
Research Article | DOI: https://doi.org/10.31579/2578-8965/248
Pelvic Rehabilitation Medicine Clinical Research Foundation, West Palm Beach, FL, USA
*Corresponding Author: Katherine Wolfrum, Pelvic Rehabilitation Medicine Clinical Research Foundation, West Palm Beach, FL, USA.
Citation: Allyson Shrikhande, Lolasri Rampally, Katherine Wolfrum, Jasmine Ross, Gautam Shrikhande, (2024), Significant Improvement Noted in Vulvodynia when Pelvic Neurogenic Inflammation is Addressed, J. Obstetrics Gynecology and Reproductive Sciences, 8(8) DOI:10.31579/2578-8965/248
Copyright: © 2024, Katherine Wolfrum. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 October 2024 | Accepted: 05 November 2024 | Published: 12 November 2024
Keywords: vulvodynia; pelvic pain; chronic pelvic pain; pelvic floor muscle dysfunction; levator ani myalgia; sexual intercourse; intercourse pain; female sexual dysfunction
Synopsis/Brief Summary
Vulvodynia is effectively treated by the PRM Protocol™, which improves pain, function, and quality of life in patients with chronic pelvic pain.
Objective: Vulvodynia, characterized by chronic pain and/or discomfort around the opening of the vulva, is known to affect up to 16% of adult women and may present as constant or intermittent pain that negatively impacts patients’ personal and working lives, as well as mental health and relationships. This study aimed to test the effectiveness of a multimodal neuromuscular treatment protocol in treating chronic pelvic pain and vulvodynia symptoms and improving pain and function.
Methods: 59 patients ages 20-79 presented to an outpatient clinic with pelvic pain and Vulvodynia symptoms. These symptoms had, on average, persisted for 6 years. All patients underwent a once-weekly, six-week treatment (the PRM Protocol) consisting of ultrasound-guided pelvic floor musculature trigger-point injections and peripheral nerve blocks. To measure the effects of this treatment, a 0-10 Visual Analogue Scale (VAS) was used to measure pelvic pain intensity, and the Functional Pelvic Pain Scale (FPPS) was used to measure function across multiple areas. These measures were taken on patients’ first visit to a clinic and three months after treatment began.
Results: VAS scores improved by an average of 51%. Before treatment, the mean VAS score was 7.93 (SD=1.61) (a=0.05; CI 7.52-8.34), and the posttreatment mean VAS score was 3.9 (SD=2.19) (a=0.05; CI 3.34-4.46) (P<0.0001). Pelvic pain functionality improved by 23% after three months. Pretreatment FPPS scores averaged at 12.34 (SD=5.8) (a=0.05; CI 10.86-13.82), decreasing to 9.53 (SD=5.43) (a=0.05; CI 8.14-10.91) after treatment (P<0.0001). FPPS functions that showed the most significant improvement were Sleep, which improved by 39%; Intercourse, which improved by 28%; and Walking, which improved by 28%.
Conclusions: These results indicate that a six-week treatment consisting of once-weekly ultrasound-guided pelvic floor musculature trigger-point injections and peripheral nerve blocks combined with once-weekly pelvic floor physical therapy was very effective at relieving pain and improving function for patients with Vulvodynia. Significant reductions in opiate use, ER visits, and pain interference at work were observed following treatment.
Vulvodynia is known to affect up to 16% of women [1]. It is described as vulvar pain at least 3 months in duration in nonsexual and/or sexual situations without a clearly identifiable cause1. It is a diagnosis of exclusion [1]. Vulvodynia is classified into two main subtypes by location of pain. Provoked vestibulodynia (PVD), which is the most common subtype, is provoked pain localized to the vaginal vestibule [2]. Generalized vulvodynia (GVD) is unprovoked, diffuse vulvar pain that affects the entire vulvar area [3]. Examination for vulvodynia often involves the cotton swab test (Q Tip Test), which is the standard test for PVD [4]. The cotton swab test involves palpation of several genital regions with a cotton swab tip and assessing the level of pain at each region [4].
The etiology of vulvodynia is unknown. There have been suggestions that vulvodynia stems from complex interactions of peripheral and central pain mechanisms, as well as psychological, behavioral, genetic, and musculoskeletal factors [4]. Further, chronic inflammation, genetic immune factors, and hormonal changes may also play a role in the development of vulvodynia [5].
Vulvodynia has a significant personal and societal burden due to its adverse widespread effects on women’s quality of life as well as their partners. Patients with PVD can avoid sex due to the length of lingering pain, which can last for hours to days after touch or sexual intercourse. Additionally, women may not be able to participate in routine exercise or activities such as wearing tight clothing or riding a bicycle due to the pain [5]. Furthermore, women with vulvodynia often seek many healthcare providers before receiving a diagnosis and treatment [1]. Due to this, women with vulvodynia may feel marginalized and frustrated by the healthcare system. Medical management of vulvodynia should be multidisciplinary.
Medical treatment for vulvodynia frequently involves cognitive behavioral therapy, pelvic floor physical therapy, and behavioral modifications such as guided imagery. Pharmacological interventions for vulvodynia can include botulinum type A, corticosteroids, local anesthetics such as lidocaine, and oral neuropathic pain agents [3].
Since there is limited research concerning the efficacy of vulvodynia treatment, this study tested the efficacy of an outpatient, comprehensive, neuromuscular treatment protocol aimed at treating the myofascial pain and dysfunction, peripheral sensitization, and central sensitization seen in female vulvodynia patients.
87 patients aged 18 – 79 (Figure 1) who had been previously diagnosed with Vulvodynia were included in this study. These patients presented to an outpatient pelvic rehabilitation practice between April 2021 and December 2022. For these patients, Vulvodynia symptoms persisted for an average of 6 years. Patient demographics and clinical characteristics are depicted in Figures 1, 2, 3, 4, and 5.
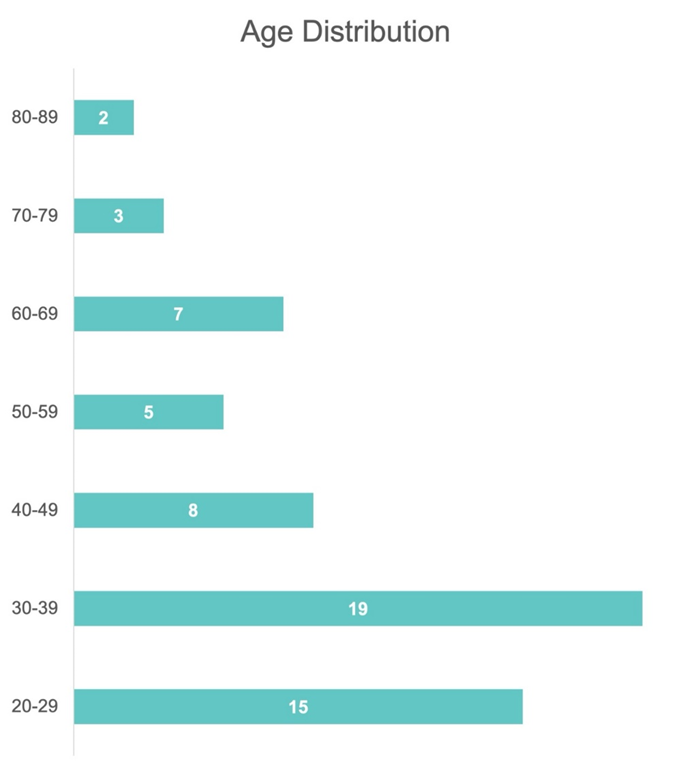
Figure 1: Age Distribution of Patients
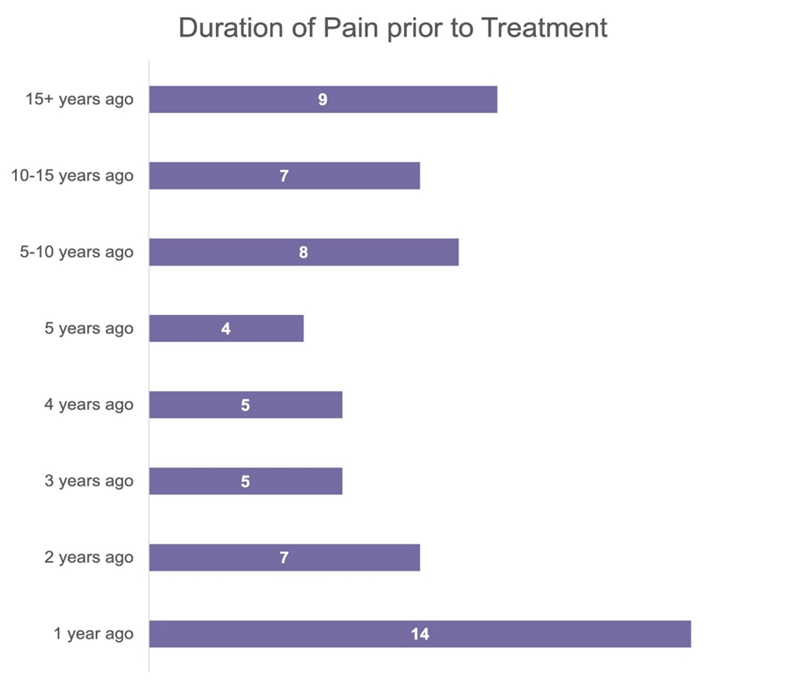
Figure 2: Patient duration of pain before the PRM Protocol™ treatment
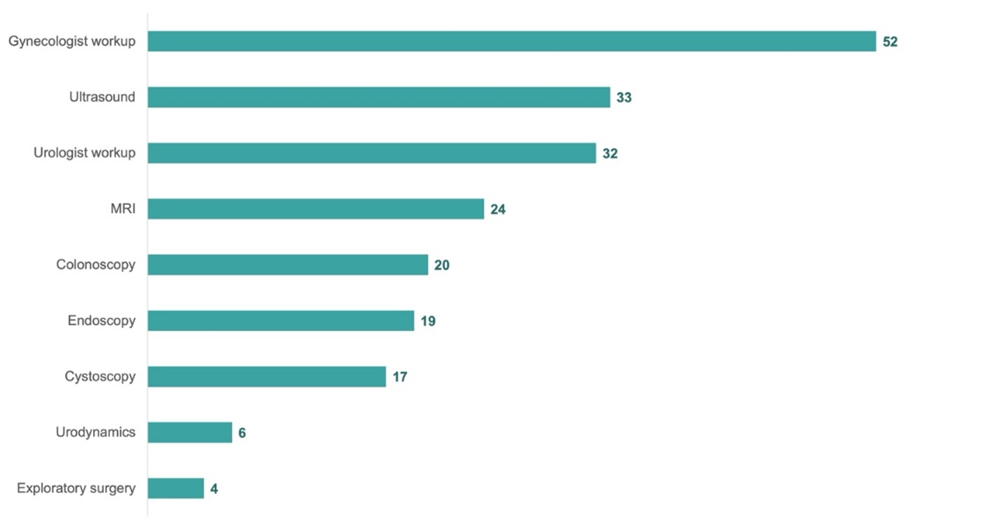
Figure 3: Patient clinical treatments and examinations before the PRM Protocol™ treatment
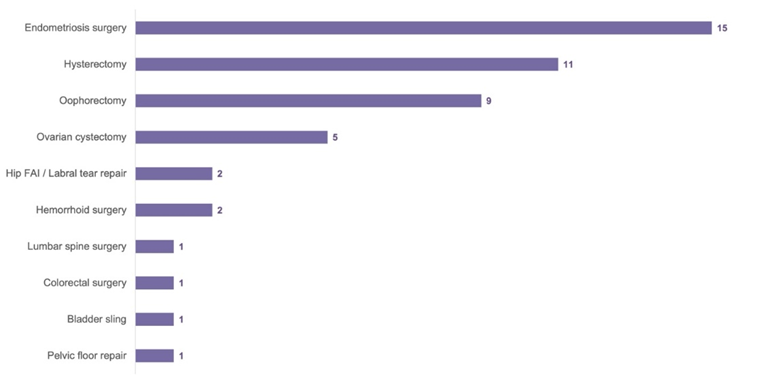
Figure 4: Patient surgical procedures before the PRM Protocol™ treatment
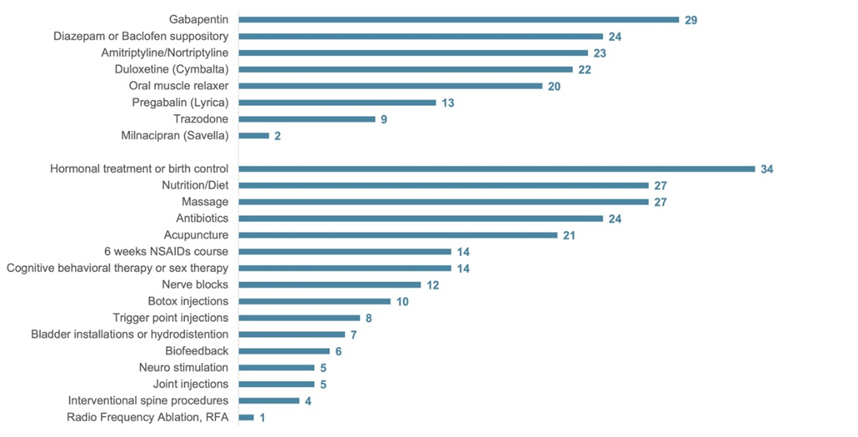
Figure 5: Population frequency use of medications and treatments before the PRM Protocol™ treatment
Patients were eligible for this retrospective chart review if they met the following inclusion criteria:
- Completion of a Full Gynecological examination with necessary workup
to exclude other causes of vulvar pain, including lichen sclerosis and infection
- Completion of 6 weeks of pelvic floor physical therapy
- Completion of an external ultrasound guided by office-based pelvic peripheral nerve block and trigger point injection series protocol, or the non-completion of this protocol.
- Completion of an internal examination with a positive cotton swab Test (Q Tip Test)
- Trigger points, pelvic floor hypertonia, and tenderness upon palpitation of levator ani sling on internal examination
- Tenderness along the pudendal nerve and posterior femoral cutaneous nerve at Alcock's canal and obturator canal bilaterally internally
Patients were excluded from the retrospective chart review if any of the following were present:
- Active infection
- Malignancy
- Pregnancy
- Pudendal nerve entrapment syndrome
- Incomplete Patient Reported Outcome measures
The protocol for this research project was approved by a suitably constituted Ethics Committee of the institution, and it conforms to the provisions of the Declaration of Helsinki. Committee of The Feinstein Institutes for Medical Research, Approval No. IRB# 17-0761. Our study does not have a clinical trial number, and consent forms were waived due to study design.
This IRB-approved (IRB# 17‐0761) treatment was designed for patients whose symptoms persisted after participating in pelvic floor physical therapy. Prior to each procedure, patients were pre-medicated with diclofenac 75 mg PO and a topical anesthetic spray.
Patients underwent unilateral, once-weekly ultrasound‐guided pelvic peripheral nerve blocks. In the prone position, a pudendal nerve block at Alcock's canal was performed using 2 ml of dexamethasone with 7 ml of 1% Lidocaine on the initial visit, and normal saline was used instead of the dexamethasone for subsequent nerve blocks. Patients simultaneously underwent external ultrasound‐guided trigger point injections using Lidocaine 1% to the pelvic musculature. A global injection was administered into the iliococcygeus, pubococcygeus, or puborectalis one side at a time, treating every muscle of the levator ani sling once throughout the six weeks of treatment. A flexible, 6‐inch, 27‐gauge needle injected the specific muscle from the subgluteal posterior approach, using an aseptic technique under ultrasound guidance with the patient lying in the prone position. On ultrasound, myofascial trigger points look like focal, hypoechoic zones with lowered vibration amplitude on vibration sonoelastography, suggesting a local, rigid nodule [19].
Then, in the supine position, a nerve block of the posterior femoral cutaneous nerve 4 cm inferior to the ischial tuberosity was performed with 2 ml of dexamethasone and 5 ml of 1% Lidocaine on the initial visit. The dexamethasone was substituted with normal saline in subsequent visits.
Patients resumed normal activities and returned to work the same day after sitting on ice for 10 minutes.
Participant response to treatment was measured 6 weeks after their final injection appointment. The primary outcome measures are a visual analog scale (VAS) score to calculate pelvic pain concentration and functional pelvic pain scale (FPPS) scores to measure pelvic functionality. Patients reported their mean pain intensity from 1-10 during the previous 24 hours for the VAS score. The total FPPS score adds subs-cores from each of the following categories: working, intercourse, sleeping, walking, running, lifting, bladder, and bowel. Each category is scored 0-4, where 0 represents average performance and 4 denotes significant debilitation, resulting in a total FPPS score from 0-32.
Secondary outcome measures include a modified NIH Sexual Function Profile (SFP), which consists of three questions concerning sexual well-being totaled for an overall Modified SFP score. Absenteeism and Presenteeism questionnaires, as well as the patient-reported frequency of opioid use and Emergency Room (ER visits), are utilized for a more well-rounded account of a patient’s well-being.
A retrospective medical records review was conducted to analyze the above outcome measures. VAS, FPPS, and SFP scores were analyzed using a Wilcoxon signed-rank test for paired samples due to their non-normal distribution. Differences in Absenteeism and Presenteeism were tested using a Chi-squared test, and changes in opioid use and ER Visits were tested using a McNemar test for paired proportions. Statistical analyses were performed in SPSSv.29, using a cutoff of α = 0.05.
Statistically significant results were achieved across several outcome variables. A 1-10 VAS (Visual Analog Scale), FPPS (Functional Pelvic Pain Scale), a modified SFP (Sexual Function Profile), Opioid use, Emergency Room visits, Absenteeism, and Presenteeism were measured at participants’ initial appointment (Before Treatment) and their appointment held 3 months after their first injection (After Treatment). Results for the statistical tests outlined above can be seen in Figures 6, 7, 8, 9, and 10.
VAS pain levels decreased by 50% from a Before Treatment average of 7.96 (SD 1.61; α = 0.05, CI = 7.59-8.33) to an After Treatment average of 3.99 (SD 2.3; α = 0.05, CI = 3.46-4.52) (p< .001) (Figure 6). FPPS total scores decreased by 26% from an average of 11.49 (SD 6.38; α = 0.05, CI = 10.03-12.96) to an average of 8.55 (SD 5.50; α = 0.05, CI = 7.29-9.81) (p< .001) (Figure 6). Improvements in all FPPS categories were statistically significant (p < .001), with the largest decreases in Sleep (38% improvement), Intercourse (35% improvement), and Walking (28% improvement) (Figure 7).
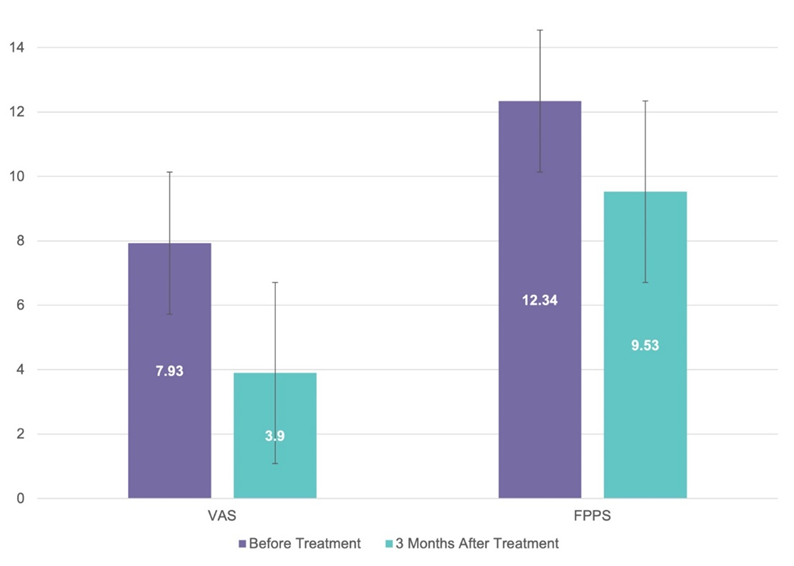
Figure 6: VAS and FPPS scores were measured at participants’ initial appointment (Before Treatment), and their appointment was held 3 months after their first injection (After Treatment).
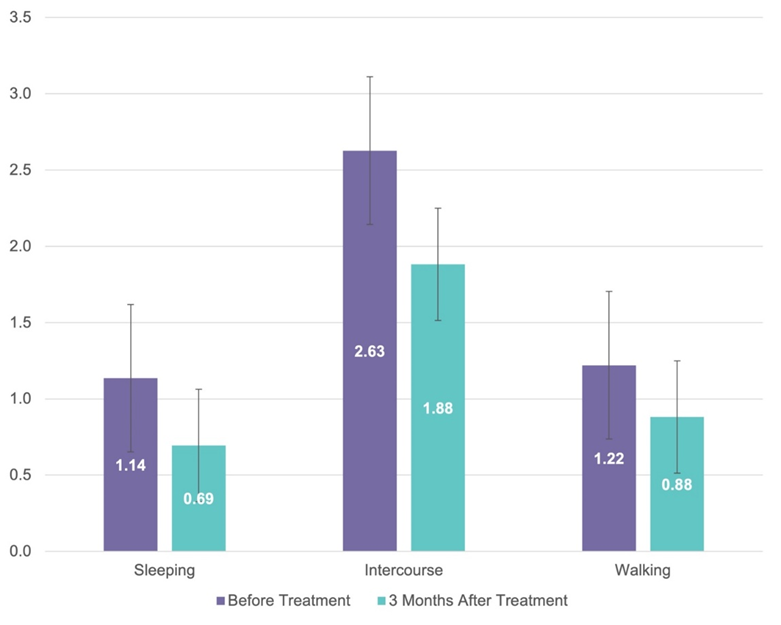
Figure 7: FPPS scores in the categories of Sleeping, Intercourse, and Walking were measured at participants’ initial appointment (Before Treatment) and their appointment held 3 months after their first injection (After Treatment).
Our modified SFP asked the following three questions: “In the past 30 days, how would you describe the comfort of your vagina during sexual activity?” “In the past 30 days, how often have you had difficulty with sexual activity because of discomfort/ pain in your vagina?” and “In the past 30 days, how often have you stopped sexual activity because of discomfort/ pain in your vagina?” Responses were scored 0-5 and summed for an average improvement of 23% (P=0.0406) (Figure 7,8).
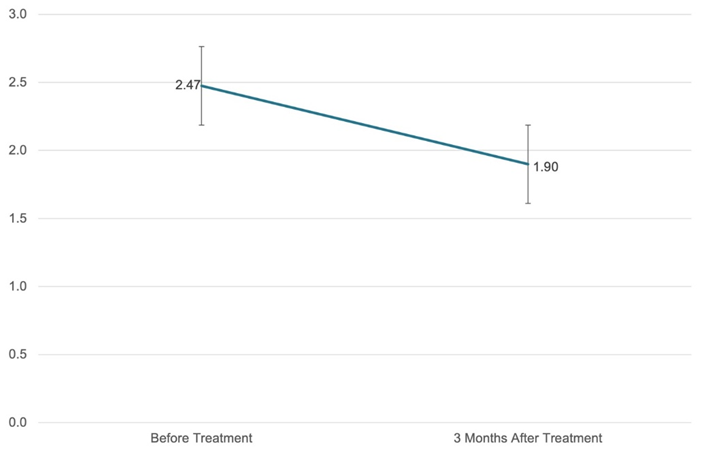
Figure 8: Modified Sexual Function Profile (SFP) measured at participants’ initial appointment (Before Treatment) and their appointment held 3 months after their first injection (After Treatment).
Opioid use for pelvic pain decreased by 64% for patients (Figure 9). Before Treatment, 8% of patients reported having gone to the Emergency Room for pelvic pain recently (Figure 9). 0 patients had gone to the Emergency Room 3 months After Treatment (Figure 9).
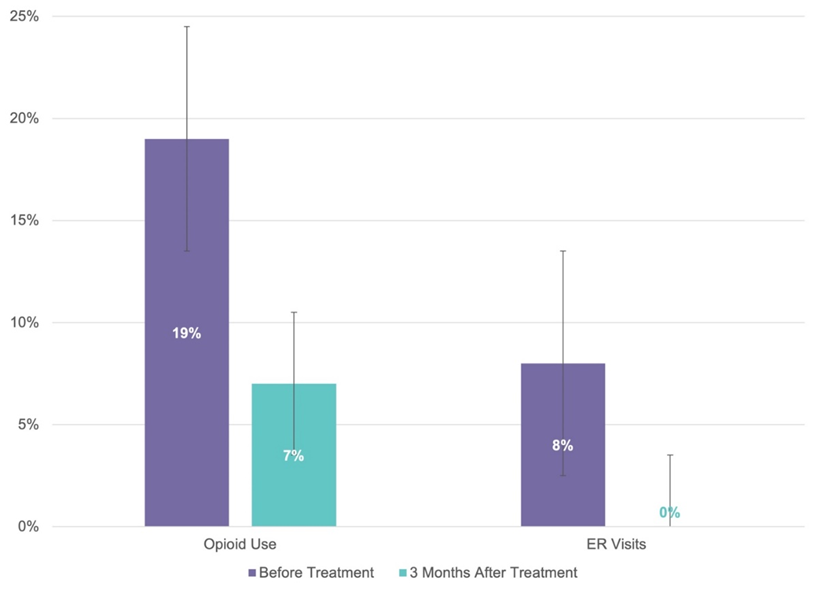
Figure 8: Opioid Use and ER Visits were measured at participants’ initial appointment (Before Treatment), and their appointments were held 3 months after their first injection (After Treatment).
Absenteeism, defined by at least one day of work missed in the past 3 months due to pelvic pain, decreased by 53% (Figure 10). Presenteeism, represented by at least 1 hour of work productivity being disturbed by pelvic pain in the past 3 months, reduced by 67% (Figure 11).
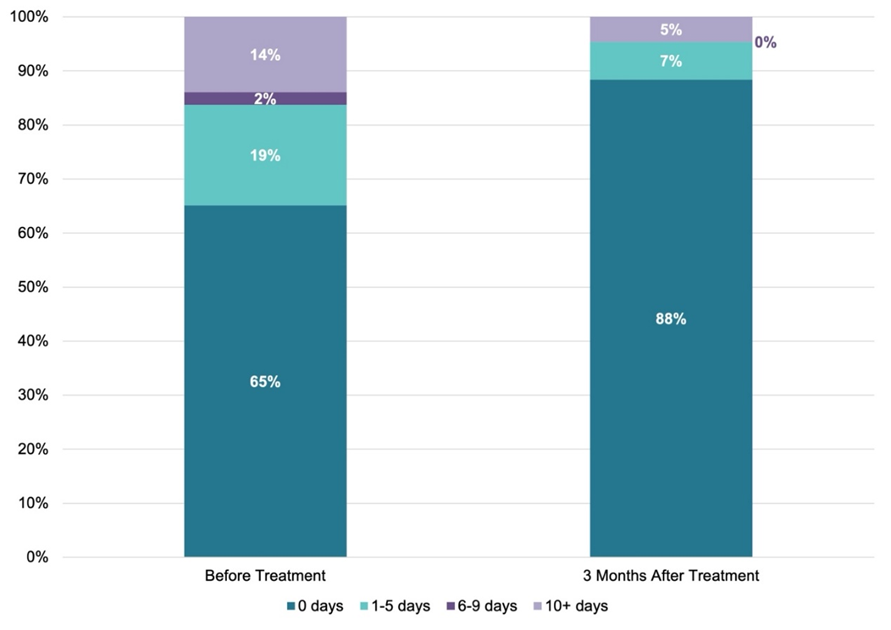
Figure 9: Absenteeism was measured at participants’ initial appointment (Before Treatment), and their appointment was held 3 months after their first injection (After Treatment).
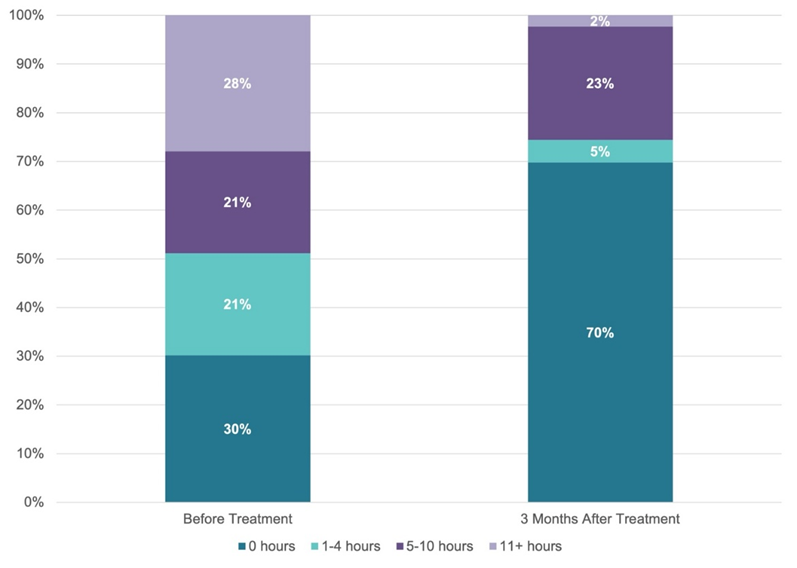
Figure 10: Presenteeism was measured at participants’ initial appointment (Before Treatment), and their appointment was held 3 months after their first injection (After Treatment).
This paper studied the effect of a multimodal protocol involving office-based ultrasound‐guided pelvic peripheral nerve blocks of the pudendal nerve and the posterior femoral cutaneous nerve, trigger point injections to the pelvic floor musculature, and pelvic floor physical therapy to treat Vulvodynia in the setting of CPP and a hypertonic pelvic floor. The paper aimed to capture the effect of this protocol on a wide variety of outcome parameters, including pain, function, work productivity, quality of life, mental health, sexual health, and healthcare system utilization. The average duration of pain for the 87 participants in this study was 6 years. 81% of participants had tried specialized treatments for vulvodynia in the past (in addition to the 6 weeks of pelvic floor physical therapy necessary for inclusion in the study), and 15% of participants had undergone surgery or procedures for vulvodynia-related pain. Productivity measured by Absenteeism and Presenteeism variables is inversely correlated with pain as measured by VAS, demonstrating that vulvodynia-related pain significantly impacts patients’ careers. As evidenced by the Before Treatment values across all outcome measures, vulvodynia patients experience hardship due to pain in every area of life.
The outpatient protocol examined in this study simultaneously targets the underlying pain and dysfunction in both the myofascial and nervous systems seen in vulvodynia patients with the goal of rehabilitation. Statistically significant improvements in VAS pain levels and FPPS function were found for participants, demonstrating the effectiveness of addressing underlying nerve and muscle dysfunction and applying the concept of neuroplasticity to vulvodynia [4,6]. Myofascial dysfunction seen in the pelvis is related to bowel, bladder, and sexual dysfunction, and it creates pelvic pain from myofascial trigger points. Treating this underlying myofascial pain and pelvic floor dysfunction with ultrasound‐guided trigger point injections to each muscle of the levator ani sling will remove the source of ongoing nociception as well as create space for the pelvic peripheral nerves to flow with less constriction and increased blood flow [8]. Peripheral sensitization is addressed using serial peripheral nerve blocks along the pudendal and posterior femoral cutaneous nerves; protocol (1) decreases neurogenic inflammation by placing dexamethasone locally to deplete substance P9 and with repetitive exposure to lidocaine 1%, which decreases the mast cell release of histamine and (2) desensitizes hyperactive peripheral nociceptors with repetitive exposure to lidocaine 1% [10]. Central sensitization is addressed by treating associated pelvic neurogenic inflammation, thus inhibiting the feedback loop from the peripheral nervous system to the central nervous system [11]. The overlap in pain patterns and innervation between the pudendal and posterior femoral cutaneous nerves leads to cross‐sensitization. This phenomenon is known to occur in the pelvis, where a sensitized structure can upregulate an adjacent, normal structure [12]. Consequently, the protocol treats both peripheral pelvic nerves simultaneously to inhibit cross‐sensitization.
The most significant improvements were seen with intercourse, sleeping, and bladder symptoms. As our protocol directly treats the pelvic nerve inflammation and pelvic muscles involved with intercourse and vulvodynia, reversing the pelvic neurogenic inflammation and hypertonic pelvic floor results in less vulvar pain and improved function with intercourse. There is evidence that vulvodynia and bladder pain syndrome/interstitial cystitis often overlap [13]. The proposed connection between vulvodynia and BPS/IC suggests that pain hypersensitivity is mediated by peripheral and central sensitization [18]. Therefore, it makes sense that bladder symptoms would improve along with the vulvodynia symptoms as our protocol addresses the associated peripheral and central sensitization [20]. Through pelvic organ cross-sensitization and bladder neuroplasticity, there is the possibility that pudendal nerve irritation can induce increased activity of bladder C-fiber afferent pathways, which is reportedly involved in the development of OAB [14]. Therefore, reversing the peripheral neurogenic inflammation around the pudendal nerve and simultaneously releasing a hypertonic pelvic floor will ultimately decrease bladder symptoms in CPP patients. Lastly, our protocol has proven to help patients with vulvodynia in the setting of CPP and a hypertonic pelvic floor achieve sleep, most likely due to a combination of decreasing their pelvic pain as well as decreasing nocturia as their bladder symptoms resolve [15]. Improvements were minimal in both walking and running for our male patients, secondary to the fact that their initial VAS and FPPS scores were also very low before treatment, leaving little room for improvement. Once pelvic pain symptoms are improved, they can regain their quality of life.
Vulvodynia patients are often underdiagnosed and undertreated as there is a lack of awareness, understanding, simple diagnostics, and treatment options in the medical community [1,4,16]. Therefore, they find themselves being bounced around the medical ecosystem, going to the Emergency Room when the pain is severe [17], undergoing many unnecessary diagnostic procedures, as well as many unsuccessful therapeutic surgical and non-surgical treatments. As a medical community, it would be best for the patient and the healthcare system to create a streamlined diagnostic and treatment protocol for vulvodynia.
Concerning their vulvodynia-related pain, patients were asked to report the number of days of work they had missed in the past 3 months (Absenteeism) and the number of hours of work productivity negatively affected in the past 3 months (Presenteeism). After the outpatient protocol, the number of participants who had missed any number of hours or days due to vulvodynia was reduced by two-thirds. These drastic improvements in both outcome measures add to the evidence that vulvodynia significantly impairs patients' careers and demonstrate the outpatient protocol's positive effect on patients’ working lives.
The study has a few notable limitations, the first of which is that the retrospective nature does not allow for randomized control groups. We cannot assess the effectiveness of our protocol against placebo control groups as we would intentionally not be treating control group vulvodynia patients who are seeking relief from their pain. However, our results are statistically significant across five validated measures for pain, function, and quality of life, showing that patients saw significant improvement in pain, function, and quality of life.
To conclude, our study reported statistically significant results for our comprehensive, outpatient neuromuscular protocol in patients aged 17–78 who had been diagnosed with vulvodynia. The most significant improvements were seen in overall pain level, intercourse, sleeping, bladder function, social participation, and anxiety. Significant decreases in opioid use, ER visits, and pain interference at work were also found after the treatment.
The authors report no conflicts of interest in this work.
All authors contributed to the design and implementation of the research, the analysis of the results, and the writing of the manuscript. All authors provide permission to submit this paper and agree they have had the opportunity to review its contents.
The study was performed at Pelvic Rehabilitation Medicine in Atlanta, Chicago, Dallas, Houston, Miami, New York City, New Jersey, Michigan, and Washington, D.C. Patient data were gathered from these clinics.
This research received no external funding.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
