding during routine catheter or CT angiograms performed for other reasons. Their prevalence ranges from 0.2% to 1.3% based published series. The most common coronary artery anomaly is origination of the left circumflex coronary (LCX) artery from the proximal of right coronary artery (RCA) or right sinus of Valsalva. The second is separate origination of the left anterior descending coronary artery (LAD) and LCX artery from the left sinus of Valsalva. Herein, we present three cases that the anomalous RCA arises from the mid of left anterior descending coronary artery (LAD). The bifurcation lesions of first case was treated using two-stent strategies of DK culotte, excellent angiography results was observed. The last two cases were treated using simple provisional stenting strategy: one stent was deployed crossover the ostium of the anomalous coronary artery, final angiographic results were excellent. These cases are extremely rare. We bring forth them in an attempt to highlight their significance, and make cardiologist to understand what important the anomalies are, and the strategy how to treatment these bifurcation lesions.
Congenital anomalies of coronary arteries (CAAS) are very rare and usually documented as an incidental finding during routine catheter or CT angiograms performed for other reasons. Their prevalence ranges from 0.2% to 1.3% based published series [1-4]. The most common coronary artery anomaly is origination of the left circumflex coronary (LCX) artery from the proximal of right coronary artery (RCA) or right sinus of Valsalva. The second is separate origination of the left anterior descending coronary artery (LAD) and LCX artery from the left sinus of Valsalva. Bifurcation disease accounts for 15-20% of coronary interventions. According to the 2011 American College of Cardiology (ACC) guidelines, provisional side branch stenting should be the initial strategy (class I recommendation) when the side branch is not large and has only mild to moderate ostial disease, while elective side branch stenting is reasonable (class IIA) if the side branch is large with a high risk of occlusion and the likelihood of side branch reaccess is low. Herein, we present three cases that the anomalous RCA arises from the mid of left nterior descending coronary artery (LAD). The bifurcation lesions of first case was treated using two-stent strategies of DK culotte, excellent angiography results was observed. The last two cases were treated using simple provisional stenting strategy: one stent was deployed crossover the ostium of the anomalous coronary artery, final angiographic results were excellent. These cases are extremely rare. We bring forth them in an attempt to highlight their significance, and make cardiologist to understand what important the anomalies are, and the strategy how to treatment these bifurcation lesions.
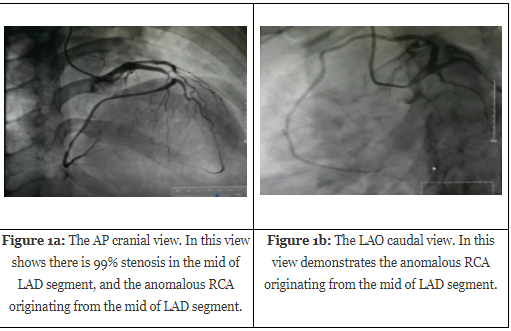
Case 1. A 47-year-young man was admitted to the cardiology department with chest pain for two hours companied with sweating after exertion. His coronary risk factors were hypertension, hyperlipidemia and ex-smoker. Physical examination was normal. Electrocardiography (ECG) showed ST elevation 0.2-0.4mv in leads V1-4. Echocardiography showed normal left ventricular systolic function without regional wall motion abnormality. Coronary angiography was performed through trans-radial access, and only a solitary ostium could be cannulated, which give off left main coronary artery (LMCA), left anterior descending (LAD) artery, left circumflex (LCX) artery, and an anomalous right coronary artery (RCA) originating from the mid of LAD segment (Figure 1a, 1b). The single coronary artery anomaly was classified as type [4] L-II A. The left main coronary artery was patent, but there was 99% stenosis in the mid segment of LAD, and LCX was normal. There was 50% stenosis in the ostium of anomalous RCA which originating from the mid of the LAD artery was a dominant (Figure 1a-c).
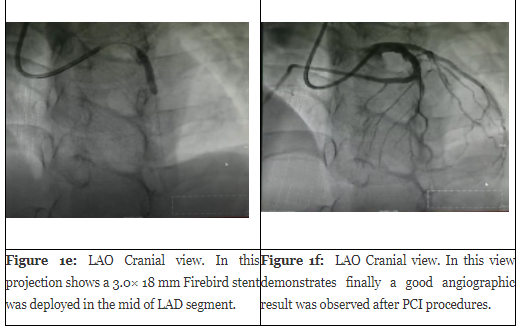
Based on coronary angiogram findings, the decision was made to proceed with percutaneous coronary interventions (PCI) of the bifurcation lesions to the mid of LAD and the ostium of anomalous RCA using DK-culotte stenting strategy. A 7 Fr sheath was inserted through right radial artery, and the left coronary ostium was engaged with an 7 Fr EBU 3.5 guiding catheter. Two 0.0014 inch balance middle weight (BMW) wires were inserted into the LAD and the anomalous RCA artery. We pre-dilated the LAD and the ostium of anomalous RCA using a 2.5×15-mm Quantum Maverick RX balloon (Boston Scientific Corporation, USA). Thereafter, we deployed a 3.0× 23 mm Firebird (MicroPort Medical Corporation, Shanghai, China) stent to LAD-RCA lesions. Adjunctive post-stenting balloon dilatation was done using a 2.5×15-mm Quantum Maverick RX balloon at mid LAD and a Quantum Maverick RX balloon 3.0×15-mm at the LAD-RCA. We performed DK culotte crushing with a 3.0× 18 mm Firebird (MicroPort Medical Corporation, Shanghai, China) stent at the mid LAD. Additional kissing ballooning was performed using a Quantum Maverick RX balloon 3.0×15-mm at LAD-RCA and a post-stenting balloon Firebird 3.0× 18 mm at the mid LAD. Finally a good angiographic result was seen (Figure. 1d-f).

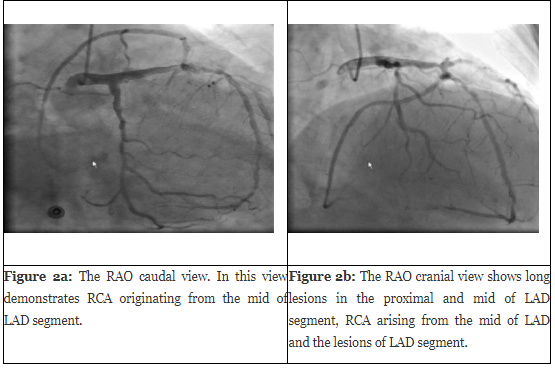
Case 2. A 74-year-old woman presented with a history of progressive angina pectoris for 3 months, she suffered from diabetes mellitus and hypertension for ten years. Coronary angiogram was performed through trans-radial approach. The coronary angiography results showed nonobstructive ostial LMCA and diffuse LAD disease extending from the proximal to the mid segment. The left circumflex artery (LCX) was long lesions in the proximal segment, and the anomalous right coronary artery (RCA) originating from the mid of LAD was patent (showed in figure 2a, 2b).
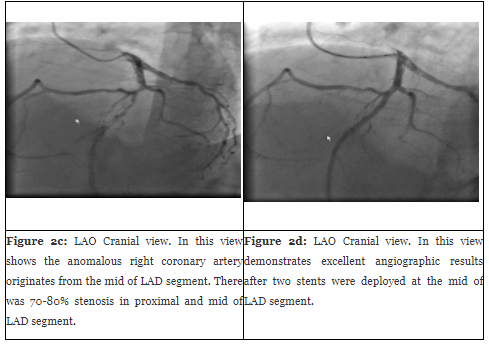
Based on coronary angiography findings, the decision was made to proceed with percutaneous coronary interventions (PCI) to the proximal and mid LAD and LCX. A 6Fr EBU 3.5 guiding catheter was used to engage the left coronary system. A 180-cm balance middle weight (BMW) wire was used to cannulate the LAD, and the other BMW was used to cannulate the anomalous RCA to protect it. The proximal and mid LAD lesion was predilated with a 2.0-× 20-mm Maverick 2 balloon (Boston Scientific Corporation, Natic, MA, USA) at 12 atm. A 2.5-× 30 mm Endeavor (Medtronic Corporation, Minneapolis, MN, USA) stent was implanted at the mid LAD segment, and a 3.0-× 23 mm Firebird (MicroPort Medical Corporation, Shanghai, China) stent, it crossed over the anomalous RCA, was deployed at the proximal LAD at 14 atm, jailing the wire in the RCA. The mid LAD stent appeared to be underexpanded, so it was postdilated with a 3.0-×12-mm Quantum Maverick RX balloon (Boston Scientific Corporation, USA) up to 14 atm. Finally a good angiographic result was observed, and the ostium of anomalous RCA originating from the mid of LAD is not affected (see figure 2c-d).
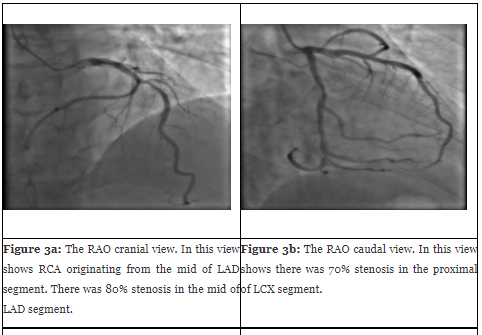
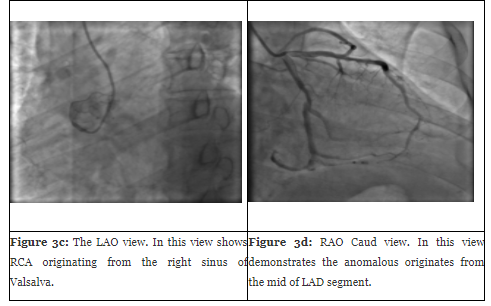
Case 3. A 54-year-old man was admitted with effort chest pain for three months. His coronary risk factors were hypertension and history of ex-smoking. The echocardiography showed normal left ventricular function (EF=54%) without regional wall motion abnormality. The physical exam was normal. The ECG showed T-wave inversion in leads V1-4 and chest x-ray was normal. Coronary angiography was performed through trans-radial access. Left coronary angiography showed the left main coronary was normal. There was 80% stenosis at the mid LAD segment, while LCX 70% stenosis in the proximal segment. The anomalous right coronary artery originating from the mid of LAD segment (Figure. 3a-d)
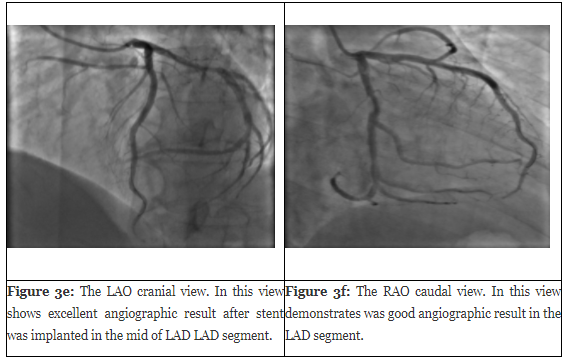
According to coronary angiography findings, the decision was made to proceed with percutaneous coronary interventions (PCI) of the bifurcation lesions to the mid of LAD. A 6Fr Jukin’s 3.5 guiding catheter was used to engage the left coronary system. A 180-cm balance middle weight (BMW) wire was used to cannulate the LAD, and the other runthrough (NS) wire was used to cannulate the anomalous RCA to protect it. The mid of LAD lesions was predilated with a 2.5-× 15-mm Maverick 2 balloon (Boston Scientific Corporation, Natic, MA, USA) at 12 atm. A 3.0-× 30 mm Resolute (Medtronic Corporation, Minneapolis, MN, USA) stent was implanted at the mid LAD segment, it crossed over the anomalous RCA, was implanted at the mid LAD at 14 atm. Finally a good angiographic result was observed (Figure. 3e-f ).
Discussion
Congenital anomalies of coronary arteries (CAAS) are very rare and usually documented as an incidental finding during routine catheter or CT angiography performed for other reasons. Their prevalence ranges from 0.2% to 1.3% based published series [1-4]. The most common coronary artery anomaly is origination of the left circumflex coronary (LCX) artery from the proximal of right coronary artery (RCA) or right sinus of Valsalva. The second is separate origination of the left anterior descending coronary artery (LAD) and LCX artery from the left sinus of Valsalva. The third is the anomalous right coronary artery (RCA) originating from the aortic trunk of ascending artery or left sinus of Valsalva. When the anomalous right coronary originates from the mid of left anterior descending coronary artery, it is called single coronary artery (SCA) [2], its prevalence is less than 0.024% [3]. The anomalous coronary artery is first designated with "R" or "L" depending upon whether the ostium is located in the right or left sinus of Valsalva. It is then designated as group I, II, III. Group I has anatomical course of either a right or left coronary artery. Group II anomalies arise from the proximal part of the normal right or left coronary artery, and cross the base of the heart before assuming the normal position of the inherent coronary artery. Group III describes the anomaly where the LAD and LCX arise separately from the proximal part of the normal right coronary artery [4]. Herein, we presented three extremely rare cases of anomalous RCA detected incidentally during routine coronary angiography. The first case is the anomalous RCA arising from the mid of left anterior descending coronary artery (LAD). The bifurcation lesions was treated using DK culotte stent technique, finally excellent angiographic results were observed (Figure. 1f). The last two cases are treated using simple provisional stent technique: single stent placement covering the the side branch. Final good angiographic results were obtained (Figure. 2d, 3f). All the cases are belongs to L-IIA subtypes according to Lipton’s classification [3].
Despite advances in the field interventional cardiology, the optimal stenting technique for bifurcation disease remains the subject of debate. Bifurcation disease accounts for 15-20% of coronary interventions. According to the 2011 American College of Cardiology (ACC) guidelines, provisional side branch stenting should be the initial strategy (class I recommendation) when the side branch is not large and has only mild to moderate ostial disease, while elective side branch stenting is reasonable (class IIA) if the side branch is large with a high risk of occlusion and the likelihood of side branch reaccess is low [5]. The case we present is that the anomalous right coronary originates from the mid of left anterior descending coronary artery, and the bifurcation lesions were treated using simple provisional stent or two-stent strategy (DK-culotte), final excellent angiography results were observed. The case is extremely rare, so we bring forth them to attempt their significant in our clinical practice [6].
Coronary anomalies are usually detected during coronary angiography. However, X-ray angiography is limited by its inability to provide information regarding the spatial orientation of the anomalous artery with regarding to the surrounding cardiovascular structures [6,7,8]. MSCT coronary angiography has proven to be effective not only in the identification and characterization of coronary artery disease, but also in the evaluation of the anatomical coronary details, and clearly demonstrate the surrounding cardiovascular structures of the anomalous coronary artery.
Conflict of interest
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
