
case report | DOI: https://doi.org/10.31579/2690-1897/197
1Department of Urology, St John of God Subiaco Hospital, Perth WA.
2Department of General Surgery, St John of God Midland Hospital, Perth WA.
*Corresponding Author: Vivien Hsu, SJOG Subiaco Hospital 12 Salvado Road Subiaco 6008 Western Australia.
Citation: Vivien Hsu, Ruwan Wijesuriya, (2024), Should cross-sectional imaging be performed prior to surgery for painful incarcerated hernias?, J, Surgical Case Reports and Images, 7(5); DOI:10.31579/2690-1897/197
Copyright: © 2024, Vivien Hsu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 May 2024 | Accepted: 30 May 2024 | Published: 07 June 2024
Keywords: diverticulitis; hernia; incarcerated hernia; cross-sectional imaging
The role of imaging in assessment of patients presenting with acutely painful hernias is unclear to date. Traditionally, patients presenting acutely to the Emergency Department (ED) with painful incarcerated hernias are operated on after the initial clinical assessment and imaging is rarely warranted in the work-up. We present three cases of hernias presenting with clinical features of incarceration. Two underwent cross-sectional imaging which showed diverticulitis of the sigmoid colon within the sac without vascular compromise or obstruction, and were managed conservatively during the initial hospital visit then operated on electively for hernia repair with good outcomes. The third patient proceeded to surgery after imaging and was found to have an inflamed sigmoid colon which was inadvertently entered during surgery, resulting in a laparotomy and Hartmann’s procedure. These cases suggest that perhaps there is a role for imaging in the assessment of acutely painful hernias suspected to be incarcerated, and patients with suspected incarcerated hernia may benefit from cross-sectional imaging to avoid potentially difficult operations in the acute stage or minimize complications.
CRP – C-reactive protein
CT – computerised tomography
ED – Emergency Department
IV – intravenous
MRI – magnetic resonance imaging
US – ultrasonography
WCC – white cell count
Traditionally, patients presenting acutely to the Emergency Department (ED) with incarcerated hernias are operated on after the initial clinical assessment without any cross-sectional imaging performed. The underlying rationale is that irrespective of the contents of the hernia, it is considered a surgical emergency and must be acted upon urgently without delay from further investigations as delay is associated with greater morbidity [1]. However, with the increasing incidence of diverticular disease, there seems to be more patients presenting with acute diverticulitis where on occasion, the sigmoid colon could be located within a left sided inguinal or ventral hernia, mimicking incarceration [2-5]. In this report, we identify three such cases of acute diverticulitis occurring within hernias, and will discuss the role of imaging in guiding management of these presentations.
An 84-year-old man presented with a four-week history of left lower quadrant abdominal pain associated with nausea. He denied any vomiting, fevers or associated anorexia. There were no bowel changes noted. His past medical history included hypertension, hypothyroidism, previous aortic dissection, prostate cancer and duodenal ulcer.
On examination, the patient had a soft abdomen with no peritonism but some tenderness in the left lower quadrant. In addition, a left-sided inguinal hernia was palpable and tender. The patient had noticed a painless swelling in this region prior to presentation, however was reporting significant pain on the day of admission.
Laboratory investigations showed a white cell count (WCC) within normal limits at 10.9x109/L and a mildly elevated CRP level at 54.9. A CT-abdomen ordered by the patient’s GP prior to presentation to ED showed sigmoid colon diverticulitis with the area of diverticulitis occurring at the efferent loop of large bowel within a large fat and bowel-containing left-sided indirect inguinal hernia without signs of acute bowel obstruction (Figure. 1).
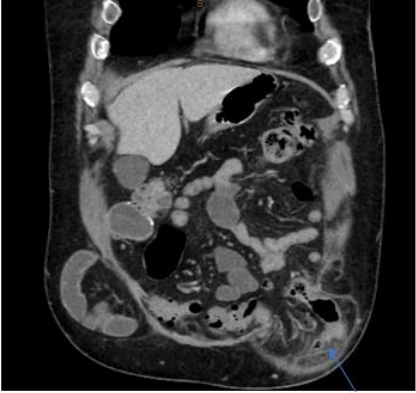
Figure 1: Coronal view of CT-abdomen/pelvis showing incarcerated left-sided inguinal hernia
A 48-year-old man presented with sudden onset abdominal pain associated with a known ventral hernia for which he was awaiting surgical repair. He reported associated nausea, but no vomiting, fevers, or altered bowel habits. His past medical history included a laparoscopic appendicectomy converted to an open right hemicolectomy, repair of an incarcerated umbilical hernia and an incisional hernia repair.
On examination, there was obvious protrusion of a large ventral hernia from a previous midline laparotomy. The hernia was tender and not reducible. Laboratory investigations showed WCC within normal limits at 10.5x109/L and a mildly elevated CRP of 20.5. CT-abdomen showed sigmoid diverticulitis within a large ventral hernia with no evidence of bowel obstruction or ischaemia (Figure. 2).

Figure 2: Axial view of CT-abdomen/pelvis showing incarcerated ventral hernia
Both of these patients were managed conservatively with regards to the hernia and the acute uncomplicated diverticulitis of the sigmoid colon. They were commenced on intravenous (IV) antibiotics and kept nil by mouth for bowel rest with IV fluids for treatment of the diverticulitis. Pain was well-controlled with ongoing analgesia during admission, with improvement of inflammatory markers throughout. Both patients recovered well after a few days of antibiotic therapy with pain resolving. The hernias were easily reduced by the time of discharge with settling inflammation of the sigmoid colon.
A 92-year-old female from home alone presented with a painful left groin mass. She denied any nausea and vomiting or associated fevers, and bowels were opening normally. Her past medical history included ischaemic heart disease, atrial fibrillation, diverticular disease, congestive heart failure, previous deep vein thrombosis, hysterectomy and cholecystectomy.
On examination, the abdomen was soft with generalised left-sided tenderness. A firm, tender swelling was palpable in the left inguinal region which was not able to be reduced. Laboratory investigations showed a normal WCC of 9.0x109/L and mildly elevated CRP of 23. CT-abdomen showed appearances suggestive of a left inguinal hernia containing a loop of small bowel, suspicious for an incarcerated hernia (Figure. 3).
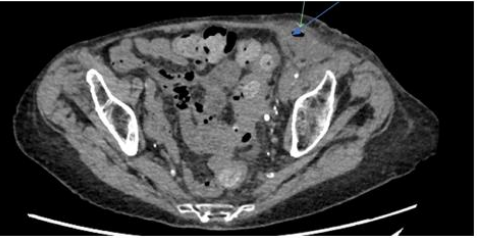
Figure 3: Axial view of CT-abdomen/pelvis showing left-sided inguinal hernia with localised perforation
The patient went on to have a laparoscopic exploration of the groin which revealed no hernia. However, a sinus tract with chronic changes communicating with peritoneal cavity was found. Upon further exploration, the sigmoid colon was found to be very inflamed and adherent to the sinus with a hard mass palpable, thought to be colonic diverticulitis. The sigmoid colon was technically difficult to separate from the hernia sac, and during the process a contained perforation sealed off by the hernia sac and omentum was revealed. As it was deemed unsafe to return the sigmoid colon to the abdominal cavity, the decision was made to proceed to a Hartmann’s procedure through a midline laparotomy and a loop colostomy formed. The operation was complicated by necrotising fasciitis of the hernia site resulting in further debridement and significant morbidity.
Abdominal hernias are a common cause of abdominal pain and intestinal obstruction, and a number of abdominal contents can protrude through these abdominal wall defects including peritoneal fat, the greater omentum and bowel loops [6-8]. The most common complications of abdominal wall hernias are bowel obstruction, incarceration and strangulation, all of which can present with acute pain [6].
Historically, imaging is rarely warranted in the diagnosis of hernias and their complications as the history and physical examination alone are usually sufficient for making the diagnosis [6-8]. One study reports a sensitivity and specificity of 75% and 96% respectively for physical examination in diagnosing hernias [6]. As such, acutely painful hernias are not often further investigated with imaging following the initial clinical assessment. This can perhaps lead to misdiagnoses and result in untreated alternative pathologies associated with the hernia. The cases presented in this report highlight the possibility of a concurrent pathology such as diverticulitis of the colon which also requires treatment, and suggests that there is perhaps a role for imaging in the assessment and diagnosis of painful abdominal wall swellings.
The role of imaging in assessment of patients presenting with acutely painful hernias is unclear to date. Imaging may be required when the clinical presentation is inconclusive or unclear to distinguish between hernias and their complications or other abdominal pathologies. There are various different modalities which can be used to confirm the diagnosis of hernias or suspected complications of hernias such as obstructions or incarcerations [1, 3].
Ultrasonography (US) is at times used in the outpatient setting for diagnosis of groin hernias, with studies reporting a sensitivity of >90% and specificity of 82-86% in detecting groin hernias [6]. When used to assess hernias, US can show features such as expansion of fluid-filled bowel, and slightly echogenic, long, strip-shaped omentum in the hernia sac [9]. By contrast, it can distinguish between a hernia and lymphadenopathy by showing an internal echo in lymphadenopathy [3]. In addition, occurrence of hernia incarceration can be detected by observation of the blood supply in the hernia contents with colour Doppler US [3,9].
Plain film X-rays have very limited use in assessment of hernias but can be useful in identifying other pathologies such as bowel obstruction (9). Magnetic resonance imaging (MRI) has been reported to have a high sensitivity and specificity of >95% in differentiating between inguinal and femoral hernias [7,8], but limited literature exists on its role in assessment of acutely painful hernias and excluding incarceration or other pathologies.
By far the most commonly used modality in assessment of acutely painful hernias which present to ED is CT, due to its many advantages. Its speed in imaging acquisition, ability to obtain three-dimensional data sets and multi-planar reformation makes it a valuable tool in assessing intra-abdominal pathology and detecting subtle signs of complications. High-resolution axial CT allows for visualisation of the abdominal wall defect, and hernia sac and its contents, and any complications associated with the hernia [1]. In particular, enhanced scans with oral iodinated contrast can determine whether the hernia sac contents are intestinal, the type of intestine involved, and the presence the bowel strangulation. Further to this, CT can be useful in distinguishing hernias from more sinister masses of the abdominal wall such as tumours, haematomas, abscesses, undescended testes or aneurysms [1,3].
Abdominal wall hernias are a frequent finding in the abdomen, both on clinical examination and on imaging, and although most are asymptomatic, they can be associated with complications which require urgent surgery. In considering the three cases discussed in this report, imaging was obtained in the assessment of all three patients and was useful in determining the diagnosis and guiding management. This suggests that perhaps there is a role for imaging in the assessment of acutely painful hernias suspected to be incarcerated, and perhaps CT scans should be more routinely utilised for these presentations.
None
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
